
The first thing you notice at the American Psychiatric Association meeting is its size. By conservative estimates, a quarter of the psychiatrists in the United States are packed into a single giant San Francisco convention center, more than 15,000 people.
Being in a crowd of 15,000 psychiatrists is a weird experience. You realize that all psychiatrists look alike in an indefinable way. The men all look balding, yet dignified. The women all look maternal, yet stylish. Sometimes you will see a knot of foreign-looking people huddled together, their nametags announcing them as the delegation from the Nigerian Psychiatric Association or the Nepalese Psychiatric Association or somewhere else very far away. But however exotic, something about them remains ineffably psychiatrist.
The second thing you notice at the American Psychiatric Association meeting is that the staircase is shaming you for not knowing enough about Vraylar®.
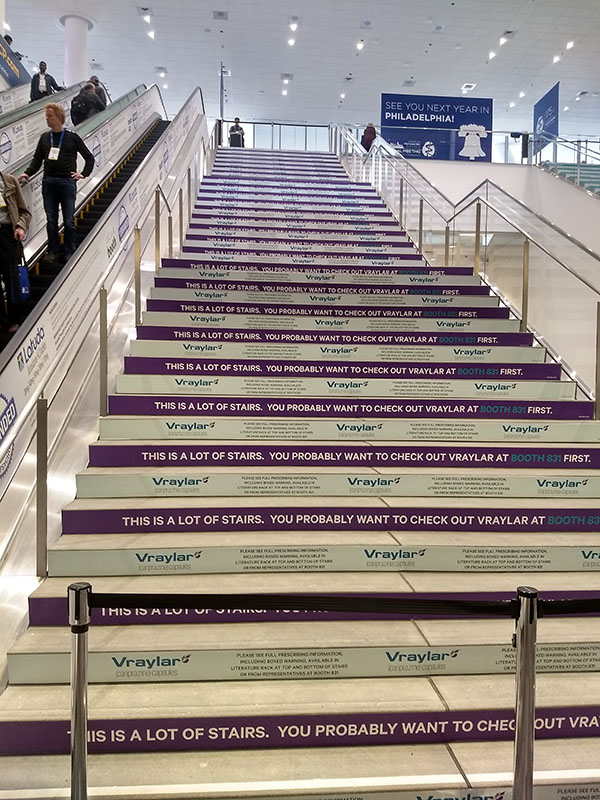
Seems kind of weird. Maybe I’ll just take the escalator…

…no, the escalator is advertising Latuda®, the “number one branded atypical antipsychotic”. Aaaaaah! Maybe I should just sit down for a second and figure out what to do next…

AAAAH, CAN’T SIT DOWN, VRAYLAR® HAS GOTTEN TO THE BENCHES TOO! Surely there’s a non-Vraylar bench somewhere in this 15,000 person convention center!

…whatever, close enough.
You know how drug companies pay six or seven figures for thirty-second television ads just on the off chance that someone with the relevant condition might be watching? You know how they employ drug reps to flatter, cajole, and even seduce doctors who might prescribe their drug? Well, it turns out that having 15,000 psychiatrists in one building sparks a drug company feeding frenzy that makes piranhas look sedate by comparison. Every flat surface is covered in drug advertisements. And after the flat surfaces are gone, the curved sufaces, and after the curved surfaces, giant rings hanging from the ceiling.
The ads overflow from the convention itself to the city outside. For about two blocks in any direction, normal ads and billboards have been replaced with psychiatry-themed ones, until they finally peter off and segue into the usual startup advertisements around Market Street.

There’s a popular narrative that drug companies have stolen the soul of psychiatry. That they’ve reduced everything to chemical imbalances. The people who talk about this usually go on to argue that the true causes of mental illness are capitalism and racism. Have doctors forgotten that the real solution isn’t a pill, but structural change that challenges the systems of exploitation and domination that create suffering in the first place?
No. Nobody has forgotten that. Because the third thing you notice at the American Psychiatric Association meeting is that everyone is very, very woke.
Here are some of the most relevant presentations listed in my Guidebook:
| Saturday, May 18 |
| Climate Psychiatry 101: What Every Psychiatrist Should Know |
| Women's Health In The US: Disruption And Exclusion In The Time Of Trump |
| Gender Bias In Academic Psychiatry In The Era Of the #MeToo Movement |
| Revitalizing Psychiatry – And Our World – With A Social Lens |
| Hip-Hop: Cultural Touchstone, Social Commentary, Therapeutic Expression, And Poetic Intervention |
| Lost Boys Of Sudan: Immigration As An Escape Route For Survival |
| Treating Muslim Patients After The Travel Ban: Best Practices In Using The APA Muslim Mental Health Toolkit |
| Making The Invisible Visible: Using Art To Explore Bias And Hierarchy In Medicine |
| Navigating Racism: Addressing The Pervasive Role Of Racial Bias In Mental Health |
| . |
| Sunday, May 20 |
| Addressing Microaggressions Toward Sexual And Gender Minorities: Caring For LGBTQ+ Patients And Providers |
| Latino Undocumented Children And Families: Crisis At The Border And Beyond |
| Racism And Psychiatry: Growing A Diverse Psychiatric Workforce And Developing Structurally Competent Psychiatric Providers |
| Sex, Drugs, And Culturally Responsive Treatment: Addressing Substance Use Disorders In The Context Of Sexual And Gender Diversity |
| Grabbing The Third Rail: Race And Racism In Clinical Documentation |
| Racism And The War On Terror: Implications For Mental Health Providers In The United States |
| The Multiple Faces Of Deportation: Being A Solution To The Challenges Faced By Asylum Seekers, Mixed Status Families, And Dreamers |
| What Should The APA Do About Climate Change? |
| Intersectionality 2.0: How The Film Moonlight Can Teach Us About Inclusion And Therapeutic Alliance In Minority LGBTQ Populations |
| Transgender Care: How Psychiatrists Can Decrease Barriers And Provide Gender-Affirming Care |
| Gun Violence Is A Serious Public Health Problem Among America's Adolescents And Emerging Adults: What Should Psychiatrists Know And Do About It? |
| Working Clinically With Eco-Anxiety In The Age Of Climate Change: What Do We Know And What Can We Do? |
| Are There Structural Determinants Of African-American Child Mental Health? Child Welfare – A System Psychiatrists Should Scrutinize |
| . |
| Monday, May 21 |
| Community Activism Narratives In Organized Medicine: Homosexuality, Mental Health, Social Justice, and the American Psychiatric Association |
| Disrupting The Status Quo: Addressing Racism In Medical Education And Residency Training |
| Ecological Grief, Eco-Anxiety, And Transformational Resilience: A Public health Perspective On Addressing Mental Health Impacts Of Climate Change |
| Immigration Status As A Social Determinant Of Mental Health: What Can Psychiatrists Do To Support Patients And Communities? A Call To Action |
| Psychiatry In The City Of Quartz: Notes On The Clinical Ethnography Of Severe Mental Illness And Social Inequality |
| Racism And Psychiatry: Understanding Context And Developing Policies For Undoing Structural Racism |
| Trauma Inflicted To Immigrant Children And Parents Through Policy Of Forced Family Separation |
| Deportation And Detention: Addressing The Psychosocial Impact On Migrant Children And Families |
| How Private Insurance Fails Those With Mental Illness: The Case For Single-Payer Health Care |
| Imams In Mental Health: Caring For Themselves While Caring For Others |
| Misogynist Ideology And Involuntary Celibacy: Prescription For Violence? |
| Advocacy: A Hallmark Of Psychiatrists Serving Minorities |
| Inequity By Structural Design: Psychiatrists' Responsibility To Be Informed Advocates For Systemic Education And Criminal Justice Reform |
| Treating Black Children And Families: What Are We Overlooking? |
| Blindspotting: An Exploration Of Implicit Bias, Race-Based Trauma, And Empathy |
| But I'm Not Racist: Racism, Implicit Bias, And The Practice Of Psychiatry |
| No Blacks, Fats, or Femmes: Stereotyping In The Gay Community And Issues Of Racism, Body Image, And Masculinity |
| Silence Is Not Always Golden: Interrupting Offensive Remarks And Microaggressions |
| Black Minds Matter: The Impact Of #BlackLivesMatter On Psychiatry |
…you get the idea, please don’t make me keep writing these.
Were there really more than twice as many sessions on global warming as on obsessive compulsive disorder? Three times as many on immigration as on ADHD? As best I can count, yes. I don’t want to exaggerate this. There was still a lot of really meaty scientific discussion if you sought it out. But overall the balance was pretty striking.
I’m reminded of the idea of woke capital, the weird alliance between very rich businesses and progressive signaling. If you want to model the APA, you could do worse than a giant firehose that takes in pharmaceutical company money at one end, and shoots lectures about social justice out the other.
The fourth thing you notice at the American Psychiatric Association meeting is the Scientologists protesting outside.

They don’t tell you they’re Scientologists. But their truck has a link to CCHR.org on it, and Wikipedia confirms them as a Scientology front group. Scientology has a long-standing feud with psychiatry, with the psychiatrists alleging that Scientology is a malicious cult, and the Scientologists alleging that psychiatry is an evil pseudoscience that denies the truth of dianetics. And that psychiatrists helped inspire Hitler. And that the 9/11 was masterminded by Osama bin Laden’s psychiatrist. And that psychiatrists are plotting to institute a one-world government. And that psychiatrists are malevolent aliens from a planet called Farsec. Really they have a lot of allegations.
This particular truck is especially sad, because they’re reinforcing the myths about electroconvulsive therapy. ECT is a very effective treatment for depression. It is essentially always consensual – although most other psychiatric treatments can be administered involuntarily if someone is judged too out-of-touch with reality to make decisions, ECT has a special status as a treatment which can only be given with patient permission. It’s always performed under anaesthesia and muscle relaxants, so patients are not conscious during the procedure and not spasming. And it can be a life-changing option for treatment-resistant depression. See this Scientific American article for more.
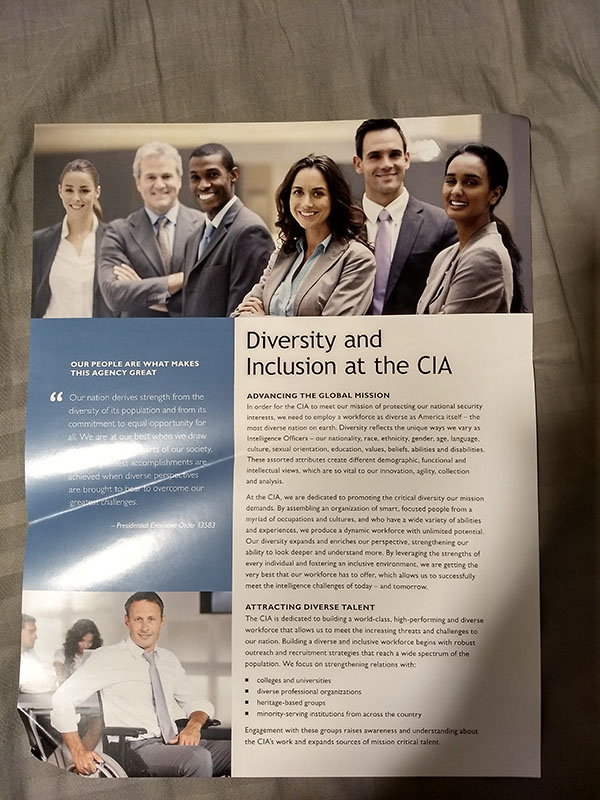
The fifth thing you notice at the American Psychiatric Association meeting is that the CIA has set up a booth.

I was pretty curious about what the CIA wanted from psychiatrists (did they lose the original MKULTRA data? do they need to gather more?), but I was too shy to ask their representative directly. I did take one of their flyers, but it turned out to just be about how woke they were:
The sixth thing you notice at the American Psychiatric Association meeting is that Vraylar® has built an entire miniature city. The buildings are plastered with pamphlets on Vraylar®. Billboards advertising Vraylar® hang over the streets and bridges. Giant Vraylar balloons hover serenly over everything, looking down with contempt and sorrow upon the non-Vraylar®-prescribing world below.

Occupying pride of place in city center, some sort of Important Vraylar Scientist is constructing the Transamerica Pyramid out of playing cards.

I dunno, if I were working in an area where the research supporting a treatment has a tendency to collapse suddenly and spectacularly, I might want to avoid building an association in people’s minds between my medication and a house of cards. But the ways of Vraylar® are inscrutable to mortal men.
The seventh thing you notice at the American Psychiatric Association meeting is that many of the new drugs are ridiculous.
It’s hard to blame pharmaceutical companies for this. The return on investment for pharma R&D is rapidly shrinking – drug discovery is too expensive to consistently make money anymore.
Rather than give up and die, pharma is going all in on newer, me-too-er me-too drugs. The current business plan looks kind of like this:
1. Take an popular older drug
2. Re-invent it, either with a minor change to the delivery mechanism, or by finding a similar molecule that works the same way
3. Call this a new drug, advertise the hell out of it, and sell it for 10x – 100x the price of the older drug
4. Profit!
Consider Lucemyra®:
It’s an alpha-2a receptor agonist used to treat acute opiate withdrawal. Alpha-2a receptor agonists are a fine choice for acute opiate withdrawal, but we already have one that works great: clonidine. Clonidine costs $4.84 per month. Lucemyra® costs $1,974.78. Is there any difference at all between the two medications? Some studies suggest maybe lofexedine can cause less hypotension, but realistically we throw random doses of clonidine at ADHD kids all the time, so it’s not like clonidine-induced hypotension is some kind of giant menace which will destroy us all.
I asked the Lucemyra® representative why I might prescribe Lucemyra® instead of clonidine for opiate withdrawal. She said it was because Lucemyra® is FDA-approved for this indication, and clonidine isn’t. This is the same old story as Rozerem® vs. melatonin, Lovaza® vs. fish oil, and Spravato® vs. ketamine. As long as doctors continue to outsource their thinking to the FDA approval process, in a way even the FDA itself doesn’t endorse, pharma companies will be able to inflate the prices of basic medications by a thousand times just by playing games with the bureaucracy.
But also:

Jornay® is a new form of methylphenidate, ie Ritalin. The usual comparison: a month of Ritalin costs $25.19, a month of Jornay® costs $387.48. What’s the difference? You can take Jornay® at night. Why is this interesting? The Jornay® representatives say that maybe people want to have Ritalin in their system as soon as they wake up, rather than having to wait the half-hour or so it usually takes for it to start having an effect. I have to admit, from a scientific perspective Jornay® is kind of cool; I expect the pharmacologists who designed it had a lot of fun. But the oppressed people of the world haven’t exactly been crying out for Dark Ritalin. Nobody has been saying “Help us, pharmaceutical industry, merely having Ritalin®, Concerta®, Metadate®, Focalin®, Daytrana®, Quillivant®, Quillichew®, Aptensio®, Biphentin®, Equasym®, Medikinet®, and Rubifen® just isn’t enough for us! We need more forms of Ritalin, stat!”
My favorite was Subvenite®, which is just lamotrigine in a conveniently-packaged box that tells you how much to take each day. The same amount of normal lamotrigine would cost about $12; it’s hard for me to figure out exactly how much Subvenite® costs, but this site suggests $540. To be fair, lamotrigine is a really inconvenient drug whose dosing schedule often leaves patients confused. To be less fair, seriously, $540 for some better instructions? Get a life.
How do all these people keep doing it? What’s their business plan? Here’s a hint:
This is the brochure for Lucemyra®, the opiate withdrawal medication that costs $1,974.78. No patient is paying $1,974.78 for it. Patients are paying $25. And doctors sure aren’t paying $1,974.78. The way all these companies are getting away with it is because in Healthcaristan SSR, nobody ever pays for their own medication.
To a first approximation, doctors make purchasing decisions, but insurances cough up the money. Insurances have a few weapons to prevent doctors from buying arbitrarily expensive drugs, but they tend to back off in the face of magic words like “I believe this is medically necessary” or “This is the one the FDA approved”. So to fill in the missing pieces of the pharma strategy mentioned above:
1. Take an popular older drug
2. Re-invent it, either with a minor change to the delivery mechanism, or by finding a similar molecule that works the same way
3. Call this a new drug, advertise the hell out of it, and sell it for 10x – 100x the price of the older drug
4. Advertise it to patients (who don’t have to pay for it) and doctors (who definitely don’t have to pay for it), neither of whom care at all what price you’re setting.
5. Make sure doctors know the magic words they need to use to force insurance companies to pay for it.
6. Profit!
This has become so lucrative that pharma companies barely have to do any real research and development at all these days. The only genuinely exciting new drugs at the conference were Ingrezza® and Austedo®, both of which treat tardive dyskinesia – a side effect you get from having been on too many other psychiatric drugs. This is probably a metaphor for something.
The eighth thing you notice at the American Psychiatric Association meeting is that there’s a presentation called “Yer A Psychiatrist, Harry!”: Learning Psychiatric Concepts Through The Fictional Worlds Of Game Of Thrones And Harry Potter. I didn’t go. I realize I have failed you, my readers, but if I had to listen to ninety minutes of that, all the Vraylar® in the world would not be enough to maintain my sanity.
The ninth thing you notice at the American Psychiatric Association meeting is that, after winning last place in a head-to-head comparison of various antipsychotics, doing worse than drugs that cost less than 1% as much…
…Fanapt® (iloperidone) has pivoted to a marketing strategy of bribing doctors with free ice cream:

The tenth thing you notice at the American Psychiatric Association meeting is that all of this has happened before.
This is the 175th anniversary of the APA. It’s been a pretty crazy century-and-three-quarters, no pun intended. Like, seriously, take a look at this guy:
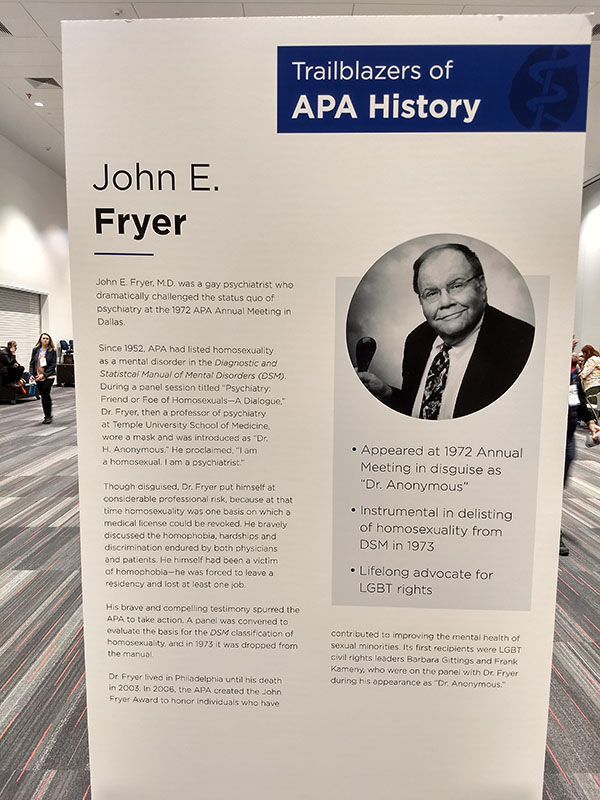
Back when you could still lose your medical license for being gay, he went to the APA meeting in a mask and gave a presentation arguing for gay rights, and the APA de-listed homosexuality as a psychiatric disorder the following year. How amazing is that?
The APA highlighted a bunch of people like this, heroes and trailblazers all. But for every great hero celebrated on posters, there is an embarrassment buried somewhere deep in an archive. My favorite of these is the APA Presidential Address from 1918, the very tail end of WWI. The head of the Association, a very distinguished psychiatrist named Dr. Anglin, gets up in front of the very same conference I attended this week (the 1918 version was held in Chicago) and declared that the greatest problem facing psychiatry was…the dastardly Hun:
The maxim that medical science knows no national boundaries has been rudely shaken by the war. The Fatherland has been preparing for isolation from the medical world without its confines. Just as, years ago, the Kaiser laid his ban on French words in table menus, so, as early as 19 14, German scientists embarked on a campaign against all words which had been borrowed from an enemy country. A purely German medical nomenclature was the end in view. The rest of the world need not grieve much if they show their puerile hate in this way. It will only help to stop the tendency to Pan-Germanism in medicine which has for some years past been gaining headway. ‘
The Germans excel all other nations in their genius for advertising themselves. They have proved true the French proverb that one is given the standing he claims. On a slender basis of achievement they have contrived to impress themselves as the most scientific nation. Never was there greater imposture. They display the same cleverness in foisting on a gullible world their scientific achievements as their shoddy commercial wares. The two are of much the same value, made for show rather than endurance — in short, made in Germany […]
In the earliest months of the war it was pointed out that there are tendencies in the evolution of medicine as a pure science as it is developed in Germany which are contributing to the increase of charlatanism of which we should be warned. A medical school has two duties — one to medical science, the other to the public. The latter function is the greater, for out of every graduating class 90 per cent. are practitioners and less than 10 per cent, are scientists. The conditions in Germany are reversed. There, there were ninety physicians dawdling with science to every ten in practice. Of these 90, fully 75 per cent were wasting their time. In Germany the scientific side is over-done, and they have little to show for it all, while the human side is neglected. Even in their new institutions, splendid as they are in a material sense, it is easily seen that the improved conditions are not for the comfort of the patients.
Out of this war some modicum of good may come if it leads to a revision of the exaggerated estimate that has prevailed in English-speaking countries of the achievements of the Germans in science. We had apparently forgotten the race that had given the world Newton, Faraday, Stephenson, Lister, Hunter, Jenner, Fulton, Morse, Bell, Edison, and others of equal worth. German scientists wait till a Pasteur has made the great discovery, on which it is easy for her trained men to work. She shirks getting for herself a child through the gates of sacrifice and pain ; but steals a babe, and as it grows bigger under her care, boasts herself as more than equal to the mother who bore it. Realising her mental sterility, drunk with self-adoration, she makes insane war on the nations who still have the power of creative thought.
But it is especially in the realm of mental science that the reputation of the Germans is most exalted and is least deserved. For every philosopher of the first rank that Germany has produced, the English can show at least three. And in psychiatry, while we have classical writings in the English tongue, and men of our own gifted with clinical insight, we need seek no foreign guides, and can afford to let the abounding nonsense of Teutonic origin perish from neglect of cultivation.
The Germans are shelling Paris from their Gothas and their new gun. Murdering innocents, to create a panic in the heart of France! With what effect ? The French army cries the louder, “They shall not pass ” ; Paris glows with pride to be sharing the soldiers’ dangers, and increases its output of war material; and the American army sees why it is in France, and is filled with righteous hatred. Panic nowhere. Vengeance everywhere. What does the Hun know of psychology? His most stupid, thick-witted performance was his brutal defiance of the United States with its wealth, resources, and energy. That revealed a mental condition both grotesque and pitiable.
After the war a centre of medical activity will be found on this side the Atlantic, and those who have watched the progress medical science has made in the United States will have no misgivings as to your qualifications for leadership. If we learn to know ourselves, great good will come out of this war.
Anglin does not deny that some may find it inappropriate to discuss politics at a psychiatry conference, but notes that:
If in these introductory remarks I have not been able to detach myself from the world’s most serious business at the present time, perhaps on reflection they may not have gone very far afield from the subject which binds us together in an association. If there is to be a change in the conditions under which we live this must have its effect on the minds of men ; whether for good or ill, I will not stop to speculate. We are intensely concerned with environment. This war itself is entangled with it,
England’s greatness, her devotion to honour, truth, and fidelity, is due to the environment in which her children are trained and grow to manhood. The ivy-grown wall, the vine-clad hills and the rose-covered bowers constitute the birth-place of English character.
Gerard tells us the cause of the war is the uncongenial environment in which the German youth is cradled and reared. The leaden skies for which Prussia is noted, its bleak Baltic winds, the continuous cold, dreary rains, the low-lying land, and the absence of flowers have tended to harden the spirit and rob it of its virtue, produce a sullen and morose character, curdling the milk of human kindness.
He does raise one warning, one problem that risks sabotaging even countries as congenial-climate-having as ourselves and our allies:
The quack medicine vendor is busier than ever. Money is plenty and he wants some of it. He uses mental suggestion and interests us. He is a specialist in distortion who probes into the ordinary sensations of
healthy people and perverts them into symptoms. Every billboard, newspaper, fence-rail, barn and rock thrusts out a suggestion of sickness as never before. The only vulnerable point to attack the vicious traffic is the advertising. If governments forbid that as they should, the next generation will be healthier and richer.
From Dr. Anglin’s address, I gather three things.
First, the billboards we shall always have with us. It’s easy to imagine this a modern problem, but apparently the generation that confronted the Kaiser was confronting annoying psychiatric advertising too. The Kaiser is gone; the annoying psychiatric advertising has proven a tougher foe.
Second, psychiatry has always been the slave of the latest political fad. It is just scientific enough to be worth capturing, but not scientific enough to resist capture. The menace du jour will always be a threat to our mental health; the salient alternative to “just forcing pills down people’s throat” will always be pursuing the social agenda of whoever is in power; you will always be able to find psychiatrists to back you up on this.
But third, science advances anyway. Psychiatry is light-years ahead of where it was a hundred years ago. Since Dr. Anglin’s 1918 address, we’ve discovered psychotherapy and psychopharmacology; come up with deinstitutionalization and destigmatization; and put rights in place to protect psychiatric patients and to protect the general public from being unnecessarily psychiatrized. We’ve even invented Vraylar®.
On my way out of the conference, I encountered this ad:

I don’t think it was even related to the psychiatry conference. I think it was for a nearby art museum. But it struck me. It struck me because it’s the sort of picture psychiatry wants to have of itself, a combination of hard neuroscience and basic human goodness. It struck me because as written, it’s obviously bogus (which Brodmann area is responsible for empathy again? How bright does it have to light up before you start feeling empathic?) in much the same way psychiatry can be obviously bogus (how much Vraylar® does it take before you can “take back control of your life” or “feel better than well”?), but is sort of an exaggerated and slightly-too-literal version of something that could potentially not be bogus. It struck me because, after making fun of it, I had to admit to myself that the thing it was pointing at was good and important and probably exactly what an art museum should be trying to do. And a psychiatrist, for that matter.

















”
But the oppressed people of the world haven’t exactly been crying out for Dark Ritalin. Nobody has been saying “Help us, pharmaceutical industry, merely having Ritalin®, Concerta®, Metadate®, Focalin®, Daytrana®, Quillivant®, Quillichew®, Aptensio®, Biphentin®, Equasym®, Medikinet®, and Rubifen® just isn’t enough for us! We need more forms of Ritalin, stat!””
I don’t take Ritalin and don’t have ADD. I take Adderrall for hypersomnolence (I have a hard time waking up, sleep more than normal, and have little energy waking). But I can’t tell how many times I’ve been asked to describe the difference I’ve observed and have to qualify the answer with “obviously, it only helps after I’ve woken up and taken it. Doesn’t do anything about how long I sleep in the first place.
So I dunno about Dark Ritalin, but Dark Adderrall sounds like it could theoretically be a nice thing.
Reading this post over again, I think the first two points can be summarized by:
1) Who makes money off of psychiatrists?
2) Who do psychiatrists make money off of?
In case (1), the big money flow is psychiatrists directing payments from insurers to pharma companies. Of course, everybody knows this..
Case (2) is more interesting. I suspect the convention is heavily weighted toward the more financially successful psychiatrists, and those are likely to be the ones with a good portfolio of private-pay patients. Those are going to be heavily weighted with well-educated upper-middle-class “professionals”, which is the class that is producing the trend of wokeness. So one way to look at all those seminars is not as an expression of psychiatric wokeness but a training program for the attitudes psychiatrists need to project to make their affluent patients feel good and/or a guide to the social pressures that those patients are most worried about.
Wow. I’m not an anxious person at all, but reading about this convention was pretty rattling. Thanks for helping me appreciate my dry engineering niche that will (hopefully) forever be insulated from woke politics.
You may not be interested in war…
… …
Oh, you poor sweet summer child.
As a person that takes ritalin from time to time: having a ~8 hour delay on the time release would be amazing
I frequently forget to take it when i wake up. and the time-release is long enough that if i take it when i remember at noon, i’ll be up until 4am.
this would give one chance to take it at night/evening, which i find easier to remember things. and if i had one of the other ones, i’d also have a second chance in the morning
also, i’d still be on today’s ritalin when taking tomorrow’s pill! that’s going to make me much more likely to remember to take it!
The advertising of prescription medications has started to hit home hard for my family and seeing the discussion here is very interesting. I do wonder how big the gender disparity of the result is. What percentage of men vs women are on prescription medication at any one time? Probably 5x or more women?
I have a family who is dealing with endometriosis. Endometriosis is increasingly well known largely thanks to the advertising of the drugs Lupron and Orilissa. Lupron is a disaster for endometriosis patients. I have had a hard time tracking down the entire history, but at some point there was a court order blocking public release of just how much data related to it was falsified. Orilissa may be better, though has been linked to several cases of permanent ovarian failure and no benefits that are better than normal birth control pills.
The effective treatment, so far as we can tell, is surgery by a skilled surgeon. But that is very much not what the medical industry is set up to provide. The endo community is now almost thankful for useless Orilissa, because fewer people are being given disastrous Lupron by doctors who have been “educated” by the pharmaceutical industry.
And that’s one disease!
Seeking information about endo has led us to some really depressing corners of the internet where retired nurses are trying to tell people the best course of medical action, because the doctors and governments won’t. Even sadder, you see story after story of women who finally found a hormonal birth control pill that worked for them with tolerable side effects, only to lose access to it – often because a “generic equivalent” entered the market. And then these women have terrible side effects and miss work and lose a bit of themselves and contribute to all the stereotypes about the unreliable female employee.
So all these posts, psychiatry focused as they are, are really interesting to me. Yay big pharma, messing up so many lives but paying for a conference where the attendees get to talk to each other about all the lives that are being messed up by big pharma.
i love this, you are right on!
I get a few hits but no dedicated Twitter account or blog.
Your move, Atlas!
Aside from the fact that every placebo controlled trial ever done for ECT has failed, sure, ECT is very effective. Anyone who expresses confidence in ECT clearly does not believe in science.
Or you know, actually had ECT after years of med resistant bipolar depression and credits it with saving their life.
I suspect like many psychiatric treatments it works really well sometimes and not at all in others so randomized trials don’t work out that well. On the other hand it has pretty bad side effects (usually significant memory loss) and I can’t imagine too many people stay on it if they don’t get a benefit.
Personal experience suggests that doctors are if anything too unwilling to consider it as an option, so I’m pretty confident that attempts to further stigmatize and sensationalize the treatment are doing more harm than good.
Are you trying to explain away rthorat’s claim? Maybe you should first assess if it is true.
I believe he has an empirical study of one that suggests a good reason for that one person to believe in the efficacy of ECT.
Also the original claim about ECT doesn’t seem correct to me, as I believe Scott has referenced good studies on it. (How do you placebo control ECT anyway)?
It’s under anaesthesia, right?
Oh, right, double blind wasn’t mentioned.
Still, you usually experience some pretty decent after effects of ECT.
https://power2u.org/wp-content/uploads/2017/01/1012-ReadBentallECT.pdf
Psychiatry stopped doing placebo trials after a half dozen or so came back negative. Suddenly, it was “unethical”. Tell me this: if ALL your placebo controlled trials are negative, how is it unethical to continue using anesthesia and placebo, but somehow ethical to continue using anesthesia + the “treatment” that has shown no efficacy and causes harm?
All the data ECT proponents cite to claim it has efficacy are NOT placebo controlled. They refuse to mention the placebo trials and if someone brings them up they will dismiss them by saying they are “old”. Today we use newer methods that are more effective. Of course, this is a lie. Today’s methods were developed to try to minimize the adverse effects. If they differ in efficacy from old methods, they are LESS efficacious (in reality, studies show they have the “same” efficacy because the efficacy is all just bias). There is NO evidence that current methods are more efficacious than older methods, which failed all placebo controlled trials.
rthorat may well be technically correct, but I care about RCT a lot more than I care that the control is a placebo.
Sorry I was unclear. When I talk of placebo controlled, I kind of assume randomization. But sure, I look for randomized, placebo controlled trials. And the placebo needs to be an appropriate placebo for the treatment.
I haven’t done exhaustive research on ECT or anything, but even a cursory look at meta-analyses of the efficacy of ECT suggest that there’s plenty of evidence that ECT is effective. What is your source for saying that “every placebo controlled trial ever done for ECT has failed”?
I have no dog in this hunt either way, in favor or against ECT. I just dislike seeing big claims like this made without some evidence to support them. Or suggesting that people who don’t agree with your claim are anti-science.
This is the definitive paper on ECT effectiveness: https://power2u.org/wp-content/uploads/2017/01/1012-ReadBentallECT.pdf
The research landscape has not changed since then, as psychiatry declared placebo controlled trials unethical for ECT right after half a dozen or so came back negative. If you cannot show efficacy, just ban the trials that remove the inherent bias. Voila, now you can pretend there is efficacy.
The placebo controlled trials mostly show no efficacy. A couple show efficacy immediately after treatment, but this is almost surely due to bias caused by blind breaking (patients who undergo ECT will have symptoms not seen in those who merely received placebo). In these trials, the advantage over placebo disappears at follow up – likely because blinds are no longer broken (remember, the doctor is the one rating symptoms, and they may not remember which patients had worse symptoms on follow up).
That’s a super interesting article about ECT, thanks for linking to it. I’m not sure I’d say it’s the definitive paper on ECT effectiveness. The BMJ printed a counter to this article you’ve linked to, and there are meta-analyses from this same year (2009-10) that show efficacy over placebo.
If this is your field of research, I yield to your superior knowledge. As best I can tell from the reading I’ve done on this in recent years, there’s a raging debate and research continues, much as it does about SSRIs.
Can you link the BMJ response? I am sure I have read it, but am not sure which you are talking about.
Of course there is a “raging debate”. There are massive entrenched interests that will protect their field at all costs. This always happens. But the defenders can only point to non-randomized and/or non placebo controlled trials. Or selectively present evidence about placebo controlled trials. Or refer to trials where patients did not receive anesthesia as “placebo”, when in fact they are “no treatment”. Read and Bentall is the definitive paper because it presents ALL the relevant evidence.
I’m adding ECT to the list of things I wouldn’t mind a 10,000 word Scottsplainer about.
I’m surprised at you, Scott, for saying that the Kaiser is gone. Quite the opposite – he has become a permanente fixture of medical care in America.
When I saw “Hun” I read it as the derogatory term for the women who sell MLM products.
And all the talk of advertising and quack medicine reinforced this for a while.
The second drug you mentioned being advertised was Latuda which Wikipedia states is “effectiveness in treating schizophrenic symptoms [is] … 13 to 15% less effective than ziprasidone, chlorpromazine, and asenapine”. And that others such as quetiapine and olanzapine “are known to possess antidepressant efficacy in bipolar disorder”.
So … why would anybody prescribe this as anything other than a 3rd or 4th tier drug?
Fabulous write-up of this conf! Scott, have you been reading about the carnivore diet (“eat what you are”) as a sure cure (pretty much) for depression, etc.? Mikhaila Peterson discusses it here: https://www.youtube.com/user/lowcarbdownunder/videos
ALL THE TALKS INCLUDING MIKHAILA’S
Worked for her father, Jordan Peterson, too.
FYI My father was a psychiatrist, educated at Harvard (class of 1950), ended up escaping the Big City (Mpls), buying a farm, raising beef cattle, & practicing at a mental health clinic in Fergus Falls, MN (one of the clinics brain-childed by JFK in his deinstitutionalization craze – there being a state hospital in FF – one of 2 in MN – so a mental health clinic actually did get built there). My father was not in favor of this mass deinstitutionalization – didn’t think it would end well & it hasn’t. The mental health clinics were supposed to “be there” for the now “free-range” mentally ill – but they ended up serving the much-better-heeled.
He was a believer in ECT (“shock therapy”) & said it was sometimes the ONLY thing that would work for older women in partic. for whom nothing else worked. I think it kind of “combs out your neurons.” 🙂 I also think it would be great for, say, soldiers coming back with PTSD.
I “agreed” to have ECT. It wiped out 25 years of memories and 27 IQ pts. It destroyed my life. It is repeated electrical craniocerebral trauma. Soldiers with PTSD and TBI blast injuries don’t need more brain damage.
Somatics, maker of ECT devices, just updated its machine manual to include “permanent amnesia and permanent brain damage” as risks.
Carnivore diet? Well, that explains the lobsters.
Let’s assume that Scientology is mostly what non-scientologists think it is, when they think about it at all.
But my thirdhand impression is that Scientology has, for whatever reason, glommed onto a number of surprisingly accurate insights about how the mind works.
Take ECT, for example. It’s nice to say that the patient is anesthetized for it. But how does anesthesia actually work? No one really knows the full story, because that would require a complete theory of consciousness. We do know, however, that different anesthetics seem to work at different steps of the nocioceptic pathway. In particular, some act further upstream, some further downstream. In the more downstream cases, are we quite sure that, just because your anterior cingulate cortex (or whatever) didn’t get the signal, no part of you ever felt pain, let alone learned some kind of subconscious aversive association to it? But this is precisely the Scientolog…ical concept of an “engram”.
So I think the reply that ECT patients are anesthetized is not really a knockdown refutation of the Scientological critique. That’s exactly what they’re worried about.
The same objection could also be applied to surgery, or any other procedure that’s done under anesthesia, and would be painful without it. Of course it’s questionable whether we should care about some (non-conscious) part of the brain feeling pain.
That’s because Scientology is a mix of random beliefs taken from many places, including psychiatry. Of course when you copy a lot of insights, there will be a few good ones in the mix, together with the bad ones.
Well, my days of not taking psychiatry seriously are certainly coming to a middle.
No offense, Scott.
There’s a lot of good people doing a lot of good stuff (including the blog author). Treatment of people with delusions keeps many of them from starving themselves because the CIA is going to put transmitters in their food. Treatment of people with bipolar disorder keeps many of them from destructive manias or depressions.
There’s just a lot of BS that accumulates because you can’t study the brain the way you do the kidney.
he went to the APA meeting in a mask and gave a presentation arguing for gay rights, and the APA de-listed homosexuality as a psychiatric disorder the following year. How amazing is that?
You mean that instead of basing it on evidence, the APA allowed itself to be armtwisted into changing the DSM?
Yeah, I would say that’s amazing…
What do you think was in his presentation? I assume it contained arguments, some of which used evidence. And I doubt it was literally just that one presentation that caused the change.
Also, what evidence would you say would justify declassifying homosexuality as a psychiatric disorder? I don’t think there was ever any reason save moral opprobrium for it being in there in the first place, so the evidence base needed to take it out should be pretty low.
This is why one uses Bayes’ Theorem. The Null Hypothesis just reifies one’s priors.
The snark here contributes nothing to the discussion and the comment implies that LG folk are mentally ill (which, even if it was true, is not kind). Therefore, this comment is neither kind nor necessary.
Considering that even its truth is up for debate, I wonder why it hasn’t been removed.
If LG people are mentally ill, I want to believe that LG people are mentally ill. If LG people are not mentally ill, I want to believe that LG people are not mentally ill. Declaring such statements off-limits because they make people unhappy to hear them is likely to corrupt your system of beliefs just as soon as you get one wrong.
As for the discussion, it seems reasonable to conjecture that if the APA is politically influenced now, it might have been politically influenced then.
(This assumes “mentally ill” is a useful non-arbitrary category, but denying that claim would undermine the basis of psychiatry anyway)
Great post.
The thing about medical ads taking over around the convention center is something that I’ve noticed in recent years around Chicago’s McCormick Place. (Which I bike past during the warm months because I live a mile or so away.) Seems to happen now for a lot of conventions and I’ve found the billboards for some of them (e.g. dentistry, gastrointestinal, etc) fairly alarming. Round a corner on your bike and suddenly you’re staring at a six-foot-tall ulcerated colon…
Presentations from an alternate universe where the APA is red-tribe:
-Guns and Anxiety: open-carrying as a treatment for agoraphobia?
-Sobriety in the Age of Trump: how the President’s example provides support in alcohol recovery
-How Climate Science hurts those with Anxiety
-She Wants an Education! – How to be sure your client doesn’t want a family
-Trucks, Guns and Masculinity – the symbolism of belonging and mental health
-Hunting and the Cannibinoid System – the science of sport and wellbeing
-Motivation and Prosperity – how to set your client up to pull themselves up by their bootstraps!
-Religion and Wellbeing – tradition helps those who can’t find their way?
-Russia, Russia, Russia – the anatomy of a conspiracy
Love it. This is along the lines of my top-level comment that got eaten.
How about: Hunting and Fishing – which meats are necessary for neurotransmitter function?
Can’t grow a healthy brain without fish oil! Checkmate, libs!
Does this mean doctors don’t prescribe generics because they’re trying to err on the safe side (legally, or for the patient)?
Also later on I think you say that people don’t pay that much (at the point of use), because insurance.
But some people are not going to be insured, and in any case, there’s probably some additional cost. If nothing else, increased insurance fees.
If you want to prescribe clonidine, do you effectively have to ask coded questions and wink at the patient until you can mis-diagnose them with something else that it’s approved for?
If it’s very hard to prescribe the cheaper, equally effective drugs, it seems like there ought to be a simple route around that.
So how much is an FDA approval?
Could a charity just flat out pay for the process?
Could it be crowd-sourced?
It may not work for this specific case, but in general if the question is : “Is this (generic, cheap) medicine X at least statistically indistinguishably as good as this (expensive, branded) medicine Y® for treatment Z?”, and you already had doctors who were treating the patients anyway, then one could run a trial with equal numbers of patients on both drugs, and the overall drug cost would be lower than putting everyone on Y®.
And provided a doctor already has patients insured and able to claim the better drug, it could be even cheaper than that.
Or if not, how come there isn’t a disruptive insurer who only covers the very basics, treatment plus ‘reasonably priced’ or generic drugs? By taking this you’d register to accept all the appropriate substitutions.
Such a hypothetical plan would be illegal under PPACA. Most novel insurance schemes would be. For whatever its merits might be, Obamacare killed any possibility of innovation in the structure of insurance plans.
As far as I understand, it wouldn’t be technically illegal, just not a Qualified Health Plan (QHP). What are the disadvantages if an insurance is not a QHP?
Well, at least until the recent changes made to the ACA by the last Congress, individuals not covered by a QHP paid a tax penalty. So, there isn’t much of a market for non-QHP policies.
But, prior to the ACA we didn’t see much in the way of these kinds of policies either. Potentially because it’s very hard to distinguish between that and a scam at the point where the policy refuses to pay for something.
For an well practiced analog , we might look at managed care in general and HMOs in particular. HMOs are (were) policies that said “we will take care of all your health needs, provide the doctors you can see, who are the ones who prescribe the care you need, Rx prescriptions, etc.”. Anything outside the HMO isn’t covered and you pay out pocket. They hold costs down by providing what is needed at the most effective price.
HMOs didn’t really deliver the promised benefits, and were generally unpopular as well.
Health insurance was one of the most heavily regulated markets in the US even before the ACA. Catastrophic-only plans were already largely illegal.
HMOs were definitely unpopular. But they held down costs (until forced to cover things by courts, rendering the entire concept useless) and did not have any impact on outcomes.
I may not be understanding this fully. I’m not an expert. However, I’ve looked at the wikipedia page for “Qualified Health Benefit Plan” (which is practically a stub), and looked at the “Patient Protection and Affordable Care Act” wiki page (which decidedly isn’t) and think that you may all be misunderstanding what I was suggesting. I think I was assuming a lot carried through on context.
Let me try again:
Imagine a legitimate healthcare plan as a basis. Now add a clause which states in essence that where a generic drug is considered equivalent or better treatment than a more expensive drug for a condition, the former will be used. Probably also an addendum allowing fall-back to the branded medicine® where the generic proved unsuitable.
Now obviously this would have to be worded in a legally watertight manner, and may even have a big list of appropriate substitutions. Let me be clear I’m not specific on and don’t care about such details; I’m not a lawyer and that’s outside the scope of a blog comment.
In essence – where two drugs are equally efficacious, require use of the cheaper one. This doesn’t affect the treatment quality, it just makes it less expensive.
It’s seems that it’s legitimate for insurance to exclude certain drugs/treatments people want to use – it’s easy to find people complaining about that online.
So it ‘ought’ to be possible to rule out drugs with obvious cheaper equivalent/superiors like Fanapt® – at least as a first line option.
“Also later on I think you say that people don’t pay that much (at the point of use), because insurance.
But some people are not going to be insured, and in any case, there’s probably some additional cost. If nothing else, increased insurance fees.”
If you have insurance and you try to fill a prescription for a new drug, they bill your insurance for $2000 and then your insurance probably charges you a $45 copay.
However, if you don’t have insurance, you call the company that manufactures the drug and tell them you don’t have insurance. Then they sell you the drug for $25. If that sounds ridiculous, that’s because it’s absolutely ridiculous.
Were there any sessions about me-too drugs in the #MeToo era?
I couldn’t get past the first two photos. Are they the same stairs? Why is the background purple in one, and blue in the other? Weird camera thing? Is it my eyes and no one else sees this, like the Internet Dress?
If you look at the first picture, in the upper right, you can see a set of blue stairs. Those must be the ones in the second picture.
If you look at the bench, you see that vrylar’s colors are purple and aqua. So I assume that they have two different staircases with different versions of their ad in each of their brand colors.
Big convention centers likely have lots of stairs like those.
Thanks for the responses!
At professional conferences, I make it a rule not to go to talks whose title is formatted “Phrase the Authors Think Is Clever: What The Talk Is Actually About”. Same with books, too.
Is that an attempt at resignedly punishing the title format so it stops, or just that there seems to be enough of a regularity between format and content quality that it’s usually a waste of time for you? (or both?)
If it’s the latter, I expect the pattern to be unstable because it’s often imitated for no deep reasons. Whatever the quality of the talk/speaker, they might sprinkle on this kind of title because they see it as a perfectly fine hook that everyone is used to. And the fact that it can be sprinkled on, that it’s so loosely coupled, would destroy such a correlation.
I wonder how many people would attend if I hosted a talk literally titled “Phrase the Authors Think Is Clever: What The Talk Is Actually About”.
The CIA: does your patient have delusional thoughts about being tracked by us? Call us today, and we can ensure that they any further thoughts they have on the matter are not delusions!
I remember reading they rotate intelligence officers in and out of counterintelligence precisely because they tend to get lost in the whole paranoid ‘hall of mirrors’ mentality.
I’d ask an actual intelligence officer to comment, but of course they can’t do that…
In the section on the CIA, I was reminded of this NPR article about the CIA just, showing up at nerd cons with recruiters. And as I clicked on the CIA’s twitter feed linked in that article, I note that the latest CIA Tweet© opens “Did you know that CIA has several #artists within our ranks?”
Something of a broader trend here. Apparently the current CIA thinks that the shadowy mystique of being America’s supervillains isn’t worth the PR of being… America’s supervillains.
I mean, given that professional wind ensembles aren’t really a thing except as a summer job for professional orchestra members, the military bands are pretty much the height of non-school wind ensemble excellence.
The CIA also has lots of jobs that look nothing like being a supervillain.
Like identifying, defending against, and prosecuting cyber attacks.
As I understand it, those are all NSA responsibilities.
Only those against US citizens or US government entities. Possible also official allies.
The pervasiveness of woke politics at what should theoretically be a science convention is distressing to me. The fact that the quoted block is true, that there are three times as many talks about a current political controversy as there are about a major, common medical disorder, at a medical conference, is upsetting to me. As in so upsetting that it sometimes impacts my basic quality of life and ability to fulfill my life obligations
This is the kind of thing that you would go to a psychiatrist for, but based on what I’m reading here, that would probably be close to the worst possible thing I could to address this. Short of joining scientology and banking on reversed stupidity, what should I do about this?
You could join the political factions that oppose wokeness. That might make you less upset and able to do basic life functions.
I am not a psychiatrist, which I think in this case is speaking towards my qualifications, but don’t rely on me as anything but a cynic.
Indeed one could, but if one is of the classic left, it’s becoming increasingly hard to find good bedfellows.
Traditionally, you have to put up with strange ones.
Ah, but with strange eons, even death may die.
You could, but in the modern political climate, doing so could be hazardous for your mental as well as physical health (depending on where you live, of course).
Are you guys being serious about this!? Joining one of the anti-woke factions is going to be just as deleterious for horseshoe theory reasons. Radicalization is bad no matter what direction it’s in.
The better thing for eqdw’s mental health is abstension, and then they can notice that woke-ness doesn’t have nearly as much influence as they think it does. It’s a paper tiger. Biden leads the primary polls.
Seriously, the anti-woke factions are just as bad in many cases.
Avoiding politics is probably the smartest thing for most people. If you work with woke people, just nod and agree and go home and take care of your kids (or your programming project).
Of course, that’s how they win…
You could always take the red pill, eat paleo, lift weights, and stop cucking. I doubt (((Scott))) wants you to do that, though. He’s just trying to blackpill you and keep you from noticing who’s *really* behind Cultural Marxism and the Great Replacement. Or why would he keep voting for the DemonRATS?
(Joke…)
Now this is an interesting conundrum. I believe that excessive wokeness is harmful for society in a number of ways (but less so than you probably think, calm down). But based on my personal experience, I also believe that trying to actively oppose it is harmful for one’s career, social life, and mental well-being. I tried open opposition, got burned, and now bite my tongue everywhere I go. Which also has psychological costs, but fewer than those caused by the fallout of the other approach.
For me, it would be best for other people to fight it while I passively cheer on from the sidelines. But I do know that this has costs that I am not willing to bear myself.
So, what advice do I give you? For your own well-being, it is probably much, much better to keep your head down and not worry so much. Tend to your own garden and let things sort themselves out. The impact on your own personal life is much smaller than you think. Unless you have the misfortune of working in Academia or SV tech, that is.
For everybody else’s well-being, including those in a permanent woke frenzy, it’d probably much better if you opposed wokeness actively. But do so in a way that doesn’t give them more ammunition.
The thought that usually calms me down is that moralistic authoritrianism is simply an unavoidable aspect of human social life. It takes on different forms, but the structure stays the same. As do the fundamental motivations and incentive structures for the people involved. A few decades ago, you had fundies, now you have Wokies. Read some Nietzsche, maybe. Learn to affirm the eternal recurrence of the small man. 😉
My advice, read this: https://slatestarcodex.com/2017/10/23/kolmogorov-complicity-and-the-parable-of-lightning/
What does “got burned” mean in this context? What did you try?
Comrade Stalin requested feedback on how to better run the farm. I foolishly suggested that maybe sending off all the anti-Lysenkoists away for reeducation might negatively impact efficiency. I got a stern talking-to by a Very Concerned Boss and I was replaced by an incompetent party member at the earliest opportunity.
That’s just one of the many similar experiences I had in this regard. It’s not worth it for me personally.
Could you describe what actually happened, rather than a metaphor about Stalin? I’m curious about what you mean when you say you got burned in today’s reality.
I’m being intentionally obscure because I don’t want to be identified.
One recent episode I remember that fits the pattern described above was that my former employer sent around emails that described in great detail how they were committed to the goal of gender equality and asked staff if they had any exciting new ideas on how they could better discriminate against men. My idea of “maybe don’t” was not met with great enthusiasm and I was replaced shortly thereafter by a female employee with much less experience and worse credentials (I know because I’ve seen her CV).
No, I won’t disclose any other details.
Be prepared to receive just-worlding on how it wasn’t what you said but how you said it, or contrariwise that you should have known they weren’t really asking for suggestions and you should have kept your mouth shut.
Well, they clearly weren’t really asking for suggestions (from me) and I should have kept my mouth shut.
Is this the new “Wow, so brave”?
(Less snarkily: Can you not complain about how your outgroup says bad things when they haven’t actually shown up in the thread yet? We have more than enough CW without taking random potshots)
I disagree. Preemptively redirecting an otherwise fully expected unhelpful narrative is a good thing. You’ll just have to make a better argument instead.
@Mark Atwood Note that @The Nybbler didn’t write anything about why the hypothetical arguments would be wrong. Dismissing an argument purely based on speculation about their motivation is not legitimate.
It looks like the bottom line here is that there weren’t enough people doing sandwich board advertising to be notable. Did the conference have a rule against attendees wearing sandwich board advertising, was it difficult to gain admittance, or is there a way to liberate drug marketing departments of lots of money by dressing up at conferences?
I see a very similar pattern in aviation. The GPS chip in your iPad? $50. The GPS that is FAA approved to go an an airplane? $10,000. I’m not kidding with those figures. It’s illegal to fly with the first one, though it works just as well, arguably better. It’s not surprising that most pilots do exactly that. (I’m talking private pilots here, not airlines)
Is that actually true, though ? I don’t know much about GPS chips, but I was briefly involved in developing a black-box. It had a bunch of accelerometers and other sensorts, a tiny CPU, and some memory storage. It also cost $CLASSIFIED dollars. For that price, you could’ve bought a whole crate of iPhones with way better functionality… but… here’s the catch: the device we worked on had to survive being fired out of a cannon at a brick wall; set on fire and frozen (practically at the same time); plus a whole bunch of conditions I don’t even remember, and that’s not even talking about power draw and physical dimensions. Everything inside it had to be custom-designed to fulfill those requirements, and that kind of engineering does tend to drive up the price.
IIRC, the big difference between aviation GPS (for private planes, not whatever the airlines have) and ordinary handheld GPS is that the aviation ones had an FAA-certified database of flight-relevant locations in it.
No need for an airplane GPS to be the guidance system for an artillery shell or whatever.
Consumer GPS chips disable themselves if they are moving too fast and/or too high. If it thinks it’s being used as the guidance system for a missile, it stops working.
60,000 feet and 1000 knots (though many manufacturers implement this as “or” — the actual rule is more lenient). Not an issue for private aircraft or even airliners. Also at least with older Garmins this was pretty easily disabled, usually by people who just wanted to exceed the altitude threshold.
And yet Boeing’s MCAS somehow managed to pass FAA certification.
For $10,000 you get a GTN-650 which is a whole lot more than a GPS chip and probably exceeds an iPhone in hardware complexity. You also get software that, along with the hardware, is tested and validated to standards that Silicon Valley seems to believe are beyond the realm of the possible, with the cost of that testing and validation spread across a user base of tens of thousands rather than hundreds of millions. That’s where most of the $10,000 goes.
It’s not illegal to fly with an iPad(*). It’s not even illegal to fly with only an iPad – so long as you use it only for situational awareness. If you want to do navigation and collision avoidance under IFR, then you need to use something that has been validated to aerospace rather than consumer-electronics standards.
A very large number of pilots use iPads, legally. Almost no pilots fly in IMC without aerospace-grade navigation systems, which start at about $5000.
* It is only a modest exaggeration to say that it’s illegal to fly without an iPad, though the FAA still supports the old-school ways of e.g. filing flight plans for the time being.
The Garmin G5 unit that we have ($2500), certified for IFR, has the unfortunate known defect of turning itself off for no reason. Which has happened to us at least once in the last 100 hours or so. I’ve also had two KLN94 GPS’s crap out on me more than once, with either lost signal, screen freezing, or other strange bugs. Just as a few datapoints against the infallible certified stuff.
To be a bit more fair though, we looked at iPads for ADS-B-in traffic awareness and a back up attitude indicator (using a Stratus Appareo non-certified system, plus certified ADS-B out). By the time you add up the iPad and other hardware and subscriptions for apps/charts we were looking at at least 50% of just buying something certified.
And then the display of an iPad is too dark for direct sunlight, there are all sorts of failure modes (ipad gets too hot, ipad has to do an update, ipad charging cable quits, app subscription expires, chart subscription needs an update, ipad not charged). And you have extra wires and gear and unsecured crap all over the cockpit that is aesthetically displeasing and can be a real hazard when ditching.
Grabbing the third rail implies a dangerous topic to raise due to the controversy. Was this presentation about racial differences in brains, or were the presenters overestimating the bravery needed in decrying racism in 2019?
Id expect this to be something like “a textual analysis of patient charts” that found that white patients get more word count, or that the rate of inaccuracies is higher in underserved populations, or something. Or non-PC words being used in clinical notes.
Yeah, exactly the kind of analysis likely to be met with nods and sorrowful soul-searching, not shocked outrage like the ‘third rail’ title implies.
(Albeit otherwise a potentially useful topic!)
Some random observations:
The CIA seems to have the most reasonable case to explicitly focus on ethnic diversity over mere capability, as they need to be able to fit in worldwide to
murderpacify andspy onhave good relationships with foreigners. Wired has been making some videos with the FBI and CIA about how they do their job. I can see them having a use for psychiatrists, both at the office and on missions (to react quickly to surprising situations).Why does the CIA have such a shitty booth? You helped get Bin Laden. Surely you can present something nice/patriotic.
I noticed the delusional title “Grabbing The Third Rail: Race And Racism In Clinical Documentation” which implies that talking about racism at APA is somehow career-ending. How brave to speak out as a
sole50th voice.This conference seems like a dystopian nightmare:
– we give you free ice cream, because only it gives us the chance to lie to you, so you’ll harm mankind by using our product.
– everywhere you look, we put ads. Want to take a break from it all? We put ads on the benches! We do give away (branded) pens so you can stab yourself in the eyes.
– want to leave because you can’t take our ad bombardment? We put ads on each step of the stairs, so you won’t be free until you reach the doors…and not even then, because outdoors is plastered too.
– talking about outdoor ads: when the city doesn’t provide enough ad space, we build our own city, so we have extra city advertising.
– look how nasty it was that many in our profession didn’t help gay people, but falsely accused them of harming others. BTW, did you know that the involuntarily celibate will likely end up killing women?
This article almost makes me feel sympathetic for Scientology for opposing this (just kidding, they suck even more).
oops, you made the same observation as me.
Sure, and then you can see a panel next year about how the APA’s culture of flag-waving jingoism is contributing to mental health problems in oppressed minorities.
Yep.
If by ethnic diversity they mean hiring more blacks and hispanics, then this is mostly irrelevant to having good international “outreach”. If they mean hiring second generation immigrants from Russia/China/Iran/etc., then it makes sense, but there is the obvious failure mode that these people might be more loyal to their ancestral homeland and ethnic group rather than Uncle Sam.
Of course, any discussion of dual loyalties of immigrants, especially second generation ones, is very non-PC, not unreasonably due to an unfortunate historical precedent.
And the Crimean Tatars.
The CIA is having the same trouble inventing the next AIDS as the pharma companies are having inventing the next Straterra.
As part of my wandering younger days, I spent between six months and a year attending a Scientology congregation. While individuals do not equal a movement/institution, what I found there was that generally people described the psychiatry of the time of the religion’s founding to be the bad psychiatry, and that modern psychiatry had vastly improved with its changes in approach (lack of institutionalizing and institutional abuse, less satanic cult panics, not treading homosexuality as a mental disorder). The big thing they were against was overprescription/overdiagnosis, which is a common laymen complaint against psychiatry.
Again, doesn’t mean there isn’t an anti-psychiatry organization founded by Scientology, just saying that thought’s not monolithic among modern church members.
“Why does the CIA have such a shitty booth? You helped get Bin Laden. Surely you can present something nice/patriotic.”
Given the audience, that would attract negative attention and be a turn-off to the people they want to recruit. Many psychiatrists in California will be starting out with a negative opinion of the CIA. They win by blending in and getting people to take a flyer on auto-pilot.
“look how nasty it was that many in our profession didn’t help gay people, but falsely accused them of harming others. BTW, did you know that the involuntarily celibate will likely end up killing women?”
In Wokistan, “incels” doesn’t mean “people who are involuntarily celibate,” it strictly and exclusively means “people who participate in the explicitly-incel-labeled online community, and occasionally people who parrot the talking points of those communities in other online spaces that are not explicitly incel.”
Only when making moral judgments about the morality of this group, not when deciding who belongs to this group.
Scott has addressed this.
In roughly the same way that the N-word strictly and exclusively means “black people who participate in a lifestyle based on street crime, and occasionally people who glamorize that lifestyle”. That’s the motte. It’s nice and defensible and maybe even useful. Now consider the bailey.
Looking through your pictures, I have to say the convention I was at last weekend looks a lot more fun. Instead of people trying to change my mind about all kinds of things and putting massive pressure on me to buy things for my patients that are over priced, I had a weekend of video games, anime, and nerd paraphernalia, with panels that are entertaining and some with real swords.
Maybe next year, skip the APA convention and come to Anime Central where we have fun and games instead of lies and protestors.
Why wait? Scott can just hit up Fanime in San Jose is this weekend.
Because Anime Central is bigger and better. No offense, but we’re the second largest Anime convention in America and much more fun than Anime Expo (the largest)
Acen isn’t bigger. According to wikipedia, it had around 32.6K attendees last year, while Fanime counted 34K. It’s just that Fanime is no longer included in the ranking lists because it’s not considered an anime-only convention anymore.
(And where are you getting your numbers? It was only #5 in 2017, and most definitely wasn’t #2 last year, by a quick skim.)
It may be relevant that people use their own money to attend fan conventions. No business deductions or anything.
That’s play. He’s there for work. Of course you had more fun.
The CIA needs psychiatrists, too, and not just for illegal mind-control experiments. I’d guess that some of it is for things like interviewing people who are coming in for clearances to make sure they’re not likely to snap and start spreading secrets everywhere. (Although that’s probably more a psychologist job.) The higher-level version is deciding guidelines for that kind of stuff. Is someone who had a psychotic break 10 years ago able to be trusted with our country’s secrets? What kinds of psych meds are disqualifying if you’re trying to get a top-secret clearance?
But I’d guess that most psychiatrists in the CIA work on the mental health of persons of interest to the US. Having a detailed profile of the guy you’re going to be sitting across the negotiating table from is of obvious value, and someone has to write them.
The CIA probably needs psychiatrists for its own people and I’m not saying that pejoratively. Think about how difficult forecasting is, add in the pressures of “Hey if I screw up this intelligence analysis we might be bombing Botswana by Friday”, and then, oh yeah, you can’t talk to anyone about it because your work is classified. I expect the CIA wised up to the necessity of having someone on staff that its covert and overt employees can talk to without violation national security procedures.
They also torture and murder people, which doesn’t just emotionally affect the victims, but often also the perpetrator.
How long before the “wokeness” itself becomes a topic for panels at psychiatry conferences? (Yes, I’m being snarky, but also not joking; I think it’s making a lot of people miserable, probably including many of the crusaders).
I say give it 10-15 years. 5-8 years for it to stop, then some time after for everyone to look around and say “wait, I wasn’t the only one who thought that was weird?”
The collapse of wokistan is a bit like the cold fusion reactor: perpetually around the corner. The first time I heard this prediction was 8 years ago.
It is starting to become annoying to companies–I have a clickbait article up in another tab about Google et al’s increasing problem with protesting employees. At some point, corporations will feel that encouraging this mentality is distinctly unprofitable and disruptive, and find a way to squish it. That’s one major source of support; the other is academia. Don’t know about them.
I have a hard time believing this, at least for the foreseeable future. Hasn’t woke capital been on the rise? Look at Nike’s recent Kaepernick move; do you think that wasn’t calculated, and a successful calculation at that?
As bad as it is, I think it would have to become distinctly worse for companies to reverse course.
There you’re talking about flogging culture war for free controversy as a form of advertising. It will eventually yield diminishing returns, but they’ll still be stuck with angry employees causing trouble in-house. And the two can’t be neatly separated.
I don’t have the quote handy, but there’s an observation that wokeness is the opposite of CBT– catastrohizing, black-and-white thinking, and such.
Several of the climate change sessions don’t strike me as “woke” — they strike me as clinicians grappling with a serious mental health problem. I can only speak for myself, but if there’s any situation that should inspire existential levels of anxiety in a patient population, the current situation with climate change is probably it. It’s basically a horror movie that’s happening in real life.
I’m not sure I agree. The catastrophic effects of climate change are a prognosis, not a fact of life for most people in the US/EU, extreme weather events notwithstanding (and it’s not like there were no hurricanes or tornados in the past).
Your level of existential dread is therefore likely to depend on how much faith you put in the prognosis.
To put it in perspective, if you believe in hell – and the possibility you might end up in it – climate change isn’t going to register as that big of a deal, when considering possible existential threats that apply to you.
To summarize: if you’re someone who puts faith in scientific evidence put forward by conservative and reputable institutions, then existential dread is a pretty reasonable response. That’s a lot of people.
Or it’s a case of thunder before lightning, in which case no dread is necessary. The fact that it’s a major psychiatry conference topic suggests the former. But I could be wrong, are public topics and the relation to [illness] common panels at psych conferences?
Can you give scientific citations that justify these “existential threat” claims? Effects of global warming I’ve seen mentioned include things like more extreme weather phenomena in some areas, more droughts in some areas, or some species going extinct. Nothing that would make us all die, or even that would be likely to seriously affect people living in developed countries. There is a lot of scientific evidence for the global warming itself, but that doesn’t mean that if some popular newspapers say that global warming is an existential threat, that claim is backed by scientific evidence.
It’s difficult to make predictions, especially about the future.
One might also note that theology departments are also conservative and mostly reputable institutions, often of great vintage.
John Schilling made my point a lot more directly below, so I won’t reiterate it. For myself, I have an economics background and that affects my priors. My faith in science that offers no reliable engineering, but is intricately interwoven with politics, is essentially nil.
I submit to you that the Cold War was significantly more terrifying, and the threat more imminent and easily understood. Did the 1965 APA convention have a bunch of sessions on reassuring patients worried about their families getting vaporized?
That wouldn’t sound that surprising to me as a thing that might happen?
I don’t know about 1965, but here’s the report (PDF) of an APA task force from 1982 on nuclear issues. It includes articles about the human response to the threat of nuclear war and power plant disasters.
Edit: as far as the cold war being more terrifying — maybe that’s true. But de-escalation was always possible (and indeed, happened in the 1990s.) Right now serious climate change feels much more inevitable, since we’ve already baked a lot of future temperature increases into the cake with our past CO2 emissions.
Significant climate change seems very likely, although how large isn’t clear, given the wide range of estimates of climate sensitivity. But that the change will produce large net negative effects is still a conjecture, not a clearly established scientific fact. If you look at the estimates of net effect on humans by Nordhaus or the IPCC, they are tiny relative to the catastrophic scenarios that scare people.
The horrific parts either aren’t happening yet or aren’t happening anyplace the clients of the median US psychiatrist is going to see them. If people are horrified, it is for the most part because of what they have been told, not what they have seen, and for the most part not what they have read in scientific journals.
And this is not new. Overpopulation, nuclear war, superpredator criminals, Satanic cults, etc, etc. The psychiatric community would probably benefit from regular, recurring education on e.g. “How to treat patients who have been terrified into dysfunctionality by clickbaity apocalyptic headlnes and stupid Voxplainers”. It is unlikely that the technical nature of the media-hyped horror du jour is of significant psychological relevance; “the population bomb is going to kill us all / make life not worth living, and there is no hope and nothing I can do” likely has the same effect as “global warming is going to…”
If the current round of apocalyptic predictions turn out to be objectively true, that also is of no psychological relevance until they actually come true, or for the tiny minority of patients who are competently and dispassionately following the technical literature.
So a preponderance of articles being object-level “Global warming is driving people crazy!” rather than meta-level “Sensationalist journalism continues to drive people crazy”, does seem to be an indication of Wokeness run amok.
That’s my position–it’s the alarmism that gives psychological problems (assuming there are cases of those, which we infer from the topics but I don’t know of any personally).
The argument would be that the situation is indeed dire, we live in a democracy, and we require people to be informed in order to vote or otherwise exert influence to solve the problem.
I don’t really by that the apocalyptic run-away scenarios in popular activism for CC are in fact likely, but even given that they are, it’s worth addressing if the activism is creating problems it wouldn’t by other no less effective methods, such as not trying to scare elementary aged children, and so on.
Bill Nye just set a globe on fire on twitter to terrify people further. This seems more like psychological warfare than activism.
Can the APA please do something useful and declare letting children have a social media account is child abuse?
Is alarmism irresponsible if you’re confident that the worst-case scenarios are realistic and no-one seems to be paying attention without alarmism?
I was trying to give that point it’s due in my post; if you think the ends justify the means, then, it’s reasonable, but even then I question some of the methods, like scaring children.
People so terrified that their imminent doom is inevitable that they need to seek psychiatric treatment seem unlikely to be able to achieve anything productive in addressing climate change.
Scott, not sure if it adds to the conversation here, but as a professional blogger, I just want to share that I’m consumed with jealousy.
Your effortless magic, post after post, is a sight to behold.
Because, of course, it’s not effortless at all. It just seems that way.
There are 42 things about this post that are delicious, memorable or simply worth stealing.
Thanks for showing up and raising the bar as well.
Wow.
Seth
It’s actually worse then you know. Scott’s said that the writing just happens, so it is, in fact, nearly effortless. He’s lucky (and brilliant) and I’d be jealous if I wasn’t so impressed.
I totally agree with your comment, but
reminded me of this..
Jealousy vs envy…
I was going to say “Spend thousands of hours practicing, and you can be that good too.”, but then I realized that you’re Seth Godin, and you probably did that already.
Wait, Seth Godin reads – and comments on – this blog and nobody is getting more excited about that? Have any bigger ‘celebrities’ (or, say, succesful authors) done that before?
Anyway, hi mr. Godin, cool to see you here!
Only just recently learned about meds to treat tardive dyskinesia. Am still not sure they aren’t some kind of prank, or maybe a sting by some agency to catch overprescribing quack therapists. If you’re screwing up the patient’s neurotransmitters so much that they’re involuntarily making faces like a French bulldog with a mouth full of peanut butter, the answer is probably to step back and try to figure out if they can be weaned off some of them. Do not repeat DO NOT try to stuff another clown in that car.
Also, if you’re over sixty, and on ADHD meds because otherwise you’d be unable to wake up after taking eight other meds which all cause sedation, something has gone wrong. You’re essentially going through life as that one drunk who takes coffee so he’ll be safe to drive home from the party. On doctor’s orders. Because the doctor is too overworked and stressed out to sit down and solve the wacky Rubik’s Cube that years of aggressive medication have made of your brain. Here’s a short-acting benzo, a long-acting benzo, some Ambien, and an opiate. See you next month!
But I’m just a tech, what do I know, etc., etc. …
Tardive dyskensia is usually a side effect of antipsychotic meds, which are nigh-universally agreed to be horrible by patients for reasons of which tardive dyskensia is one of the most mild. (I knew a guy for whom antipsychotics broke his ability to notice that effects have causes.) Nevertheless, antipsychotics can be incredibly important and life-saving drugs for people with psychosis, and the side effects can be worth it.
In addition to this and importantly for this context, it’s a side effect that can be permanent even if you go off of antipsychotics.
Have spoken w/pharmacist, confirmed that I incorrectly assumed this was another example of doctor shrugging and throwing pills at a problem. Apologies.
Psychiatrists are so woke they will extract huge amounts of money from you (of which many cannot afford) and therefore paradoxically contribute to people’s poor mental health.
The psychiatry industry tries to pretend its all about people and helping people but in reality its very exploitative and selfish.
They aren’t, like, making you go, right? Like, calling a voluntary industry exploitative strikes me as weird. I’ve never payed a shrink a cent, and they seem to be ok with that.
Exploitation can happen through fraud. A psychiatrist is supposed to be an expert, who is expected to act in your interest, in a way that you cannot do yourself, due to lack of expertise.
If they prescribe overly expensive or even much more dangerous medicine because they get gifts or simply due to laziness, I consider that exploitative.
It’s mental blackmail. “Hand over a huge sum of money or you will continue to suffer”.
If your car is in need of maintenance, you go to a mechanic. If the mechanic spends an hour lecturing you about transgenderism and then sends you on your way, he’s not a mechanic, he’s just exploiting your need for one.
The thing a lot of people on this thread don’t seem to know is that forced psychiatric treatment is not at all a thing of the past. Yes, it’s gotten harder to get a court order forcing an adult into a psych hospital. But there are still huge numbers of people still vulnerable to forced psychiatric treatment: children, teenagers, young adults, the elderly, people in prison or on probation.
Sure, but, like, that’s mad understandable in the context we are talking about, yeah?
Like, An Firinne is talking about how they charge huge amounts of money and cheat people by being unable to deliver. Then I respond that nobody is forcing you to buy.
You answer me by saying that some people are indeed forced to get psychiatric treatment, which, sure, but those people aren’t paying for it, yeah? Like, in the context of evaluating the psych industry as money-grubbers, it was fair of me to disregard children, people in prison, etc, since they are pretty much broke?
To put it another way, out of the total amount of profits taken by psychiatrists, what percentage would you say they get from people involuntarily undergoing treatment?
Oh yeah, they DO charge people who get hospitalized on 5150 (or Your Local State Equivalent) or involuntarily committed, assuming they have insurance or the money.
right, but, ‘assuming they have insurance or the money’ is doing the work in that sentence.
If someone has insurance or money, but not the independence to keep themselves from being thrown in a mental hospital, then I expect that the actual owner of the asset in question is whoever their master is, and they will find it expedient to take it off the name of the victim and leave them judgement proof.
The poor (particularly those in the first world) aren’t considered an identity group in contemporary Wokistan. This has caused not a small amount of tension between the old left, who were more class-focused, and the identity-focused new left.
Interesting write-up!
Are there similar levels of wokeness at APA meetings not hosted in California/SF?
>Make sure doctors know the magic words they need to use to force insurance companies to pay for it.
Are insurance companies stupid? If not, maybe the taxpayer gets to pay for it, after all.
Just looking at that picture, Medicare / Medicaid are kind of obvious, even if the insurance companies flat out refuse the new medicine there is money in those two. I have no idea what RelayHealth eRx copay assistance means, but do these kinds of things tend to happen without any sort of governmental investment at all? It sounds like something helping people with financial difficulties or at least liquidity issues to get their medicine regularly. Which sounds like the kinds of things government programs tend to do.
I don’t think insurance companies are permitted to just refuse to pay, otherwise they’d, like, always do that? I mean, ‘people pay me to pay them and then I don’t’ is certainly a winning strategy.
How do health insurance contracts work in America? I could imagine a contract that details which treatments they cover for each existing disease, but that would probably be some thousand pages of dense medical language. It could work, though, if independent reviewers then say something like “this insurance covers every medicine, except some for which a cheaper medicine with essentially equivalent mechanism exists”, or “covers everything up to $50,000/QALY”. Do they, instead, just cover every treatment a doctor prescribes, whatever the price?
All of the action is in the “except.” There are big, life altering differences between newer insulin and older insulin, but the mechanism is essentially equivalent. Having an epipen and calling an ambulance for allergic responses have the same drug, just a different delivery mechanism, but in one case you’re a lot more likely to end up dead.
@10240,
Insurance plans cover categories of treatment, which usually includes all medical treatments and drugs, plus some things like chiropractic, etc… with the health plan differences tending to be in how a deductible or co-pay might apply, what percentage of the bill they pay for providers they have a contract with (in-network), vs. if you go to one which they don’t, like 90% in-network, 60% out of network. The deductible is the part you pay (the 10% or 40% or whatever in the above examples) until you hit an annual max, say $3500/person or $7000/family.
The categories are things like primary care visit, specialist visit, diagnostic tests, imaging, preventative care (usually covered 100% because it theoretically saves them money), generic drugs, preferred brand drugs, non-preferred brand drugs, specialty drugs, outpatient surgery, emergency room, hospital stays, pregnancy, mental health services, rehab, high-level stuff like that, which mostly exists to steer people toward options which cost the insurance company less.
So for drugs, for example, you might pay a $5 co-pay for a generic, $45 for a brand name version, obviously designed to allow you to get the brand name if it medically matters, but push you toward the generic version if it doesn’t.
Then there may be a short list of exclusions, like elective cosmetic surgery isn’t covered, you can only get hearing aides once every 3rd year, that sort of thing, but they usually aren’t very extensive… like six things mentioned in mine.
The edge cases are where you may have an exclusion where they classify certain super-expensive and/or ineffective drugs as “specialty” and they want you to use their specific pharmacy for those, or they have a $10K/year cap on drug payments, stuff like that. Otherwise, in terms of if they are liable, its generally going to be anything a Doctor can justify to them is medically necessary for you. Some companies (who hire their own people to review stuff) may argue about something really expensive they think isn’t necessary, or require pre-approval for something which can wait, but its usually up to the Doctor involved to either be able to justify it based on the official medical “standard of care”, or not.
This is fantastic – reminds me of Thompson’s gonzo journalism at its finest.
Great article!
Somewhat related- the latest episode in the webcomic Order of the Stick is called “Replication Crisis.”
(But if you haven’t been following the comic until now, you won’t understand this one, and it contain major spoilers for earlier events.)
Typo: “1. Take an popular older drug” -> “1. Take a popular older drug” (appears twice)
Typo here. Enjoy the lawsuit.
“APA de-listed homosexuality as a psychiatric disorder”
Seems like an example of going to the mirror-reflected unscientific bias.
Bias 1) Here’s a behavior which is almost perfectly Darwinian unfit, so we may reasonably hypothesize it is caused by some biological malfunction. We have little idea what that malfunction is, so let’s call it a “psychiatric disorder” and treat it with hormones to drive our patients crazy.
Bias 2) Here’s a behavior which is almost perfectly Darwinian unfit, so we may reasonably hypothesize it is caused by some biological malfunction. We have little idea what that malfunction is, but in the past it has been treated with cruel ignorance. Let’s make up for that by declaring it to be normal behavior and restricting discussion of possible causes.
Do you mind expanding a bit on the part on restricting discussion?
Sorry. I just wrote a long response, which I lost due to connection failure.
In short, having read the position statements of the APA on homosexuality and on conversion therapy, my impression is that while one is not specifically forbidden to contemplate the empirical question of the underlying causes of homosexuality, one is strongly discouraged from doing so.
Is that impression inaccurate?
That something is “Darwinian unfit” doesn’t mean it’s a problem for the individual person, and medicine should be about treating problems rather than enforcing normalcy.
Also, having 1-2 children instead of 7-9 is pretty “Darwinian unfit”, but we don’t diagnose middle-class families with a psychiatric disorder.
“medicine should be about treating problems rather than enforcing normalcy.”
Yes, and non sequitur.
I’m asking an empirical question, not proposing a diagnosis or course of treatment. Given a behavior that is almost perfectly unfit, it wouldn’t be surprising if the underlying cause had other health consequences, even if you think the behavior in question is harmless to the individual (again an empirical question).
As for middle class fertility patterns, they are not almost perfectly unfit but only relatively so. Even then, it seems reasonable to look into the underlying causes. If a population has below replacement fertility, it is reasonable hypothesis that something is wrong.
You are not asking a question at all actually. Not a single question mark or question-like phrasing in your top comment.
If an individual is presenting with other health consequences, look into those. Otherwise, you might be wasting treatment resources on a perfectly content person.
Below maximum fertility is a puzzle, since it isn’t what we are “as if designed for.” Why would there be some special puzzle about a population with below replacement fertility?
Let me expand on the sense in which this makes sense, where “wouldn’t be surprising” is not a very strong claim.
We have an explanation for the characteristics of living creatures–Darwinian selection. We observe some characteristic that does not appear consistent with that explanation. There are then three possibilities:
1. It really is consistent, for some non-obvious reason (the gay uncle explanation for homsexuality).
2. It really is inconsistent, but we have an explanation of why it occurs (the conflict between individual self-interest and the interest of your genes, which explains why few people in modern developed societies produce as many children as they could successfully rear). The explanation might be consistent with individual interest (that one) or inconsistent (a taste for foods that were scarce in past environments, are plentiful now and bad for you when over consumed).
3. It is inconsistent and we have no explanation.
In case 3, we have no reason to expect the characteristic to have good effects and a plausible guess is that it is due to something going wrong—consider a random mutation that has observable effects.
So a behavior that appears clearly inconsistent with reproductive success is reason for suspicion of something wrong, but only suspicion.
Human beings have a tendency to dislike the abnormal, so abnormality often causes people problems, even if only due to how others react to it.
From experience, I can tell you homosexuality has some clear inherent downsides. Smaller pool of partners and significantly more difficult to have children are the obvious ones. Not everyone finds these things detrimental, but I think the fraction is larger than is popularly perceived, and it would hardly be the first mental illness that some people find livable and others want to get rid of it.
On the other hand, I can see why keeping homosexuality itself as a mental illness had second-order consequences at the time that were undesirable. Maybe they should have done what they did with transexuals and add a “sexuality dysphoria” diagnosis that’s basically “homosexuality, but it’s causing the patient serious problems”.
The difference between trans people and LGB people is that trans people require, as part of the normal course of things, physical medical care which would ideally be covered by insurance.
Would your proposal include a similar diagnosis for heterosexual people who wish to change (for example, men who want to have casual sex more easily, women who are concerned about STIs, anyone who would like a larger pool of sexual partners, etc.)?
Sure, but I suspect the set of people so distressed by being heterosexual that they wish to change is essentially empty.
If you leave aside issues of homophobia, I’m not sure why anyone would want to be straight. Bisexuality gives you more options.
eyeballfrog – if more male incels understood that most gay men are bottoms, there might be a lot more demand for therapy to get over the disgust that it’s a guy giving them a blowjob.
Wait, what? Citation?
I thought it was about evenly distributed top/bottom/versatile. Quickly googling it now it seems pretty hard to tell but at least people self-identify fairly evenly.
ETA: Also, what does whether they’re top or bottom tell you about blowjobs? That’s a different thing.
I know a lot of nonbinary people who would include themselves under trans, but don’t want medical help. Conversely, around the time when the NHS was debating whether to fund PrEP or not (which I’m going to file under “medical”) there were a lot of articles about how it’s absolutely essential to gay men’s lives.
I knew one fellow who was convinced it was a disease and the APA had been strongarmed into calling it not that.
He also practiced in New York in the 1970s through 2000s, and had quite a few colleagues who had died of AIDS.
I managed a while ago to get the last edition of a book on the treatment of homosexuality that had been de-accessioned by a medical library. It did seem like, in some cases, while they couldn’t remove homosexual thoughts, they could stimulate heterosexual ones–i.e., you can’t make a gay man straight, but you can make some of them bi. Which was enough for them to avoid societal homophobia and raise families–after all, plenty of people have thoughts they don’t like. Did they break up afterward when gay liberation hit in the 90s? I doubt any studies follow patients out that far.
The book was lost in a move and I can’t find it now.
(Schelling Fence installation: Conrad will make at most two responses in this comment thread about the downsides of homosexuality)
There are many negative health outcomes associated with the homosexual lifestyle, such as much greater risk of diseases, drug and alcohol abuse, depression and suicide. If we had another pattern of behaviors that so strongly correlated with this many physical and mental health problems of this magnitude, we would have national awareness campaigns directed at stomping it out. Yet not only do we not do this with homosexuality, but even bringing awareness to these problems is outside the Overton window.
Gay women have much lower rates of STIs than the median. The problem here isn’t gayness, it’s men.
I don’t think bringing awareness of these problems (at least the diseases) is outside the Overton Window. Several of the gay men I know tend to be extremely critical of at least some of the behaviours and attitudes that lead to high STI rates among MSM. But it’s probably understandable that they don’t react kindly to that sort of narrative coming from groups who, historically, haven’t exactly had their best interests at heart.
Given the history, talking about “stomping it out” probably isn’t likely to lead to a productive conversation, either. There have been no shortage of efforts to stomp out homosexuality, many of them very nasty indeed. None of it has worked.
I’m not sure I agree that it’s obvious that homosexuality is “almost perfectly Darwinian unfit”. Population genetics is complicated, as is social history. Homosexual behaviour can be adaptive in other species, and there are hypotheses that explain male homosexuality in humans in these terms. Though I agree they tend to be a bit shaky.
In my experience, the strong emphasis on homosexuality being allegedly totally unfit tends to come from people advocating the homosexuality-due-to-pathogen theory, which is WP:FRINGE to say the least and probably too CW to discuss here (though there is now a new non-integer-numbered OT).
“I agree they tend to be a bit shaky.”
These are arguments from inclusive fitness? Is there another one besides the “helpful gay uncle”? How does that one work? You have to be so helpful that your sister has more than two times as many kids as she would without your help?
“homosexuality-due-to-pathogen theory”
I don’t have a preferred hypothesis. I just think it’s an obvious question.
“probably too CW to discuss here”
I’m not from around here, so to speak, so I don’t have a horse in that race.
That’s not how the math works out, as the effects could include more than one relative, including extensive kin networks, and the opportunity cost will be lower in situations where the total number of children is not limited by available fathers.
Yes, but the fraction of genes you share drops off geometrically in the distance along the family tree, as does the amount of help you can provide, so this is a reasonable approximation.
The fraction of rare alleles you share does drop off geometrically. I don’t see any reason the amount of help you can provide should. If you’re in a situation with large, communal extended families or a village where everyone lives very close together, it seems like it’s definitely not the case.
So, no, I don’t think it’s a reasonable approximation, especially in the case where the number of fathers is not limiting, which I hadn’t thought of before.
“I don’t see any reason the amount of help you can provide should.”
I do have in mind a traditional communal life with extended family and some kind of subsistence farming or hunting, in which case from what I can tell the limiting factor is how much food you can produce to feed children. If you can feed N of your own children and one wife, you could feed N+k of your nieces and nephews, where presumably k>1 while they are young.
Then wouldn’t you have to have k=N just to break even? My wife does have a healthy appetite, but… And the break-even k grows geometrically in distance, no?
As for less tangible forms of help, indeed I don’t think it drops off geometrically, but I also don’t see how you can provide many times more of it than if you had your own children.
” the opportunity cost will be lower in situations where the total number of children is not limited by available fathers.”
Sorry. I’d like to understand this, but don’t. Opportunity cost of having children? And lower for whom?
I have a childless older brother…and can confirm that the provides approximately zero help with my children.
Actually his influence on my fitness is surely negative if you account for childhood kicks to the groin.
Why is the gay germ theory more controversial than, say, maternal immune response? Both posit an exogenous environmental cause at a young age that causes homosexual orientation through damage to the child. The gay germ theory notably does not claim that homosexuality is in any way contagious.
Probably a belief that the ignorant public will react as if they had a contagious disease, making their psychological state worse.
Does the maternal immune response idea have, well, any non-circumstantial evidence at all supporting it? Because that would help, and the gay pathogen theory can’t currently clear that bar AFAIK.
I think also “it’s due to weird biochemistry in the womb” sounds a lot better and less threatening than “it’s literally a disease”. Which is not to say that the second one is necessarily false, but it explains why it’s more controversial.
Do any of the theories of the origin of homosexuality have any non-circumstantial evidence?
I suppose it depends what you mean by circumstantial.
Obviously we don’t have any experimental data to assess causality, but IIRC there are gene variants associated with a higher chance of homosexuality, for example. You could say a mere statistical association is only circumstantial evidence, but it seems better than postulating a pathogen nobody’s ever seen.
How not?
My understanding of it is that male homosexuality is the result of an infection in early childhood, either from a currently unknown pathogen or (more likely) as an uncommon side effect of a known pathogen. The infectious window would be long past for any adult gay men.
@eyeballfrog That would mean gay men can infect boys.
We already know that gay men can infect boys with Epstein-Barr, just like anyone can infect anyone with Epstein-Barr. 90-95% of people are already infected with Epstein-Barr. Would learning that Epstein-Barr causes homosexuality change anything more than when we learned that it causes narcolepsy and multiple sclerosis?
I’m no mental health professional but my impression is that the definition of “mental illness” depends heavily, if not entirely, on the criterion “does it impair functioning, make you subjectively miserable, or put you at risk of harming yourself or others.”
If you’re happy, functional, and not harming anyone then, almost by definition, you’re mentally healthy. Lots of gay people meet those criteria so it doesn’t make sense to describe it as a mental illness, at least not in and of itself.
Whereas the criterion you seem to be implicitly proposing, “does it seem to be rational behavior based on our current, limited understanding of evolutionary biology?” isn’t one I think anyone follows when determining mental health or much else. For example, is use of contraception a sign of mental illness?
@onyomi
While that is true, none of us function perfectly. So what gets declared a mental illness is extremely subjective, depending largely on what problems get considered normal and which are not, which in turn heavily depend on societal norms and constructs.
Nowadays we call rambunctious children mentally ill because they have trouble in school.
I’m not sure if this was a reply me, but I’m not proposing “same-sex attraction” (as the APA puts it) is a mental disorder, only that this shouldn’t be ruled out a priori, just as the APA says it shouldn’t be ruled in a priori. In fact, I have no idea what is a “mental disorder”, but I guess the operational definition must be “whatever it is that psychiatrists should be trying to treat.”
As for contraception, surely they are trade offs between quantity and quality, and different niches for different strategies. But it’s really hard to see where there’s a niche for zero children. So I’m merely suggesting that if there is some behavior which seems very difficult to make sense of biologically, then it is a reasonable hypothesis that there is some biological malfunction.
While we are at it, is voluntary celibacy a mental disorder?
If it’s truly voluntary, no, though it may be a symptom of a mental disorder.
The DSM 5 is what (in the US and most of the world) is used to diagnose whether something is a mental disorder. And while that book is the product of history and culture and a whole bunch of political wrangling, it’s also the product of some science and is fairly articulate about criteria. I’m not sure the best word to use for the process is “subjective.” Maybe messy, fraught, complex, imperfect. All of medicine is that way. And true enough, psychology perhaps more so than a lot of medicine.
The vast majority of disorders include in their list of criteria whether the symptoms are causing significant distress and/or impairment to the person. Having no libido or minority sexual preferences or any number of other less common human experiences does not qualify a person for having a mental disorder.
The DSM is used as the justification for insurance billing in the US and insurance billing requires that services be “medically necessary.” Optimizing individuals from an evolutionary perspective or just generally kicking people further into the center of the bell curve isn’t really the goal.
I think you are missing the point of the DSM, which is mainly to provide a list of diagnoses in order for doctors to apply treatment (presumably to remove, modify, or mitigate the condition) and to get that treatment covered by insurance.
It’s not that no one is interested in or willing to discuss the causes of homosexuality, it’s that the APA decided that homosexuality is no longer a condition that ought to be inherently considered a disorder to be treated. Thus it moves out of the scope of what the APA wants listed in the DSM.
I wonder, is excessive wokeness characteristic of medical (as opposed to the scientific) or American (vs European) conferences?
I’m not a big conference-goer myself, having only been to FENS among the notable ones, but I recall essentially nothing of this sort.
Any European doctors or American scientists here to compare the impressions?
Is FENS a neuroscience conference and if so, do neuroscientists really have a self-image as scientists, perhaps even ones that are more like real scientists than physicians (“medical… as opposed to the scientific”)?
It is indeed a neuroscience conference. As for self-image, I can only speak for myself and a couple colleagues, but there’s definitely a distinction between people doing just science (as in sticking electrodes into pieces of rat brains in my case) and doctors, who deal with sick people. Not that you can’t do both, but I think there are fewer such people out there.
What I meant is that do neuroscience researchers actually think that they are doing science and identify as scientists, akin to researchers in the physical sciences? That seems rather presumptuous. Medicine has a firm basis in basic science while neuroscience is more like a particularly soft and unrigorous branch of psychology.
That’s the opposite of how I’d see it, as a curious outsider. Interested to hear your justification.
At this point could you please define what you mean by “neuroscience” here? While biology in general cannot claim the rigor similar to physics, I wouldn’t go as far as setting something like neuropharmacology below psychology. You take a drug, poke a receptor with it. However, I get the impression you don’t necessarily include that in “neuroscience”.
This was going to be more or less my response as well. I’m pretty electrophysiology counts as neuroscience, and it’s nothing like psychology.
Neuroscience literature is characterized by low statistical power that is not even remotely commensurate with the prevalence of significant effects reported. The same problem haunts psychology, too, of course, but the difference is that whereas this had led to many efforts at reform in psychology, neuroscientists seem to be completely unfazed by the cargo cult nature of so much of what they do.
I only know one neuroscience researcher personally, and he seems plenty concerned about the lack of statistical power of the research in his field. But a lot of neuroscience research is expensive, and the fix for low statistical power is bigger experiments, which multiplies the cost. So there’s no easy solution to the problem.
There are alternatives, such as multi-lab collaborations. Essentially, it’s a choice between cargo-cult careerism and real science and neuroscientists seem to be heavily in favor of the former. Here’s a good perspective; a quote:
The woke stuff hasn’t really arrived here in Europe yet. In Italy, where I live, most people roll their eyes when you bring up that stuff. In UK/Ireland, it’s a bit more taken seriously, due to US influence I would imagine.
I depends completely on where you are, including within countries.
Now here’s something interesting. You write:
“The people who talk about this usually go on to argue that the true causes of mental illness are capitalism and racism. Have doctors forgotten that the real solution isn’t a pill, but structural change that challenges the systems of exploitation and domination that create suffering in the first place?
No. Nobody has forgotten that. Because the third thing you notice at the American Psychiatric Association meeting is that everyone is very, very woke.”
Interestingly though, in your whole list of workshops, there is no reference to class, capitalism, poverty or the poor. There is one reference to inequality, but it is ambiguous and might be talking about inequalities of racial status.
So it seems like, to the extent that we have a politics here, it is is definitively ‘Socially liberal, fiscally silent’.
Not to be moralistic about it, but given the relationship between poverty and, say, schizophrenia, this seems like a pretty galling lacunae.
Score one point for Marxist theories of ideology?
Not that this undercuts your analysis, your reference to woke capital is very apposite I think.
Even if it was true, while I think it is an oversimplifcation because those big structures do not map 1:1 to personal misfortune and suffering, why confuse the job of the doctor and the political activist? Suppose you live in a dictatorship where the dictators goons beat up random people. What is the better use of a doctor, to heal the victims or to become the 10000th political activist trying to topple the system?
Probably some balance betwixt the options? The doctor’s primary goal should be healing, but I also assume a doctor is going to be better educated, better connected, better funded, more respected… generally having any collection of advantages over your average activist, whose only advantages relative to the doctor are probably time and fanaticism.
That’s not to say a doctor should be preaching to their patients about The Glorious Revolution, but in a bit of their spare time (10%, perhaps, would be fitting) they can promote it to their peers. I certainly take the thoughts of doctors I know socially more seriously than I do of any clipboard-carrying street activist.
Yeah, but part of this respect is based on the idea that they will help you based on proven medicine. I trust crystal healers a lot less than doctors, because I expect the latter to actually help me.
Activism typically involves believing that certain things are true or false far more strongly than would result from an impartial scientific approach, because it fits an agenda. In general, activists seem very prone to hypes that fit their ideological prejudices.
Yeah, but this conference is explicitly not limiting it to people’s free time, but making it part of a educational effort on psychiatry.
That’s the point of “woke capitalism.” Less “hey, how come CEOs make 400 times what a worker makes?!” and more “how come more of the evil oppressor CEOs aren’t women?” Less “income inequality” and more “racial income inequality.” Distract people from things they can change, like class, by getting them super worked up about things they can’t change, like race and sex/gender (with some exceptions).
To be fair to the left, groups like DSA often do discuss class in addition to all the woke stuff. I think the MSM (NYTimes et al.) doesn’t play it up because it would scare the people who advertise $10 million luxury apartments.
If I were conspiratorial in addition to cynical, I’d say that the media puts all the woke stuff in there to enrage downscale whites, particularly men, into voting Republican and enforce a system of racial and sexual polarization that splits the working class and keeps both parties bribable by capitalists. But…nah. They believe it.
Yes, I agree.
I don’t know about the doctor/prescriber side of mental healthcare as much, but on the psychotherapist side of things, we have an ethical duty to be concerned with people’s access to care, barriers to treatment (which include economic factors), and other ways that poverty might contribute to mental health problems. We also have some ethical duty, not clearly specified, to provide pro bono services and to advocate out in the wider world for the concerns of our patients (which would include economic concerns that are impeding their access to care). So I’d say an APA conference that doesn’t address poverty and mental health is failing a core ethical duty.
It’s not that we have to be “activists” on every issue. It’s that we have to be effective advocates for our patients in a world where poverty may significantly affect their health and their access to healthcare. In my practice, that means finding community resources for patients, coordinating with other service providers to increase access to care, educating legislators about access to care issues, taking continuing ed classes that address healthcare access and ethical issues, leaning on various government agencies to shake loose services, and arguing with health insurance companies where they are reluctant to cover necessary services. Even though we don’t get paid for that work, it’s very much considered part of the job.
Perhaps most of those are “fiscally silent”, but not “How Private Insurance Fails Those With Mental Illness: The Case For Single-Payer Health Care”. Granted, that’s specifically agitating for government involvement in the industry’s funding rather than addressing “root causes” of mental illness.
Non-consensual electroshock therapy is being used in a school for severely disabled children in Massachusetts https://www.theguardian.com/us-news/2018/dec/18/judge-rotenberg-center-electric-shocks-ban-inter-american-commission-human-rights
This isn’t ECT, it’s just giving people electric shocks.
True. They still claim it is a treatment where psychotropic drugs have failed.
Are they still around?
Can we make them be less around?
If I remember, it came up on reddit and the argument for the school basically boils down to:
Most of the kids there, pretty much all other options have failed.
The behavior involved is typically extremely serious and often dangerous to the individual and/or others.
So little Timmy is head banging all the time, he’s going to go blind if he keeps doing it from the head trauma.
You could let him go blind.
You could keep him drugged up for the rest of his life.
You could physically restrain him for the rest of his life.
Of you could shock him a few times when he tries to head bang in a very simple example of operant conditioning and it sometimes just works, stopping him from head banging and he doesn’t go blind and doesn’t need to spend the rest of his life restrained.
Which option is the least cruel and under which definitions of cruelty?
I notice that infants enjoy head banging. I also recall doing light head banging as a child.
Why do humans do this?
They haven’t discovered drugs.
That “Center for the Art of Lighting Up the Section of the Brain Responsible for Empathy” poster is so on-the-nose that it makes me think the artist must be a (current or former) brain science person having a go at bad cognitive neuroscience. It’s like the art installation version of this classic Neuroskeptic essay.
Blogger Paleo Retiree says the American genius manifests itself most distinctly in covering every possible surface with advertising.
I recall a press release for a startup that was going to cover the inside of the cup on every golf hole with ads.
Do Sand Hill Road VCs play golf? If so, that seems like maximally efficient targeting of your real audience.
Your section about the woke panels reminded me…. are you seeing people in psychological trouble because of climate
changeemergency, crisis or breakdown and/or Donald Trump?I think it was you, Nancy, who first alerted me to the idea of “progressive ideology as CBT in reverse.” Instead of recognizing one is catastrophizing over trivial issues and stopping yourself, the media takes trivial issues and informs you they are in fact a catastrophe. In fairness right-wing media does this too, but there’s a lot less of it.
My wife’s best friend is going through a divorce, partially as a result of media-induced hysteria over Trump and climate change. After the election she became alternately anxious and depressed over everything to do with politics and climate change. Her husband, who’s also a Democrat but…perhaps more cynical about politics found her impossible to talk to so for the past two and a half years and just…stopped talking to her. And now has started divorce proceedings. High school sweethearts, married over 20 years, 2 kids. And it’s over, he’s already made up his mind he doesn’t love her anymore. I really hope some of those programs were about talking to people who are too worked up over politics and calming them down, and not about terrifying them further.
I’ve heard people mention ideas like this before and it sounds like an astute observation. Anywhere good I could read more about it?
The book “The Coddling of the American Mind” by Greg Lukianoff and Jonathan Haidt talks about this.
If you’re outraged you’re paying too much attention.
Can confirm I’ve noticed this trend too. At least once a day I notice a headline using the word “terrifying”, something I didn’t recall seeing before on sites like The Guardian. It’s like they’re getting themselves and their readers into a fear frenzy. Although, right wing news sites like the Daily Mail have been doing this for years too, just over different subject matter.
Fear was traditionally a tool of control on the right, interesting to see its emergence on the left too.
I see this with my grandma. She’s generally non critical, and so she’s slowly becoming more and more fear-driven as the media feeds that stuff out.
I have a coworker who I got along with well tell me the other day that Pizzagate was a false flag for the *real* child sex ring being run by Trump’s people using captive immigrant children.
I’m not sure it’s quite so new.
My grandmother died a decade ago and never used electronics more complex than the non-smart home telephone.
She did however read broadsheet newspapers constantly.
Towards the end of her life she gradually became terrified for my cousin because she was convinced that the streets of the local cities were basically constantly awash with blood and violence. They weren’t, at least no more than when she herself was young with occasional drunks fighting… but getting all your impressions of the world from the news is a terrible thing because they primarily talk about terrible things.
Most of the time ignorance is bliss and people are, by default, mostly ignorant of the low key violence going on around them.
People don’t seem to cope well with getting informed about all the awful things that are happening, even just within a few-mile radius.
I freaked out one of my work colleagues by showing her the online london crime heatmap: you can view a map of all crimes in an area over any particular month, suddenly she learned about all the fights within a few miles of her house all at once.
It didn’t change her home in any way, it’s no more or less violent than before but now she knows.
It’s a nice observation. I was familiar with the principles of CBT growing up (even once saw Albert Ellis on the East Side!) and remember vaguely thinking when reading about a lot of this stuff decades later, “This is the exact opposite of the the stuff I’ve been reading.” Never quite made the leap to thinking of it as anti-CBT though.
Also, Nancy, if on the off-chance you’re the one who sold me a few geeky buttons at Arisia 10 years ago, I’ve still got them.
Somehow I’m reminded:
“The second night’s audience, by contrast, was the weirdest I’d ever played. They were abnormal from the very start, and when we found that we were not getting the laughs we were accustomed to, that threw us. Then some of the audience started laughing at things no one had ever previously laughed at. Once they roared at the set-up of a joke and then received the punchline in complete silence. We were bewildered, but struggled on desperately towards the final curtain, and when it came down we went into collective shock, trying to understand what had gone wrong. Michael was soon there with the explanation. Every ticket for that performance had been bought for the attendees of a conference that was being held in London. A conference of psychiatrists. There had been a shrink in every seat.”
– John Cleese, So Anyway
What does the Hun know of psychology? His most stupid, thick-witted performance was his brutal defiance of the United States with its wealth, resources, and energy. That revealed a mental condition both grotesque and pitiable.
OK, maybe Dr. Anglin got a little carried away. But going to war with the United States twice in a quarter-century does seem kinda nuts.
I’m not as familiar with WW1 as I am WW2. My understanding is that US involvement was something the president wanted and had to convince his countrymen to go along with it. So calling someone crazy for going to war with an enemy they did not actually choose seems a bit disingenuous.
One could make a case that the Schlieffen plan (sp?) was crazy but given that a far away neutral power ended up declaring war on Germany, it’s possible Britain would have entered the war on France’s side regardless of what happened to Belgium, but like I said I’m a nonexpert on that part of history.
I do always wonder whether holding the French at the franco-german border and going after Russia would have been better if it kept Britain out of the war for a few months, but going through Belgium and northern france captured a fair portion of French industry so IDK.
With WW2 IIRC the declaration was done to remove the shackles that had been put on the uboats because the US ships were *technically* neutral. Also they weren’t expecting the US to focus on them until japan had been dealt with.
US Manpower was not the deciding factor in the European theatre in either of the world wars, it was the war material they supplied which I imagine was easier to destroy if you were at war with the state that was supplying it. The war was already lost by the summer of 44 anyway.
I can’t say for sure what Britain would have done if Germany had invaded France without going through Belgium, but the Germans had pretty thoroughly burned their bridges with the British by 1914. The whole naval arms race was basically Germany challenging the British on something negotiable to Germany and nonnegotiable to the UK. This raises all sorts of suspicions, and if you’re going to invade the UK from the continent, you probably want to do so from Belgium, because you’ll land on the plains of East Anglia, which are terrible defensively.
This, unfortunately, was probably not feasible. The problem is that Russia’s size sets a fairly hard lower limit on how quickly you can conquer that country, and that limit is a lot higher than the time required to take out France. Remember that the German high command mostly served in the Franco-Prussian War, which they effectively won in 6 weeks. If you expect that kind of performance, then the Shleiffen Plan makes a lot of sense.
Not really. Wilson was constitutionally unsuited to conduct international diplomacy, and he seems to have genuinely wanted to keep the US out of the war, and to achieve “peace without victory”. (All this did was delay victory 25 years.) When the Germans kicked off unrestricted submarine warfare again, Wilson changed his mind and brought the US in.
And yes, propaganda from that era is usually hilarious in its obviousness.
This sounds like you are saying that there wasn’t a victory in WW1.
Pretty much. Wilson screwed up the postwar situation so thoroughly that a second round was inevitable from the time the ink on the Treaty of Versailles dried. Particularly if your announced goal is “the war to end all wars”, that doesn’t look like victory to me.
When you say it wasn’t feasible I’m thinking about it in terms of what we know in hindsight. I don’t disagree that the Schleiffen plan was logical to the people who made it at the time.
1. For a brief period the western front would be narrower for Germany and Germany would face fewer troops, both of which are advantages to the defender. Germany would have also had a few months to fight without being blockaded. The Eastern front allowed for the kind of mobility the Germans were accustomed to whereas on the western front circumstances would have favored the defense.
2. Germany was ultimately able to force Russia to sue for peace [historically]
3. Germany would have been able to allocate more men on the eastern front than they had to “defeat” Russia historically because of #1
With perfect hindsight, maybe you’d go for Russia first. But given what they knew at the time, I don’t think that’s a viable option. Russia is never going to go down quickly. Barbarossa was more successful than any potential invasion in WWI could have been (because of changes in transportation), and yet it didn’t knock them out of the war. Only revolution did that, and those take a while to ferment. On the other hand, they came pretty close to winning in France in 1914. And pretty close to losing in the east, except for Tannenberg.
In WW I couldn’t Germany have first gone after Russia to capture some territory (like Poland), then destroyed the railroads and roads in front of their positions for a 100 miles or so and then with a good buffer against Russia gone after France?
I think the Russian army still walked places, and 100 miles isn’t that far for a marching army. Plus it’s easier to build up supply lines to a slow-moving army, so the buffer would probably not be a logistical issue.
Uhm 100km was about the range that the armies in the USAmerican Civil War could advance before their rail heads.
The problem would rather be, that destroying transport infrastructure in a way that need more than a few weeks to repair is really really hard.
“100km was about the range that the armies in the USAmerican Civil War could advance before their rail heads.”
Yes, but battles in the US civil war had far fewer troops and fewer supplies per troop than in WW I. How do you slowly march troops against concentrated German WW I artillery fire when the Germans can quickly move their artillery in place using rail roads?
The first paragraph of my answer was directed at Watchman.
Advancing 100 miles (160km) beyond one’s rail heads might be possible for an marching army. Fighting a sunstained combat with machine guns and modern artillery probably not.
But I’m doubting the abillity of the germans in 1914 or 1915 to destroy the infrastructure to an degree that the russians wouldn’t be able to rebuild it, in a couple of weeks.
I mean they couldn’t do it in 1943 and ’44
Yeah, what Germany needed in WWI was better diplomacy, starting well before the war, including more sensible behavior in a lot of respects (most dramatically not pissing off the British, but they made plenty of other mistakes as well). Of course, truly competent diplomacy would have averted the war rather than winning it; there’s nothing Germany stood to gain by war that was remotely worth the cost.
I’ve seen a good case made that WWI was essentially an attempt to unite Germany behind the conservative/Junker faction because the Reichstag was in danger of falling into the hands of the liberals. I’ve also seen a reasonable case made against it, but it’s not the most implausible theory in the world.
OK, fair enough; if they absolutely needed a war for domestic political reasons, I still think they underestimated the cost and would have been better off finding other ways to pursue their political ends. But if they keep the Italians on side, persuade the Belgians not to make a fuss, and avoid pissing off the British (mutually reinforcing projects; if the British and Italians are friendly, the Belgians may see less upside in putting up a fuss, and if the Belgians cooperate, that’s one less thing to piss off the British, etc.), then the Schlieffen plan might work. It failed by a surprisingly narrow margin; give the French an extra front in Italy and, more importantly, remove the BEF, and that might be enough to get rid of that margin. And so conceivably better diplomacy could have gotten them the quick war they wanted. And then Germany likely forces France to surrender a few colonies whose value is overrated, and Austria-Hungary gets a little more territory full of resentful troublemakers to add to the resentful troublemakers it is already struggling with. And so in short order people start questioning whether it was worth it, and the conservatives face challenges from the liberals all over again. So I still vote for no war (even apart from my lack of sympathy with the conservatives).
Oh, I’m not defending it as a good plan. The idea of going to war to cement national unity is, at the very least, extremely dangerous. The last time someone pulled it off (at least in Europe, results may not apply in the 3rd world), it was Bismarck in 1870, and nobody running Germany 40 years later was nearly up to his caliber. Since then, we’ve seen spectacular failures in 1905, 1914, and 1982.
I like Dan Carlin’s point about the war:
German diplomacy purposefully alienated Russia, so that Russia allied France. This meant that Germany was in a two front war position. Their solution was attack France as hard and fast as possible, and then fend off the Russians. Attacking Russia first would a) as bean said, take a long time, b) be not be worthwhile since there is not much to gain, c) eventually cost enormous casualties because Russia has so many people. Russia had weak infrastructure and essentially could not attack, because logistics were bad. These reasons meant that France, who had one of best armies at the time, a large international force of experienced soldiers and officers was the greatest threat.
Also, @James Miller and @RalMirrorAd
Some of your comments presuppose that Germany started/caused the war. That’s not right. Russia declared mobilization against Austria-Hungary first, and Germany’s could not sit around waiting for Russia to figure out how to transport food and troops to decimate their closest ally. AND as soon as Germany declared war on Russia, France could declare war on Germany.
Interestingly Hitler, and many Germans beside, were upset that the allies blamed Germany for the war. He called it Western Propaganda. I think even today, many people forget that Germany did not start WWI. So in a way, the guy was right. Dr. Anglin certainly ate the propaganda.
John, I have to disagree with you on this. Germany was absolutely responsible for the shape of the war as it turned out. They wrote the infamous “blank check” to Austria, which encouraged their diplomats to make all sorts of outrageous demands against Serbia. (And Austria didn’t have John Schilling in command to back things up, either.) Then, when this provoked Russian mobilization, they decided to go to war not only against Russia, but also against France because their war plans essentially rested on being able to mobilize faster than either of those two powers.
I’m pretty sure the General Staffs on both sides would disagree on this. The Russians did attack East Prussia, but Hindenberg and Ludendorff defeated them very comprehensively.
I don’t think the point was that Russia could literally never fight an offensive battle. Rather, that their logistics were too poor to support / exploit the sort of full scale sustained offensive that would be required to seriously threaten German interests. France was the priority threat that needed a quick defeat – Russia could be held off until the war in the West was won.
That wasn’t the crux of their plan. The crux of their plan was that Russia wouldn’t be able to mobilize fast enough to attack before they could deal with France. They were wrong about that, and were fortunate that Hindenberg and Ludendorff were around to step in and save them.
As for what was threatened by a Russian invasion, check the map again. The most obvious target for the Russians was East Prussia. To everyone else, it’s an awful, cold, barren stretch of land that no one in their right mind would really care that much about. But it was the spiritual (and often physical) home of the Junkers, and so had to be defended. (This explains a lot about the German aristocracy in the runup to the war, now that I think about it.)
I thought the Japanese brought the US into WWII, with the German’s frantically trying diplomacy stuff to keep us out of it.
Hitler declared war on the US after Pearl Harbor, for reasons that I’m sure made sense to him. If he hadn’t, Roosevelt would have been in a terrible position, because he saw (correctly) how much of a threat the Nazis were, but it would have been extremely difficult to go “The Japanese attacked us, now let’s declare war on Germany!”
I presume that Hitler declared war so they could sink lend-lease ships. The US effectively had already entered the war by supplying the allies.
I consider it likely that in the absence of Hitler’s declaration of war, the US would have kept enlarging their lend-lease program, resulting in either a declaration of war by Hitler once he had enough or submarine warfare against US ships, resulting in a Lusitania-style event that caused the US to declare war.
It was worse than that, because of Roosevelt’s “neutrality patrol”, where he essentially was using the USN to escort convoys halfway across the Atlantic. In a lot of ways, the US was the aggressor in the Atlantic until we provoked Hitler into declaring war. But that doesn’t make it a good decision. There were issues with Lend-Lease before war broke out, because it looked like we were shipping military equipment overseas when we desperately needed it ourselves. Continuing that program while we’re fighting a completely different enemy is, at best, politically difficult.
It wasn’t that stupid to declare war on the US. Really as soon as the US switched from Cash and Carry to Lend Lease the war was a foregone conclusion whether or not US soldiers were involved. Given the huge amounts of US aid flowing to the UK and USSR being able to take submarines which had been preying on relatively well defended Atlantic convoys and send them to massacre undefended US coastal shipping worked out really well for Germany in the short run. This cut down on US production and the US entry and military buildup cut the fraction of production going to Europe where it could do good in the short run. Given that Germany was already fighting one continental empire it would basically have to win quickly if it was going to win at all. So the short term benefit at the expense of long term danger involved in the declaration was arguably the right move. I could easily imagine Soviet troops in Berlin a year ahead of schedule if Germany had acted differently.
I’m not so sure of this. Yes, the Drumbeat campaign was a big problem for the US, but whatever dip it may have caused in deliveries of supplies to Europe was more than compensated for by the removal of all political constraints on Lend-Lease. You went from jokes about it being like loaning someone chewing gum instead of a hose to “yes, of course we will give our allies all the supplies we can ship them”. And that happened pretty fast.
You’d think so, wouldn’t you? But the Iraq War showed us that it’s not so hard.
Pretty much. If we imagine the Third Reich is absolutely scrupulous about never shooting at anything that might be flying a US flag, then they eventually lose for about the reasons Andrew notes. It may take a few years longer than he suggests, but in the end we can always find non-American bodies to actually shoot the guns we produce for Nazi-shooting. If the Third Reich is not so scrupulous, then here’s the crew of the Reuben James 2.0 to show that the Germans did so attack us, clearly in league with their dastardly Japanese allies.
What Hitler should have done after Pear Harbor was to declare war on the Japanese.
“You and what navy?”
The one he gets from America under lend lease, of course.
I assume that’s a joke, but no. If Germany declares war against Japan, and does not meaningfully attack Japan (hint: they can’t), then this is dismissed as a silly meaningless diplomatic ruse.
In the unlikely event that Germany does meaningfully attack Japan, great, America’s enemies are fighting war against each other and we’ll help neither while fighting a holding action against the one while providing free munitions to our allies fighting the other and gearing up to wage total bloody war against them both sometime in 1942.
When I saw his name, I wondered if he had a distant descendant who was even more xenophobic and entirely too Germanophilic.
This seems like a good post to ask this: I’ve recently watched a couple of documentaries on the Rajneeshpuram movement. One mentions that a key demographic for them was California psychiatrists. This documentary cited that something like ten percent of the group in the 1970s were Californian psychiatrists and their families. I wonder if Scott has ever heard about this, or met any of these people. I couldn’t figure out what about this particular cult specifically appealed to psychiatrists. Any insights or theories?
I’d never heard of these people before (okay, I vaguely remember someone named “Osho” being involved in a cult scandal, and Wikipedia says that was these guys). Based on PIHKaL, I get the impression that California psychiatrists a generation or two ago were a hotbed of hippie-ism, but beyond that I don’t know.
Bending spoons with your mind in the early 1970s was big among California aerospace engineers, as was the amazing Pyramid Power pyramid scam in May 1980.
That particular statistic sounds dubious (maybe less so if you substitute “therapist” for “psychiatrist”, California was and is full of new-agey non-medical therapists who would be drawn to something like that), but apparently 36% of the population had graduate degrees, which is kind of amazing.
I’d be curious to know what attendance looks like at all those wokeness panels. Just for comparison, PAX has been getting progressively more woke over the years, but the woke panels usually have single-digit attendance. My impression is that many of these panels are just fig leaves, designed to deflect at least some of the inevitable social media outrage.
Sorry–what’s PAX? Google turns up a company that makes vape pens.
PAX is a (series of) convention(s) centered around video and tabletop games, having arisen from the community around the webcomic PennyArcade – hence the acronym (X for eXposition), though PAX might not officially stand for anything anymore.
Ugh. I stopped going to PAX 5 or so years ago, partly because the panels gave me the distinct impression that, as a straight white male, I was not welcome. I wanted to go there to celebrate gaming; I did NOT want woke politics shoved in my face. I imagine it’s ten times worse now.
Speaking of gamer culture:
Nice to know that if you’re an incel, not only are you miserable, desperately lonely, and at high risk of suicide, but at least if you go to a psychiatrist they’ll … also treat you like an enemy. And they have the power to imprison you.
FWIW, PAX (what is now called PAX Prime) used to be a truly welcoming place during the first couple years of its operation. But recently, it’s become a lot more like this APA convention: slick, corporate, woke, and totally soulless.
I’m guessing they’re not familiar with Betteridge’s Law.
I will extend some charity to the Wokepersons who hosted this panel. They’re not saying “involuntary celibacy: prescription for violence?” but the combination of inceldom and misogynist ideology. How well they adhere to that distinction, who knows.
“Incel” gets used without differentiation, but I think there’s two main groups. There are people who are unable to find a sex partner and either cope with it or try to improve themselves to the point they can find a sex partner, and then there are people who, because they are unable to find a sex partner congregate on internet forums where they blame all their troubles on women/society/genetics and get incredibly angry and resentful.
If you’re a guy who’s a 1, well, you’re probably deformed and have lots of other problems beyond sex. But for anybody else…a guy can move up 3 points with some effort. Get a job so you can support yourself and buy some clothes that fit. Exercise. Find a homosexual to cut your hair. Then a guy can start out as a 2, do that and work his way to a 5 and he’s within spitting distance of a girl who’s a 6 and that ain’t bad! It’s the guys who are 2s, are really mad about being 2s, and stew over it where you might get a problem.
@Conrad Honcho
My experience with feminist responses to men with dating problems is that they tend to assume that the men lack success due to excessive misogyny, aggression, being too controlling, etc. So the advice tends to be really poor if not actively counterproductive if the man’s problem is that he believes in equality too much, is not aggressive enough, is not proactive/controlling enough, etc.
Let’s just say that I have my doubts whether a panel with that title is going to encourage psychiatrists to give good help to many men with dating problems & whether they will be open to the idea that misogyny may be a result from bad dating experiences, rather than the cause.
My impression of incels, or at least the ones on wizardchan, /r9k/, and the weirder subreddits, is that they are people who have a lot of issues with self-image and with sex in general, who mistake their internal issues for external ones.
They don’t want to pay a prostitute, to sleep with unattractive people, to spend hours watching PUA videos and practising, or to hook up on Tinder by playing a numbers game. They usually don’t even want to sexually assault anyone. What they really want is to be validated by a relationship or by a chance sexual encounter, but they’re so low in confidence that failures hurt them very badly.
I’m not sure the woke left really understands incels. Their analysis sees the root of the problem as mysoginy, when I think it’s projected self-hatred.
If all you have is a hammer, everything looks like a nail.
I would say the cause of that self-hatred is very low self-esteem & high neuroticism, where they see no path for self improvement that makes them worthy in the eyes of others.
Presumably, they didn’t see any results from tentative attempts to improve themselves, resulting in the conclusion that they have an unchangeable trait that makes them so unattractive that no (feasible) self-improvement can make up for it.
They typically seem to name themselves after that trait. For example, braincels/mentalcels believe that they are incel due to mental issues such as social anxiety or Aspergers. Ricecels/currycels believe that women strongly dislike not so masculine Asian/Indian bodytypes. Heightcels believe that their short stature results in no women wanting them. Baldcels… well you get it.
The irony is that women more often have low self-esteem & high neuroticism, and tend to more often be passive, so these most hated of men by feminists, who get accused of being the most toxically masculine men, are actually more feminine than the average man.
I only peeked into a few of the relevant rooms, but I agree they seemed pretty empty.
This strikes me as very important. Assuming that feedback mechanisms on panel performance are working, this means the event organizers ought to be selecting against them. (Maybe they already are? It’s not going to happen, but I’d be interested in seeing a breakdown of the submitted proposals.) But if event organizers are deliberately willing to harm the conference in order to promote more of these less-successful talks, that’s very concerning.
It also sounds like you didn’t actually go to any of these talks. That’s a shame, since it would have been interesting to hear if any were actually good on an individual level.
But even fandom conventions have mixed reception around panels.
For one thing, panel topics are prone to Sturgeon’s Law.
For another, there are basically only two kinds of fandom panels that get a good crowd: a reliably comedic one, and one featuring a famous enough guest.
Scott not going to any of the talks seems the norm in fandom conventions as well. I’ve seen people with the impression that panels don’t even exist at conventions, that you only go to buy things, gawk at the cosplay, and hang out with friends. Or in this case, have medical vendors shill at you so you might buy things in the future, and hang out with other attendees.
As panels are presumably offered by volunteering members rather than some sort of compulsory requirement all must provide in turn (although that latter model seems likely to get better panels) then this tells us little about APA as an organisation other than:
1. As everywhere what we appear to be calling woke activists are keen on expounding their message, presumably in the genuine belief that their views are key to improving colleagues’ practice and client well-being. Believers in any quasi-religiius theory (and by this I mean the woke ideals are seen by many as a panacea to loads of problems, and some followers believe they are combating evil; no judgement on their scientific merits is intended here) tend to be more prone to seek to and convert others to their ideas. I’d bet that in the 1970s APA was suffering a rash of quasi-Marxist and other leftish philosophical tradition papers for the same reason…
2. APA has a schedule to fill and is probably happy to fill it with anything in and around the Overton Window offered by their members.
Do we know if this is true?
Regardless, I find it interesting that an offering of voluntary to attend panels that he does not like is so offensive to Scott.
I wonder if what is going on here is more disillusionment, the assumption that these large organizations are supposed to be uniformly oracular fonts if knowledge, rather than composed of … people. And the realization that not all of those people are marching in lockstep towards the priorities that Scott finds important.
I think it’s more like they’re marching in lockstep towards priorities that…don’t really have much to do with the practice of psychiatry.
This is Scott “freedom of expression is sacred” Alexander offering this critique. Scott “argument gets counter-argument” is saying he thinks it’s wrong that people are even making these arguments.
Perhaps he is right. Maybe it is dangerous that many people are making these arguments. Honestly I don’t know enough about this conference, nor the ACTUAL arguments to assess. I suspect that Scott doesn’t actually know either. But,assuming he is correct, then maybe he should reassess other stances.
I don’t think that’s a fair assessment. Scott isn’t demanding these people stop speaking, he’s questioning the venue. If you go to a physics convention and they have a bunch of talks about needlepoint techniques, asking wtf they’re doing there isn’t coming out swinging against the freedom of expression of needlepoint enthusiasts.
Being in favour of freedom of expression also does not require you to applaud any expression of any kind, anywhere.
There are worlds between taking active steps to silence someone and disagreeing with their ideas. Or judging those ideas to be of poor quality.
Heck, a healthy marketplace of ideas requires disagreement.
Wait, where does he say he thinks it’s wrong that people are even making these arguments? Where does he say it’s dangerous that they’re doing so?
I certainly don’t see him saying these sessions should be prevented, which would be the thing that would actually be inconsistent with his stated beliefs.
Counter-argument gets counter-counter-argument. All is right with the world.
Well, no, at least one of the arguments is wrong. But we’re all still talking here, not banning or facepunching, and nobody is trying to change that.
1 – I don’t see any counter argument from Scott. He doesn’t actually present any argument to counter. Just a vague nodding at how awful it is that there are people who approach psychological care from a position that is [boo light]woke[/boo light]. It’s the kind of thing that Scott generally is against, and in fact frequently blogs specifically against.
2 – We have people elsewhere in these comments who say they feel that they should not seek pychological care, that psychology may not even be a real profession, that Republicans should not seek care, based on Scott’s comments. His comments are not being perceived in a neutral manner.
I really liked Scott’s post here, and I also agree with HeelBearCub that it may lead someone with conservative leanings who is outside the profession to feel like they are at risk of being the target of political conversion when they’re just trying to get help with a mental health issue.
I have never in my life heard tell of a patient who was upset because their mental healthcare provider was imposing lefty positions on them. I’m sure it has happened, but I hear a zillion critiques of all kinds of healthcare professionals from clients and that has never been one of them.
It’s not that they’d say that the right was the problem.
It’s that they’d not say it, but be thinking it all the while.
Isn’t that the argument?
I might be wrong, but I understood Scott’s point to be something like, “The volume of tangential political stuff is too dang high”.
It might be that those topics are not really tangential(see counter-arguments in the comment section to that effect!). He admittedly doesn’t go into a ton of detail on this, but this section feels like it’s mostly a joke so I am reluctant to hold Scott to such a high standard.
@spookykou:
It’s the kind of “joke” where you sneer about the “macho” topics at FFA convention.
And note that there are a number of people in the comments section who have taken this completely 100% seriously,and are stating as fact that psychologists are left-leaning and can’t or won’t provide care to conservatives.
@HeelBearCub
I would be very surprised if American psychologists were not left-leaning as a group. The educational attainment required to become a psychologist pretty much assures this, based on the pew research data I have seen.
That some people on SSC are terrified of the woke left isn’t exactly news, I would be shocked if there was any treatment of that list of panels that Scott could have offered that would not have generated at least some of the responses you are talking about.
Still I think he makes an argument, and that argument is open to counterargument. Even if it is a bit lazy.
I don’t know what FFA is, but I think I take your meaning there all the same. On the one hand I do think it is possible that Scott might get upset at a Vox article for making a joke similar to the one he made here, but I think mostly he would be upset if the whole point of the article was bashing macho-ness in FFA, or in society in general, and this was just one more in a list of potshots that culminated in an article titled “Macho Madness” or something. This post is making fun of the APA, it makes fun of the APA for a lot of things, woke-ness just being one of them. I don’t think I can fully articulate why, but that seems like a substantive difference to me.
The FFA apparently is holding rodeos at their convention this year, but that’s entertainment, not intended as a presentation.
Their 2015 convention had some political stuff, like a session called KNOW Hunger “Learn what it takes to live on a SNAP food budget”, and one about “becoming a beef advocate”. Also such macho topics as “Vet Tech Urine Checks” and “The Livestock Dating Game”.
I thought that already (more “can’t” than “won’t”), but this post is about psychiatrists, not psychologists. However, the New York Times does tell us that indeed psychiatrists _are_ left-leaning, on the whole.
@SpookYou
The FFA is the Future Farmers of America. According to their website: “FFA is the premier youth organization preparing members for leadership and careers in the science, business and technology of agriculture”.
Pretty interesting how I’ve never heard before of the biggest youth organization in the US, with 670k members. It probably says something about how isolated the blue tribe-based media culture that I get exposed to is from red tribe culture.
Interestingly, 3 out of 4 articles on the homepage of the FFA are about women in the FFA. Quite macho indeed.
@HeelBearCub
I think that professional conferences are reflective of the culture and concerns of the profession and the organization running the event. This includes what they consider acceptable at the conference, including:
– how much they let money dictate the experience vs quality (or other) concerns
– how much they accommodate (specific) activists
– what kind of entertainment they consider appropriate
– how much room they give to established best practices vs speculative new stuff
The high level of wokeness at this conference probably reflects the extent to which psychiatry is an outlier in medicine with regard to political leaning, suggesting that the profession has a high number of far-left practitioners.
Scientific studies have found that far-left and far-right social psychologists are much more prone to discriminatory behavior based on their politics. Furthermore, large parts of society dislike the social norms of the far left. There is a lot of evidence that people on the right wing feel oppressed by how people on the left react to them and a decent amount of evidence that this is not (only) oversensitivity, but due to hostile behavior by those on the left.
It is a fact that psychiatrists are far more left-leaning than other medical professions, as I’ve shown earlier in this comment. Presumably, the right-leaning types are more likely to be found in rural/red areas, but many of our concerned SSC-citizens live in urban/blue areas where psychiatrists are probably even more often left-leaning than the NYT-reported data shows.
Studies also show that conservatives tend to be different from progressives on how much openness to experience they have and how conscientious they are. This determines people’s goals and morals.
It seems quite plausible that progressives tend to have a harder time understanding conservative needs, in the same way that extroverts have a harder time understanding the needs of introverts. Furthermore, they may consider conservative desires to be immoral. For example: they might consider a man who only wants a stay-at-home partner to be controlling and abusive, but not a (wo)man who only wants a working partner. They may be eager to attribute unhappiness in a woman who is a stay-at-home mother to her not working, but may be far less eager to attribute unhappiness in working mothers to them working.
@Aapje:
Let me get this straight.
Your position is that discrimination, in the “unjust or prejudicial treatment of different categories of people or things” sense, is real, it is harmful, and requires special awareness to combat?
And that people in position of authority or power, especially those who come from a majority culture on those positions with sometimes discriminatory views of the minority culture, have a special duty to avoid furthering that climate of discrimination?
@HeelBearCub
“Unjust treatment” begs the question, but yes, it exists. So does prejudicial treatment, which partially overlaps with unjust treatment. Most prejudice is at least partially correct on the group level (as scientific studies have shown) and acting on prejudice often has upsides as well as downsides. In fact, it is quite common for people to court the prejudice that they want (and create prejudices that benefit them), for example, by how they dress, act, etc. A gay man who plays to a gay stereotype can get themselves be approached more by gay men who prejudicially assume that the person is open to a sexual overture by a gay man. This can then be a major advantage, reducing the chance that people end up alone and unloved (and reducing the chance of gay bashing by a heterosexual man who is approached mistakenly), thanks to helpful prejudice.
So I believe that prejudicial treatment can be an overall good for society if the benefits outweigh the costs or it can be an overall bad if the costs outweigh the benefits. A true prejudice-free society would almost certainly be a horrible dystopia that no normal person would want to live in.
I believe that the contemporary (ostensibly) complete rejection of prejudice is not merely ignorant, but also something that people don’t really consider just if applied consistently and something that people don’t actually practice when they consider the prejudice to be an overall good.
Note that in practice, people typically categorize based on moral judgments, rather than by objective definitions. So instead of arguing that some prejudice is bad and some is good, they call the kind that they object to “prejudice” and deny that the kind that they like is prejudice. But this just results in begging the question.
So given this ground work, I can answer your first question(s):
– prejudice and such is real
– some of it is more harmful than beneficial overall & the benefits and harms are not necessarily distributed evenly
– I favor actual open discussions (and study) of the upsides and downsides of certain forms of discrimination/prejudice & recognition that it is a grey area, not black and white. I also favor recognition that the very same prejudice can benefit one group and harm another. These are probably completely different kinds of awareness than the kind that you were thinking of.
I don’t consider the majority/minority distinction to be inherently useful. This is correlated to power dynamics, but only imperfectly. “Dominant” is much better. I also don’t like special duty, as the weak also have duties. So I’ll use “greater” instead.
I think that the dominant culture has a greater duty to ensure that non-dominant cultures have the freedom make a case for and against prejudices that they favor and oppose.
I also think that the dominant culture has a greater duty to ensure that the needs and desires of the weak are fairly catered to, instead of oppression of the kind described by the quote: “Democracy is two wolves and a sheep voting on what to have for dinner.”
Note that dominant and weak are contextual. The very same group can be dominant in one context and weak in another.
@Aapje:
That sounds pretty darn woke.
Unless you only mean this to apply only to conservative, White people, which I don’t believe you do.
So, I think it’s certainly fair to say that it’s a professional duty of psychiatrists to ensure that they are providing proper care to their clients regardless of their political affiliation (no, this is not an invitation to jump the shark and ask me about treating those affiliated with the military wing of the IRA or ISIS.)
But it’s also fair to ask them to be aware of discriminatory practices regarding other non-dominant parties besides rural patients, particularly ones who have traditionally received inadequate or discriminatory care.
Nor do we have any particular evidence that this conference had no sessions that related to the needs of rural, exurban or conservative patients.
I believe the full listing is here
They have kindly listed everything that would be CW as “Global, Political, and Social Issues.” That category comes pre-corrupted. You know what you are getting. (Mini-EDIT: There is another called “Community Psychiatry” which you might not tell from the title, but is all the same stuff. Basic Income is now part of psychiatry.)
The one labeled “Ethics” seems more likely to be both a) corruptible and b) worth corrupting. I took a look. One thing about the death penalty. One about reporting to law enforcement. [1] Out of about 12. Not too bad.
There are tracks about addictions (“opioids” turns up ~18 times on the page) and religions. Only one I could find about rural communities based on the word “rural.”
[1] Also “To Write or Not to Write: Ethical Issues for Clinicians Writing Fiction, Personal Narrative and for Popular Media” which felt like it was chaired by Scott, but, nope.
As mentioned, ~20 sessions on opioid abuse.
There are also ~10 sessions specifically treating the military.
There also several sessions on political polarization or general cultural inclusivity.
There is also the session specifically about treating people who threaten the president (if Scott’s coding anything that deals with guns as woke, that is the opposite).
@HeelBearCub
The woke typically seem to favor one or more specific groups and then demand that prejudices are used when in their favor, but not in their disfavor. For example, women/society may apply negative prejudice to men, like assumptions of guilt in Title IX courts or ‘Schrödinger rapist,’ but men/society may not apply negative prejudice to women, like assuming that certain behaviors by the alleged victim make a false allegation substantially more likely.
Such an approach, where the benefits of applying prejudice are maximized for a favored group, no matter how much harm that does to a disfavored group, is oppression, not fairness. Fairness is balancing the harms and benefits somewhat equally.
The devil is in the details here. What is ‘inadequate or discriminatory care’? The answer is not going to be value-/ideology-free.
You can search the program yourself, where it seems to be best to do it by presentation title, not the default search option: keyword. I found 50 presentations with ‘rural’ in the title, so too many to list here. Some of these are part of the same session. So the number of sessions is less than 50. At first glance, they seem friendly to rural folk.
The results for “conservative” were a lot less impressive, at 2 results:
– Leveraging Cognitive Consistency to Nudge Conservative Climate Change Beliefs
– Navigating Disclosure of Sexual Minority Identity for Men in Socio-Politically Conservative Areas
Both of these seem to be hostile to conservative beliefs.
@Conrad Honcho
Needlepoint is more of a mathematics thing. If you want to go to a physics conference, you’ll have better luck with knitting.
Psychology has always been political. Freud wrote Civilization and its Discontents, Adorno, Marcuse and Lacan all were influenced by psychoanalysis in various ways, Authoritarian personality in the 1950’s was discussed in the context of Naziism, etc. The DSM’s attitudes towards sexuality were definitely politically influenced.
Which is more important to the practice of psychiatry?
(a) ADHD
(b) Immigration
The correct answer is (a). But there are three times as many panels on immigration. Even if ADHD treatment has been fairly quiet for the past year, the ratio of attention seems very strange.
How many psychiatrists need MORE discussion and coaching on the state of ADD diagnosis and treatment, though?
If I go to an RDBMS conference, I don’t expect there will be too many sessions on primary key – foreign key relationships, even though this is completely fundamental to an RDBMS.
ETA: and I definitely wouldn’t expect lots of different speakers addressing this issue. I’d expect some large session covering “fundamental RDBMS concepts” or “recent changes to fundamental implementations” or something like that.
How quickly does the state of the art change for primary-key/foreign-key relationships? How quickly does it change for ADHD medication?
I’d (weakly) expect the treatment of a major psychiatric disorder to have enough research into it that there would be important sessions on the topic every year.
I don’t think many people at, say, a major virology conference will go “what, MORE research on influenza? Booooring.” It’s important, and there’s always something new.
ETA: I largely agree with your ETA. Though it still depends on the size and fluidity of the field.
@Heterosteus:
Yeah, I largely agree with your comments. Put another way, I think it’s a mistake to go by “number of sessions and presenters” and not “number of available seats and attendees”.
Listing every poster presented at a scientific conference, as if they are all equally as relevant as the main session for the day, seems like a weighting error.
If I go to an RDBMS conference, I don’t expect there will be too many sessions on primary key – foreign key relationships, even though this is completely fundamental to an RDBMS.
I personally have taught sessions about primary key – foreign key relationships at DRBMS conferences, and have attended many more sessions on the topic.
And have been part of BOF sessions and Open Spaces sessions were we talked key types and relationships, and literally advanced the state of the art while doing so. (I used to work for MySQL AB, specializing in bespoke storage engines for specialized applications.)
Like most foundational topics, it has no limits to the depths one can usefully plumb and then teach.
@HeelBearCub
Studies have shown that younger kids get treated for ADHD/ADD significantly more often than older kids, suggesting quite strongly that immaturity is being treated (as well). So I would hope that there is still debate among psychiatrists about better diagnosis and treatment.
@Aapje and @Mark:
You are both arguing against a straw man, here.
I would expect new research, or ongoing harmful conduct, in a very large area like ADD research to receive star treatment, and be well attended. Ten pennies are not worth more than one dollar. Nor do pennies preclude the existence of some number of nickels.
HeelBearCub, I think you are being uncharitable to Scott. Universal associations of healthcare professionals (ie. associations which are not overtly partisan, like hypothetical “Democratic Doctors of America”) should not allow invasions of political campaigners or of pharma industry marketing on their official conferences, at any rate not to an extent described here.
So far as I know, sf conventions have more people who’d like to be on programming than slots for them. Anyone know whether the association finds itself needing to fill slots or needing to choose who gets to speak?
I’d image conference presentations look pretty good on a psychiatrist CV, so probably they aren’t begging for presenters.
And hey, they could always ask the Nigerian delegation to give a talk about the problems seen by psychologists in Nigeria. That seems like it would be both genuinely relevant, useful, and promote diversity.
I didn’t see a single thing on the right side of the Overton window. You know, panels like “Disemployment Shock, Employment Anxiety, And Resilience: A Public Health Perspective On Addressing Mental Health Impacts Of Job Loss“, or “Navigating Christianity: Addressing The Pervasive Role Of Anti-Christian Bias In Mental Health“, or “Transgender Care: How Psychiatrists Can Discourage Self-Injury And Provide Sex-Affirming Care“, or “Sucking It Up: Providing Care for the Traditionally Masculine Man“.
Of course, Scott’s list was selected to make the point that the conference was woke, so he wouldn’t have listed such talks even if they were there. But somehow I feel quite certain that they were not.
Exactly. Psychiatry is a bubble where the right half of the public’s Overton window is utterly unthinkable.
I think we can see how this narrowness of thought will lead to trouble treating half of patients.
Psychiatry is strongly coded left-wing, people who voluntary search psychiatric care are going to be overwhelmingly left-wing. Hence you get the people who get panic attacks because of Trump, climate change, etc.
Right-wing people either go to their priest, if they are religious, or on Reddit, 4chan, etc. if they aren’t.
Involuntary treatment probably consists in giving patients tranquilizers and antipsychotics and keeping them looked up for a week or so to make sure they don’t harm themselves or others.
…a subset of people who will receive psychiatric care. And if you think it is a good thing that some people get psychiatric care whether they “want” it or not, then it hurts your case if you let psychiatrists be perceived as ideological propagandists in one side of the culture war.
Likewise if you want to increase people’s willingness to seek voluntary psychiatric care when they’re not entirely sure they need it and also not entirely sure it’s safe to ask.
@vV_Vv:
I get what you’re saying, but that’s more psychology, yes?
Carl Jung proposed that the reason the talking cure worked so well even though Freud’s theory was fruitloops (and he’d learned from the master) is that it replaced talking to a priest in a secularized world. But priests can’t handle the pharmacology side of helping people.
I think there is a continuum between psychology and psychiatry.
If you are schizophrenic you’ll definitely need a shrink to give you meds, voluntary or not, and how woke this shrink is probably is not going to make much difference.
For things like depression, however, if I recall correctly, pharmacological treatments work more or less as well as psychotherapy, which is probably similar to what a priest/pastor/imam/etc would do. If you are a religious conservative having a common ground of shared values with the person who’s taking care of you is probably going to be beneficial.
“Right-wing people either go to their priest, if they are religious, or on Reddit, 4chan, etc. if they aren’t.”
I suspect a fair number probably go to the psychiatrist and roll their eyes at any leftism that gets dispensed with the drugs. I could be wrong, but I doubt your average farmer in Nebraska expects 4chan to do anything about his depression. Though I’d love to hear from some rural people.
Yes. When my mother was demented and dying, my shrink was very helpful, both through the talk and through the meds, but it was a constant battle to keep him on topic.
I do have to add that eventually he seemed to get it.
My understanding is that medical conferences are mostly a way for pharma companies to legally bribe doctors by buying them a holiday with paid travel, accommodation, food (including ice cream), and so on, and aggressively advertise to them in the process.
The talks are just fig leaves to pretend that there is a scientific purpose to the event. Nobody listens to them, so usually nobody really wants to give them, except woke activists who are always eager to push their ideology wherever they can.
Mine own ears have listened to people who work in mental health “healing” professions say in social events among people that they are sure agree with them that if they ever get a patient who is a vet, one of the main things on their todo list is to take away their guns.
And then see most of the people around them nod and agree as this is said. (It doesn’t help that more and more places are now allowing these “healers” to do such a thing with the stroke of a pen on 3rd hand say-so without even actually being required to have their victim be their patient.)
Gee, I wonder why vets don’t trust “therapists”?
There are many things I like about Seattle, and a few things I despise, and this sort of thing is an illuminating example of the sort of thing I despise about this place.
There hasn’t been a panel at a PAX that hasn’t needed someone counting the line for fire code in years.
I was at PAX East two months ago. It’s not PAX Prime, but I’m not sure it matters since it easily sold out. (In ~16 minutes after tickets became available, IIRC.)
While there, I attended a panel titled “Designing Asian Settings and Themes in Analog Games”. What I wanted was an insightful overview of Asian tropes as they appear in Western media, advice on common mistakes outsiders make when trying to introduce Asian elements, maybe a few ideas for a wuxia-style tabletop campaign. What I got instead was a below-average-quality sensitivity training class that almost focused more on gender and sexuality than on race, even. It was awful, and I gave some very negative feedback.
It was maybe at 1/3 capacity. And the next panel I went to hit capacity 80 minutes before start time.
My regular-con-going life lasted like 2 years because panel talk quality is so consistently BAD. People giving talks are bad at it, and audience questions are worse. A convention is one of the worst settings for holding a good discussion on anything.
With the exception of workshop-type panels, because of selection effects, but until I get into cosplay, those still have limited appeal. Music-centered panels are usually good, but rare.
I now only go to cons if I really, really like the music guest.
Took a peek at this year’s Fanime panel listing out of morbid curiosity, and good golly is it a wasteland. 4 days of content, and maybe 2-3 panels worth looking at. And no weapons workshops this year, either.
I agree with you above; I used to go to an awful lot of cons, and never spent much time at the panels. I’d systematically move through the dealers’ room and occasionally take pictures (always asking permission) of particularly impressive cosplayers.
Sorry if this is a stupid question — but to what extent is the American Psychiatric Association representative of psychiatry as a field ? Is it an authority that represents the current state of the art in industry and research, sort of like IEEE or ACM; or is it primarily a sales and marketing organization ?
I’m not too sure what you’re asking, but I think the APA is pretty official. For example, they’re the people who make the DSM.
Ok, in that case… wow. Just based on your photo-essay, I could almost conclude that psychiatry is barely even a legitimate discipline at this point 🙁 It’s probably not nearly as bad as it looks, but still, I’m fairly depressed now. Perhaps I should see a psychiatrist… oh… wait…
Yeah, I’m glad I don’t have need for a psychiatrist right now. I get the feeling if I were…I dunno, sad about my relationship with my parents (I’m not) they would tell me my real problem is that I’m a Republican. And to take Vraylar®.
I agree that this is fascinatingly weird. But professional conferences are notoriously bizarre. AMA or AAP (pediatrics) conferences are going to be likewise weird, but that doesn’t make all of medicine insane or worthless. The kind of folks who lead workshops or give lectures at these conferences aren’t really representative of the majority of the profession. And while it is indeed nuts the degree to which pharma gets to sell itself at these events, that’s the case across all of medicine in the U.S.
People who are sad about their relationship with their parents might do better to find a talk therapist. Psychiatrists are medical doctors who are specialists like an orthopedic surgeon is a specialist (in the U.S., that means MDs or DOs) who prescribe medication for mental illness. A tiny percentage of them do talk therapy anymore. Talk therapy is mainly done by psychologists or other licensed psychotherapists (MFTs, LPCs, LCSWs, etc). If any therapist told you that your real problem is that you’re a Republican, you could have their license for that… or at least file a serious complaint against them that would lead to sanction that would affect their licensing status.
@cuke
Yet the programmer conferences I’ve been to are a lot more normal than this.
That doesn’t seem like the expected way politicized therapy might go. I’d expect a bias to blame the person’s misfortunes on their racism, misogyny, etc (or if they are ‘of color’ or women or such, the racism, misogyny, etc of others). In itself such a claim is not absurd. There are people who are (so) racist, misogynist, etc that this causes problems for themselves and there are people whose problems are due to racism, misogyny, etc by others.
So a misdiagnosis is then not going to result in an automatic sanction for misbehavior, if someone complains, because it all depends on context. The medical board is surely going to give the therapist the benefit of the doubt, to such an extent that the misdiagnosis has to be truly absurd for them to get a sanction.
Aapje, walk me through what a misdiagnosis of the kind you describe would look like? I don’t have a sense for what you’re imagining.
Remember, diagnosis refers to what’s in the DSM 5 and is used for insurance filing purposes to justify why treatment is medically necessary.
This, but with the psychiatrist having Marcotte’s ideology, chastising Scott A for being misogynist and prescribing chemical castration drugs.
Aapje,
Racism and sexism aren’t diagnoses and psychiatrists and therapists don’t have tools to “treat” them. You can’t misdiagnose someone with sexism. You can misdiagnose someone with depression when they have bipolar disorder.
If a feminist therapist tells their patient that the patient is depressed because of their sexism, the patient will have received an unhelpful assessment. The therapist will have violated their ethical codes. What follows from that is hard to say, but it’s hard for me to imagine how chemical castration would follow from that. I can see this producing what Ozy described here in this discussion, which is a person leaving a therapist’s office feeling angered by an unskillful provider.
@cuke
A fairly common and IMO legitimate criticism of psychiatry is that they have a tendency to threat symptoms, not the cause. For example, if someone is in a depression-inducing situation, they tend to treat the depression, but not the cause. The only way to do this is to numb people, so they can endure the pain better.
In effect, this makes them better at being victims, instead of ending their victimization.
A somewhat similar problem exists with feminism, which largely doesn’t want to truly address the cause of ‘toxic masculinity,’ because it would mean that women would have to give up benevolent sexism, which feminists typically don’t want. So they also tend to address the symptoms (like stoicism), without addressing the cause (female desire for stoic men & providers, etc). The end result is that they harm men: men who listen to feminists start acting more feminine, in a way that works for women, but not for men.
The men who open up about their emotions don’t get the sympathetic response that women get when doing the same. They get bullied by men and women & dismissed by women as potential partners. Men who let it get to them when they are turned down again and again by women, often end up not approaching women in the way that they want to be approached, resulting in romantic failure, which often results in loneliness and such.
So their lives simply become worse. It’s not even necessarily good for women, because:
– the loss in ‘toxic masculinity’ is accompanied by a shortage of men that approach women how they would like to be approached and by men they want to date.
– men who figure out that they’ve been (further) victimized by feminists can get very angry & radicalized
So, add feminism to psychiatry & one can expect that for male help-seekers, psychiatry will become even more prone to not address the cause, but to perpetuate or even worsen the victimization of men.
@Aapje:
I, like you, enjoy coming up with general theories to explain the world. I’ve learned, though, that the one place it doesn’t help me at all is in relationships, because there are lots of different kinds of people who are attracted to lots of different kinds of people.
However, if you’d prefer a competing general theory, I remember a couple of “PUA gurus” talking about how they had the most success with women once they learned to share their emotions with women. They theorized that women were attracted to it because back on the savanna it’d only be the most socially dominant men who’d be willing to share their emotions, given all the risks that entails.
I’m pretty sure both your theory and their theory are Just So stories, but you might enjoy adding it to your mix of ideas.
@Aapje
The feminists I’ve talked with about this have mostly said that they’re looking for emotional intelligence (or a demonstrated willingness to work to become more emotionally intelligent), rather than low self-esteem and neuroticism. Part of what they see as toxic about toxic masculinity is that it tells men that emotional intelligence is something that’s only for women. Those feminists think that emotional intelligence should be for everyone.
But speaking of neurotic men… I think that catastrophizing theorizing (like you’re doing) has discouraged a lot more of them from ever approaching a woman than actual experiences of approaching and being rejected. There are probably a lot more women who’d like a neurotic partner than are getting them, because those men are being discouraged by people like you, and aren’t even trying.
Let me suggest a different analogy.
Imagine a patient who is a fundamentalist Christian. He gets referred to a psychiatrist who is an atheist. The psychiatrist is not permitted to turn the patient down on account of his religion. Further, in treating the patient, the psychiatrist is legally required to pretend to share the patient’s beliefs. If the patient says “the reason bad things are happening to me is that I am a sinner,” the psychiatrist has to act as though he believes it. Being a sinner suffering for his sins is part of the patient’s identity, and the psychiatrist isn’t allowed to question it.
That seems to me analogous to requiring a psychiatrist who doesn’t believe that a transsexual patient is really of the gender the patient identifies as to accept the patient and to act as if the psychiatrist shares the patient’s self-identity.
Aapje, what happened to Scott Aaronson is symptomatic of a much larger problem than feminist bias. Whenever a patient complains that they’re afraid of hurting people in some way (hurting women with sexual advances like Scott Aaronson, a mother doing something that will lead to her kid being hurt, a driver worried about hitting someone with their car, etc.), the psychiatrist is supposed to SERIOUSLY consider OCD/ scrupulosity as a diagnosis. In practice, a lot of the time, the psychiatrist doesn’t. The fact that people who are afraid of hitting people with their cars are getting misdiagnosed as well was guys who are afraid of hurting women sexually suggests the misdiagnoses aren’t political.
@Andrew Klaassen
You seem to be supporting my point. Men do better with women if they are able to use emotions to get things from other people, aka emotional intelligence, which is not the same as just dumping your real emotions on people. The point is that emotional intelligence for men isn’t and can’t be the same as for women, because people respond differently to male displays of emotions than female ones.
Very neurotic men typically have to fake stoicism for a decent shot at a relationship. The idea that women are highly diverse in their needs and that men who do very poorly can succeed by not changing beyond the most superficial (like dressing nice), is fairly typical feminist advice, but very damaging.
It’s inconsistent with scientific findings of greater male variability. Even without different expectations due to gender roles, men at the tails are going to face a severe gender disparity in women who are equal on that measure. Furthermore, if people are not optimizing along a single variable and if traits are hard to see, the chance of a match at the tail end is quite bad. It pays off a lot to move to the center, especially if other men already do so anyway, because it appeals to women.
Also, I don’t think I’m catastrophizing, but rather, telling it how it is, so people can adapt if they can or recognize their poor odds if they can’t.
@MichaelF
I didn’t claim that the initial poor diagnosis was due to feminism, but that it would be worse if the psychiatrist would be an (extremist) feminist, who believes that men should have a level of scrupulosity/self-hatred, that in actuality makes effective wooing very hard, if not impossible.
@Aapje
We agree on some things, and disagree on others. This is one thing we partially agree on. Rigid gender roles have been a way for societies to successfully get neurotic people together. Neurotic men who rigidly follow gender roles and neurotic women who rigidly follow gender roles may or may not enjoy the partners they end up with, but they end up with them either way.
…or they end up with them if they’re part of structures which facilitate that. Traditionally those have been churches, small communities, and, to a lesser extent, bars. You blame feminists, but I’d suggest that part of the failure of neurotic, emotionally immature people to get together in our generation has been the loss of those structures. We’ve lost spaces where a) people can observe each other over long periods of time and thus feel safer with each other, and where b) there’s social pressure to marry which neurotics would be uncomfortable pushing back against.
I can’t say much about bars, but I know that small communities are disappearing and probably won’t be coming back in the foreseeable future. More interesting – and, unlike small communities, potentially reversible – is the decline in churches. As a mildly neurotic atheist I won’t welcome a church revival, but I won’t be surprised if lots of other neurotics find a way to convince themselves to go back to church. (Or, given the relationship between religiosity and fertility, perhaps more people will end up in church as a simple side effect of being raised there.)
To put it another way: Perhaps both atheists and feminists are responsible for the decline in neurotic people getting it on, that result being mediated by their impact on church attendance and religiosity. You can blame Steinem and Friedan, but you also have to blame Hitchens and Dawkins.
I haven’t heard the feminists I know say that, though perhaps we spend time with different feminists. The ones I know say that whether they’ve wanted to or not, whether they’ve been suited to it or not, they’ve been forced to work hard to develop their emotional intelligence, and they’ve done lots of emotional labour. They say they want to be with a man who’s willing to give up the rigid male gender role which says “men don’t do emotions” and put some effort into developing emotionally. The ones who’ve found a man like that generally say that they’re happy.
I’m sure there are lots of women who disagree with them, perhaps including your own feminist friends.
There’s some research on mating which finds that people tend to match on percentiles rather than absolutes. A man who’s 90th percentile on a male physical attractiveness scale is likely to end up with a woman who’s around the 90th percentile on a female attractiveness scale, even if the woman would be rated much higher than the man if you were to put the scales together. Ditto with wealth: A man who has 90th percentile wealth among men is likely to end up with a woman who has around 90th percentile wealth among women, though in absolute terms the man will be much wealthier. The author suggests that the same is true for kindness.
No word on neuroticism in that study, though I’ll take a gamble and suggest that it’s the same case there. Even if there’s a statistical tail of men who are more neurotic than women at that extreme, they can still match up percentile-wise.
(A tangent which I’d be curious to know whether you agree with: I suspect that the usual measures of neuroticism miss a lot of male neuroticism, because they miss neurotic men who are rigidly performing stoic male gender roles. What do you think of that?)
People who are catastrophizing never think they are. 🙂 I’ve done plenty of catastrophizing myself, including about this issue – some of it fed by people doing what you’re doing, some of it self-generated – so I like to think that I know it when I see it. As always, I could be wrong. 🙂
@Aapje
Are you saying that scrupulosity and self-hatred are the same in this instance, or alternatives which lead to the same end result?
I would suggest that the two are orthogonal. You can be scrupulous and still “effectively woo” a partner. I’d agree, though, that being both scrupulous and self-hating is likely to hurt your chances. If you believe that no woman would ever consent to be with you, and you’re scrupulous about not violating consent, you’ve put yourself in a trap. You will fail to put yourself in situations where consent is a possibility, and even if you accidentally end up in one you won’t see the consent because you don’t believe it can exist.
That’s why I think an important realization for many scrupulous and self-hating men is the variety of men that women are attracted to.
(Another important realization is the bit about matching that I mentioned above. If you don’t put much effort into emotional and personal development, you’ll probably end up with a woman who doesn’t, either.)
Andrew, I think that you and Aapje are using different definitions of the word scrupulosity. Aapje clearly means the mental illness:
https://en.wikipedia.org/wiki/Scrupulosity
You appear to be thinking of “careful”.
Thanks for the clarification, MichaelF. That does change the argument.
On second thought, having read the Wikipedia entry, I’m not sure it changes the argument as much as I thought.
Though it’s not necessarily religious, an obsessive and debilitating focus on fears of violating consent boundaries is at the core of this. I guess what I’m talking about is the benefit of moving from clinical scrupulosity to the informal kind, from obsessive fear to reasonable respect.
@Andrew Klaassen
You seem to be reading more into my comment than what I actually wrote. I am not blaming feminists for the failures of neurotic and/or scrupulous men to attract a partner in general. What I blame them for is that on the whole, they tend to:
– refuse to actually listen to the men who fail due to neuroticism and/or scrupulosity, because this doesn’t fit their theories about toxic masculinity and such, so they just start to assume that the men are lying
– give bad advice based on their bad theories
I think I get it. Men tend to care more about crazy women who ruin their lives than women who try to get attention of a man by being around him all the time, not getting the message that he doesn’t like her and then perhaps getting angry at him for not doing what he’s supposed to do, according to her. So if you have a male-dominated environment where men talk about their grievances, it’s also going to be a bit unfair to women by considering female behavior that is harmful to men much more important (and being more eager to pattern match women to that behavior) than behavior that mostly hurts the woman herself. They are also going to care less about male behavior that harms women than the average woman.
As a grievance movement for women, feminism would be fine, if unhealthy for people who stick with it too long. However, it goes a lot further than that, with claim of scientific validity (and the manipulation/suppression of science when it doesn’t cooperate), the making of laws and policies based on their theories, (very effective) attempts to slander those with other theories in the media and not allow them a podium, etc.
Scott Aaronson is a good example of the latter, with him being attacked by various prominent feminists for making a claim about his own experiences that goes against feminist theory in the comment section of his own blog. No prominent feminist came to his aid, not necessarily to agree with what he said, but even just to defend him from slander. Your feminist friends all might be perfectly nice people, yet I’ve heard that so often and when push comes to shove, they let the bad feminists run the show. So what does this make them?
True. And men often want ‘low maintenance’ women who approach men, have similar (instead of higher) expectations of how much household work is needed, are eager to have sex when the guy is horny, are just as active in bed and otherwise do what the man likes best. Why can’t women do the ‘labor’ of learning these thing???
Seriously though. Your feminists friends complain about men not measuring up to one part of the female gender role, which they had to work hard to achieve. However, they fail to realize that it is harder and less rewarding for men to do so, as they have to be stoic as well and don’t get responses that are anywhere as nice for being ’emotionally intelligent’. They are themselves are probably also not measuring up to the male gender role in some ways that many men really would like to see different.
At least, that’s what the evidence strongly suggests, with the women who adopt the male gender role most by earning a lot and thus providing, still demanding a man who provides as well, in contrast to high-earning men. That’s what men who hang around with (or ask) feminists notice, when they rarely if ever approach men. Etc.
Many (neurotic?) men feel that approaching women and/or getting turned down a lot is immensely painful and challenging. Why aren’t women being asked to put some effort into that?
This is good advice for some, who see women as too similar, but bad advice for others, who expect more variety than there actually is. It can even be both, because women are much more varied in some ways than other ways.
If we would have a society where men (and non-feminist women) could actually honestly share their perspectives, rather than get their balls (or labia) cut off, we might get actual progress, instead of things getting worse in important ways with mainstream society being utterly flabbergasted at why.
What the mainstream media and feminists consider reasonable is typically anything but. Did you read ‘Untitled?’ Were those responses reasonable in your eyes?
@Aapje
Thanks for pointing me to the Scott Aaronson kerffufle. Lots of interesting commentary by him, feminists responding to him, and in the comments here and elsewhere. I’m sure there were thousands more words written than what I read, but I did stay up most of the night reading as much as I could.
I’ve seen the same ugly social dynamics among feminists that I’ve seen among pretty much every group of people who are organized around ideas, whether they be economists, atheists, people who write baby-raising books, the religious, archeologists, or Star Wars fans. People who almost toe the orthodoxy line but get some crucial detail wrong are the most strongly condemned. That doesn’t excuse those dynamics, and it doesn’t help people who are hurt by them. However, knowing how common the social dynamics are does help me (callous ol’ me?) look past them to see what interesting and true ideas the group might have. Many of these groups do have at least some interesting and true things to say. (…for approximate values of truth, of course.)
My first reaction to a number of recent feminist ideas was, like Aaronson’s, extremely defensive – how could they attack someone like me, clearly a good guy and unimpeachably committed to equality! – but then I noticed that, huh, they were right about some of my thought patterns and reactions, things I hadn’t paid attention to. Interesting! Some of it was like encountering cognitive-behavioural therapy and noticing negative self-talk for the first time: Things that had always been there but somehow always escaped my attention.
I mentioned economists. They also have a habit of viciously flaming the unorthodox and sometimes bending statistics to their preconceptions, but that doesn’t stop me from reading and learning from them. Some of them have political agendas that are in service of people who want to reduce my power, but that doesn’t stop me from reading and learning from them. I learn, I shape my own conceptions, I compare what they say about the world to what I observe myself. I also expect that if I say that a personal experience of mine disproves or invalidates some orthodox tenent of some economic school, I will (provided anybody notices) get flamed and pilloried for it. Sometimes they’ll be right to flame me, and I’ll learn something from them. I don’t reject interesting ideas from economics just because some of its proponents are assholes, and I don’t do the same with feminist ideas, either.
Speaking of feminist ideas, this comment had some of the most interesting that I encountered in the whole Scott Aaronson discussion. That might be my bias as a parent for parenting experience and analogies showing through, though. This one had a really interesting idea, too.
I’m glad to see that Aaronson learned some of the things that I also learned and have been babbling about, about developing your social and emotional skills and giving up some of your obsessive fears and scrupulosity. He seems to have learned them even better than I did, and started from a much more socially crippled place. It was interesting to read him talk about realizing that there had been women flashing signs of interest at him the whole time which he couldn’t see because he didn’t realize that was a possibility. Thanks again for pointing me in the direction of that discussion!
If this reply is incoherent… the sun is coming up, and I haven’t slept.
Oh, one more thing… the feminist spaces that I’m in, at least, have either a) gotten much friendlier to men discussing male pain with each other than the Aaronson discussion from 2015, or b) the men in them have gotten much better at not stepping on feminist landmines. Either way, I find them a friendlier space in which to discuss male emotional and social experience with other men than the predominantly male spaces I’m in.
Andrew, Amy’s comment struck me as showing that she understood virtually nothing about scrupulosity/ harm OCD- and the fact that you liked it shows me that you don’t either. Firstly, women being afraid of hurting their children are one of the most common manifestations of scrupulosity/ harm OCD. But also, Amy says that when in doubt, she asked a cop. That works for her, but for a person with true scrupulosity/ Harm OCD, that’s reassurance seeking, which just makes things worse. Amy’s comment was basically “Why can’t these people just snap out of it?”
@MichaelF
Apologies if I came across as saying “just snap out of it”. For me, learning to deal even with a comparatively minor variation of this took years of dead ends, depression, and flailing around. From what I gathered (and apologies again if I’m wrong), Amy doesn’t seem to have experienced any of this particular challenge (though she faced plenty of other challenges). However, I thought she did a very good job of describing the skills and perspective I eventually flailed my way to when she described a) how you navigate the unclear and shifting line between “appropriately discipline your child” and “have your child taken away by the government”, and b) how a telling part of your attitude is whether your fears are focused on “what if I slip up and bad things happen to me?” vs. “what if I hurt someone else?” I’m intimately familiar with both (a) and (b), and I think they’re great analogies to the parts of romantic relationships that can be deeply scary for some of us.
She did a great (if unintentional?) riff on Solzhenitsyn, seeing that the line between good and evil runs through her own heart, as it runs through all our hearts. I found that much more realistic than Aaronson’s take that someone could be so shy and introverted that they’d be congenitally incapable of sexual assault. (In all situations?) From my experience, how much of my heart is filled with “what if I slip up and bad things happen to me?” vs. “what if I hurt someone else?” is a decent indicator of where that line is lying at a given time. I’ve noticed that it’s a decent indicator in other people, too.
@Andrew Klaassen
My experience is that feminists have a very high amount of bias though, even if you go to their most valued papers and books.
So you have to be extremely critical of the many fallacies that are common, like god of the gaps reasoning, applying certain reasoning to merely one gender, the exaggeration of gender differences (ironically enough very common), using extremely poor evidence (even mind-reading and novels), etc, etc.
Withstanding this bombardment of fallacies and bad evidence is very difficult and requires very high skills & the acquisition of knowledge from other sources.
—
Just to expand on what MichaelF said: normal human beings try to calibrate their behavior to the norms of other people to quite a large extent.
However, an issue is that the messages that other people send can be hard to interpret, for many reasons, for example:
– messages often have implicit assumptions
– messages are often targeted at problematic people, not non-problematic people
– messages are often direction pushing (be more X), instead of telling people how to behave
– how hard people shout is often not well-correlated to how serious the message should be taken
– people are often selfish in their messaging
– some messages are at least partially designed to increase the status of the sender and may involve a purity spiral
As with all communication problems, errors can happen at both ends & quite often when miscommunication happens, you can blame both sides. Is autistic Jack to blame for not understanding how subtle Mary communicates or is Mary to blame for being very subtle? Should Jack recognize that Mary is a person who communicates subtly or should Mary recognize that Jack is autistic?
Is Amy to blame for believing that a message is intended for her, that wasn’t, or is Bob to blame for not making it clear that the message is not intended for Amy?
There is no clear answer here. However, what should be clear is that messages with more ‘traps’ will cause more problems in receivers. So it seems perfectly fair and a good thing for people like Aaronson to warn those who send messages that these messages can be misinterpreted and how they can be. This doesn’t even necessarily have to result in changed messaging for this to reduce communication problems. Merely the notification itself can make it clear to some receivers that they’ve been interpreting messages wrong.
Anyway, what happened here, is that the message by Aaronson was misinterpreted as an attack on the feminist demand for better behavior by men, rather than on the way the message was presented.
Of course, ultimately we live in a very immature society where the understanding of human communication and coordination by most people is very poor.
@Aapje
My experience is that bias always colours studies of human behaviour, even when the researchers assure you that they have no bias at all and are just looking for the facts. It’s useful to get multiple perspectives to help see what those biases are and develop your own judgment.
(My bias about people who say “I have no bias” is that they usually mean “I think the ways things are is normal and natural and uncoerced and I don’t want to examine my biases, so the study I’m about to do will produce results which comfort the comfortable.”)
So I’ll read a standard work in economics which presents most of the free market order as natural and fair, but then I’ll read some Marx on primitive accumulation or some libertarians on government support for corporate inefficiency. Not all feminist critiques of science will be useful, but a careful picking apart of sex difference science like Brain Storm is worth spending some time on. You might not reject innate sex differences when you’re done (the author doesn’t, either), but you also won’t find yourself surprised if some of the verities of the field end up going the way of 5-HTTLPR or nasal oxytocin or ovulation research results. (Most interesting part of Brain Storm for me: How is it that some measures of masculinity and femininity were reversed over time in studies of gender, but the studies kept finding that men were more masculine and women were more feminine on those measures? The reasons are the usual ones for human behaviour research: Data mining, p-hacking, selective publication, failure to consider alternate explanations.)
Feminists have also had a useful impact on broadening the scope of the questions asked by science. A lot of early scientific research on sexual evolution was guided by Victorian assumptions: Aggressive males and passive females; fighting fathers and loving mothers. As a result, there were some things that scientists failed to notice about motherly love and sisterly kindness until feminist scientists insisted on testing those unexamined assumptions.
One thing I’ve learned from digging up multiple perspectives, including feminist perspectives, is that scientists who wade into controversial subjects are often not basing their opinions on well-supported facts so much as on their hunches about which theories will be supported by future facts. There’s a great discussion of this in The Golem. This is true even in the hard sciences. Scientific history doesn’t reward the third guy whose study proves that General Relativity is true via solid, carefully conducted research with unambiguous results. It rewards the first guy, even if his data analysis is controversial. (It rewards the guy who came up with General Relativity before there was any evidence for it even more.) As much as science is supposed to be about data (and in the end it usually is), a lot of exploratory science is about hunches. Virtually all of our science about human behaviour is currently at the exploratory stage, and probably will be for a long time, but we act like it isn’t.
Even if one’s hunch is that science done or inspired by feminists will turn out to be wrong, it’s good to understand which assumptions they’re challenging. It’s good to be reminded that the standard theories on things like sex differences are running on hunches, and to know some of the reasons that parts of them might turn out to be wrong.
I’ve got more to say about the other kinds of evidence that feminists use and areas outside of science, but I’ll let it percolate for a bit.
@Andrew Klaassen- no, you still don’t understand. True scrupulosity doesn’t just mean excessive fears about moral issues. it’s a collection of symptoms. It means, for example, that if you ask someone to make sure something is safe needlessly, and they tell you it’s OK, your scrupulosity will get WORSE. That’s called reassurance seeking.
As I understand it, you were never diagnosed with scrupulosity and never heard of it until a few days ago. Nor have you spent years studying it. If you got better by trying to be less selfish, or something like that, you almost certainly didn’t have scrupulosity. And yet you (and Amy) seek to lecture people who actually do have it on what will work. That’s what I meant by “just snap out of it”. Often, someone who doesn’t have an actual mental illness (or has a DIFFERENT mental illness) thinks the symptoms are similar to problems in their lives and that people with actual mental illnesses can get over it the same way. It doesn’t work that way.
Getting back to your comment on Amy’s comment- she wrote that maybe guys with fears like Scott’s are really worried about facing consequences for misbehavior. She wrote that mothers don’t become afraid that they might shake the baby and kill it when in reality mothers with scrupulosity/ OCD worry about killing their babies either intentionally or accidentally all the time. She wrote that men with scrupulosity who are afraid of hurting women don’t see them as people- but does that mean mothers with scrupulosity who are afraid of hurting their babies don’t see them as people? To clarify- yes, people with scrupulosity/ harm OCD often say “I’m going to hell” or “I’m going to jail” or “my husband will leave me” if they think they’ve done something wrong but they also experience intense guilt. In fact, scrupulosity/ harm OCD is associated with fear of guilt. It’s what one psychiatrist called a double barreled threat. And no, you can’t get over it by realizing you’re being selfish or whatever. In fact, the stereotype that people with scrupulosity/ harm OCD are just afraid of being punished is a way society stigmatizes people with scrupulosity.
And finally, you couldn’t understand why Scott insisted that “shy nerdy men”-meaning men like him who are afraid of committing rape/ sexual harassment- weren’t capable of committing rape. People with scrupulosity say stuff like that because they’re often accused of wanting to do what they’re afraid of. In fact, people with scrupulosity/ harm OCD often sanitize their symptoms when talking to a psychiatrist so the psychiatrist doesn’t think they’re a danger.
TL:DR- you know nothing about scrupulosity. You liked a harmful comment because it flattered your ideology.
There are treatments for scrupulosity/ harm OCD- but there’s a reason why people with those conditions don’t want to talk about those treatments in public. Acting like there’s an easy way out trivializes what these people- some as young as 12- have to go through.
@MichaelF – Thanks for explaining more of this to me. I meant to be empathetic rather than prescriptive, but I’ve obviously still got some work to do on my social intelligence. 🙂 To put that part of it more plainly: It took me – with no diagnosed mental illness and fears much milder than* those you’ve described for scrupulosity – many years to get (some/most) of my fears around trying to start a romantic relationship sorted out, so I can see how it would take a long time and involve a lot of pain and work for someone with scrupulosity. I would not prescribe any easy fixes. 🙂
I liked Amy’s comment because it reflected things that I had learned via my own years of flailing about. From your comment, it sounds like it doesn’t reflect the sorts of things that someone with scrupulosity would need to learn. I apologize for interjecting it into a discussion that it didn’t apply to.
If you don’t mind my asking, what does someone with scrupulosity have to learn? After the years of struggle and work and help that it takes to make progress and be comfortable with normal-ish romance, what moral and emotional and social lessons does one have for oneself?
I can’t speak to scrupulosity, but I can, from my own experience, say that this is true for some parents who are obsessively focused on what people will think of them as parents and on their own overwhelming feelings of guilt. I’m sure that there’s still some recognition of the baby as a person, but it is only seen through a very thick fog of self-focus. They may be able to say “of course I recognize my baby as a person!”, but their actions do not reflect that. Again, this is not about scrupulosity, but it is about being completely focused on one’s own pain in a way that blinds one to the needs and experiences and individuality of others. (It’s also not about ideology, as it’s something people do no matter their ideology.)
It’s also not completely ridiculous. If you break your leg or get cancer, of course you’re going to be selfish and self-focused for a while. It hurts! You need to heal! You are not going to be the best parent (or partner) for a while, no matter how much you’d like to be!**
*though not completely different from
** Analogies between physical pain and emotional/mental pain aren’t perfect, but I sometimes find them useful.
@MichaelF
That’s interesting. Something that’s necessary to say in one situation (“No, my dear therapist, I *don’t* want to rape people!”) becomes counterproductive in another (“He says that thousands of people he doesn’t know could definitely not rape anyone? Highly improbable.”)
@MichaelF
Apologies for the serial replies, but your comment has prompted lots of self-reflection. I did not get better (at least the first part of getting better) by trying to be less selfish; in many ways, it was the opposite of that. I learned that in some cases it was okay to impose on people a bit; in some cases it was okay to express what I wanted; in some cases it was okay to not be afraid of offending; and in all cases it was okay to think my thoughts and not feel guilty for them. Those aren’t the only things I had to learn (there was some shame stuff going on in addition to guilt stuff), but those seem like the parts that overlap somewhat with what I’ve been learning about scrupulosity. Apologies again – and glad for a correction – if my meager knowledge of scrupulosity is again incorrect.
There was a second stage, though. It took years to get over fears of hurting people or offending them or crossing ambiguous lines that would bring disaster. A number of years after those years (yes, I am middle-aged), I’ve looked back and seen how much those fears made me focus on myself and my pain and not see women as fully individual. When I was finally able to overcome the hurdles to starting a relationship, those fears weren’t fully resolved and caused a whole new set of problems. (What do you do when you have to end a relationship but are consumed by guilt at the thought?) Looking back now, I’m seeing that there was still a whole lot that was concern for myself and my own feelings of guilt disguised as concern for them. I very much thought that I was concerned with their pain, but I was often more concerned with a caricature of their pain that was a reflection of mine.
So there’s a weird double thing going on with selfishness here. First I had to get more selfish in one way, then I had to get less selfish in a different way. First I had to learn to be selfish enough to say, “This is what I want,” and then I had to learn to be unselfish enough to say, “And what do you want?” without leaping to conclusions about what the answer was obviously* going to be.
I’m not sure if any of that makes sense, since it’s the first time I’ve tried to write it out.
*sarcasm
Conferences in my field (financial trading), at least here in the Midwest, tend to be two-day long cocktail parties and golf outings with a market outlook speech or two. Pretty much… exactly what anyone would expect.
Bankers are really, really boring.
@Andrew Klaassen- regarding what’s helpful for scrupulosity, is there some way I could get your email? I’d rather not discuss it here for reasons that will become obvious once you find out.
@MichaelF
Sure.
@Andrew Klaassen- Thanks. And I’m sorry if I was a little rude earlier. It gets frustrating to have to explain this over and over again.
@Andrew Klaassen
Feminists actually are not the ones typically questioning the aggressiveness of men, resulting in one frustrated scientist writing this.
PS. Note that if you reply via the link in the mails, your comments will end up out of order.
@Aapje
The question of evidence is a really interesting one. I was re-watching some clips from the movie Office Space a few days ago. It does not depict real events. It is fake. You could even say that it is full of lies, as early reactions to novels in some communities had it.
And yet… it captures some truths that would be extremely difficult to express quantitatively or measure in a scientific study. You would probably get chuckles of recognition from a low-level temple functionary in ancient Sumeria with a decent translation of the movie. (“If you could just go ahead and make another copy of all these clay tablets, that’d be greeeaaat.”) Even though nothing in it is true, there are still truths in it – about petty power, boredom, small rebellions – if that makes sense somehow? In the end, the “lies” in Office Space are truer than the scientific research on 5-HTTLPR that we had to throw away recently.
There’s a lot more going on with fiction than just that, and it’s all worth exploring. Sometimes fiction is about amplifying distortions of reality, and that’s worth studying. Sometimes fiction is about writing stories of the weak and unimportant that don’t make history, where it wouldn’t be fair to the privacy of the participants to use real facts about them, and that’s worth studying. If some piece of fiction is popular or acclaimed, it tells you something about human nature, and it’s worth applying a theoretical lens or two to that to see what you come up with.
Whatever you come up with after applying various lenses will be weakly supported statements about human nature, but that’s currently true of most of the science that’s done on human nature, too.
Agreed. This is true of every politicized question, and I’d suggest that learning to read novels in various critical ways adds another tool to your evidence toolkit. As you say, don’t limit your knowledge acquisition to just one source.
@Aapje
Depends on which feminists you’re talking to, and the context of the conversation. 🙂
It’s funny… in my (thankfully extremely limited) personal experience with partner violence, Straus’ analysis matches my domestic experience while feminist analysis matches my interactions with organs of the state. Two situations, two useful perspectives.
I’ll push back on one thing from the Straus paper: Straus talks about how easy it is for simplified, distorted narratives to take hold, but he doesn’t want to recognize the salience of that with regard to his own headline findings. I think that, given how recent and fragile feminist gains of nominal equality are, feminists are being reasonable to fear that his nuanced take (which includes the fact that men cause more physical harm to women at the extremes of violence) will be reduced to “women are just as violent as men, so why should we worry about gender differences?” by the time it gets digested as popular culture and translated into politics.
I’m just starting a read of this feminist response to Straus, which you might find interesting if you haven’t read it already, as the author says, “It is difficult to argue with Straus because we often agree with him. In particular, we do not dispute that more than 100 empirical studies using the research instrument called the Conflict Tactics Scale (CTS) consistently support the conclusions that women use as much violence as do men.”
Thanks for the note on this. I was wondering what was going on!
@MichaelF
My stumbling into a topic that I didn’t know much about was rude, too. Ironically, it’s mostly feminists who have tried to teach me this, but I obviously wasn’t paying very good attention…
@Andrew Klaasen
When you build your social analysis, on fiction by an author who wanted to make the same point that you do, do you realy find useful facts about real people, or are you part of a semi-academic mutual admiration society?
@DarkTigger
That depends on whether you, the author, and the mutual admiration society have discovered something true and useful about human interaction, doesn’t it? 🙂
(How can you know whether it’s true? If it’s an accurate reflection of something you’ve experienced, some power dynamic you’ve been in, you can at least say that it’s not false. How can you convince others that it’s true? How can you discover whether it’s a universal truth? Those are both much harder questions, and they’re often where outside critics are too dismissive and inside advocates are too enthusiastic.)
@Aapje
It just occurred to me (which means that the idea is probably not original to me) that your point about greater male variability could contribute to the finding of Straus and others that mild violence is roughly equal between the sexes while extreme violence (especially extreme post-relationship violence… interesting…) is dominated by men.
This also gets me thinking about statistical tails and who they matter to. If something raises your chance of getting into a serious accident from .001% to .002%, you probably won’t care at all – but the hospital, which sees a doubling in the number of serious auto injuries it has to treat, will care a lot. I expect that it’s the same with the people who have to deal with the extremes of partner violence.
DavidFriedman, I see you raised the same example I was thinking of above — about religious differences between therapist and patient.
This statement — “the psychiatrist is legally required to pretend to share the patient’s beliefs” — is not true based on any training or experience I’ve had. If you were in therapy somewhere along the line and you formed this impression from that experience, that sounds like an awful and unprofessional experience of therapy and I’m sorry you had it. If this impression comes from something that you’ve read here, I want to say really clearly that there is no sense in which our job is to pretend to share the patient’s beliefs and there is no legal or ethical requirement to do so.
We are not legally required to share anyone’s beliefs. We are required to competently treat a wide range of people for the mental distress they present with. It’s not my job to decide that a person’s religion is making them depressed and to convert them to something I like better. It’s not my job to say “Oh, you’re a Catholic; yes, I am too and I believe everything you do.” In fact, this would be considered pretty unskillful, bordering on unethical. My Catholicism or lack thereof is not relevant to your Catholicism. My job is to understand what your Catholicism means to you if it seems relevant to the distress you’re communicating, not to share my attitudes about Catholicism with you.
If you are worried about the current state of psychiatry, ask your doctor about Forgetitall, available under most insurance plans. Side effects include sudden onset of cost disease, institutional collapse, failure to replicate, and a sudden desire to worship Moloch in a small portion of patients. See our ad in everywhere for more details.
If they’re all so woke why it is so hard to find a psychiatrist in fucking Berkeley who will use the right fucking pronouns? Every single one of those transgender panels needs to be replaced with a single panel where a person says in a calm and patient voice that if a patient identifies as a man, then you use “he”, and if a patient identifies as a woman, then you use “she.” I think after about seven or eight hours of that perhaps any psychiatrists other than Scott will be able to grasp the concept. (I’m not going to get into nonbinary identities. That is a subject understood by the average layperson within about two minutes, and is therefore apparently too complicated for psychiatrists.)
Every psychiatrist I know in my practice is pretty trans-friendly, feel free to email me if you want more specific recommendations.
Right now I am particularly annoyed at the mental health care system because I am trying to extract permission to donate a kidney, which involves a lot of grinning and pretending to be Neurotypical Karen while a person calls me ‘she’ and then asks about how the bottom surgery I’m not going to get will affect my sex life with my husband. (It is unclear to me what relationship this has to kidney donation.) So my ability to seek new psychological care is somewhat limited.
If I decide to brave the mental health system again I will ask.
Apologies if this is a stupid question, but how is a psychiatrist in a situation where they refer to their own patient in the 3rd person while they’re in the room?
He makes a good point.
😛
Or she.
Statistically less likely, but they could be.
In this context, I think that a specific choice was needed to make the point.
Correct!
Everyone wave hello to the thought police!
Greenwoodjw banned for three months, despite the irony
alternatively, use they and cut down on syllables
This is actually a pretty common English construction– for example, if a person is describing what someone else might think about you.
Yet in your answer, this is achieved with the word “you.”
But I admittedly don’t know what I’m talking about, so ignore me.
“Well, maybe when you tell Steve you don’t want to hang out with him, Steve thinks ‘she’s just tired'”
You could say “Steve thinks you’re just tired” instead, but that conveys slightly different meaning. The above phrase is more stepping into the mind of Steve.
@moonfirestorm
It seems way more straightforward to phrase that as: “Well, maybe when you tell Steve you don’t want to hang out with him, Steve thinks that you are just tired”
It seems to me that there are two likely possibilities:
– psychiatrists have been taught to phrase things this way, perhaps to attempt to force patients to see things from the perspective of the other, so they use the third person exceptionally often
– they don’t do this very often, but Ozy is extremely sensitive to any such misgendering
Both of these seem fairly plausible to me.
Aapje, this way of talking that moonfirestorm describes is common in clinical training programs, so your first possibility is exactly right. It comes across as odd when a person first starts one of these programs and by the end, it comes as second nature. There are a number of intentional communication techniques that happen inside of therapy that don’t happen in other contexts and this is one of them, and it coincidentally raises the frequency of using the client’s third person pronoun.
@cuke
Is there any scientific evidence that this speech pattern works for the intended purpose or is this just supposition?
@Aapje
I’m confused that you’re taking such a strong position against this. It really doesn’t seem much of a stretch to me that you might refer to someone in the third person when discussing these sorts of hypotheticals, or that these sorts of hypotheticals would come up in a therapy session (or any other context where you’re talking about the thoughts of others).
Also, there are other contexts in medicine where you might be referred to in the third person, such as referral letters. I know at least two trans people who have been given referral letters for other doctors (or copies thereof) which misgendered them.
@Heterosteus
I’m confused by your comment, since I didn’t take a particularly strong position, IMO.
My first comment in this specific subthread merely pointed out that the rebuttal by Ozy didn’t actually use the third person singular.
My second comment noted that this seems like an odd thing to say, but I immediately accepted the possibility that psychiatrists have peculiar speech patterns.
My third comment asked whether this apparent habit has a scientifically validated therapeutic purpose.
From my perspective, I was being inquisitive and critical, asking for clarifications, which is not the same as taking a stance and defending it.
Repeated engagement can come off as having a strong opinion in online communications, even if it is just curiosity.
For what it’s worth, I read Aapje here as pursuing a curiosity, which seems like a perfectly fine thing to do in this space. People come on here and snipe and are gratuitously nasty and that’s not what this is, and I appreciate it.
As to this question:
I don’t know.
We do have pretty solid research showing that building a strong working relationship with a patient in which they feel that we understand their point of view really well is strongly correlated with better outcomes.
There’s a huuuuuge amount of specific technique-y stuff in the field of psychotherapy ranging from the fairly reasonable/logical to the bizarre. It’s not unlike in some ways the marketing frenzy over drugs that are very similar. Some therapists build whole careers on trademarking their particular approach, and because words are what we have to work with, it can be very focused on which words, when, and how.
There is research that investigates ways of interacting in sessions that seem to build this strong working relationship and ways that interfere with it, but I couldn’t summarize that research here. There is also research showing that no one technique is overall more effective than another technique, broadly speaking, as long as we’re not doing things to undermine the working relationship.
I could see where *maybe* saying, “Maybe Steve thinks you’re just tired,” could make a patient think, “Why would you say that? Do I look tired? Do I seem tired right now?” and *maybe* saying, “Maybe Steve thinks, ‘he’s just tired’,” comes across more as the therapist taking on the persona of Steve to make the “tired” comment.
Thank you. It seems like a fringe concern when you speak a language in which almost every sentence is gendered, but I understand why it would become a big deal in English. I could tell similar stories, by the way. You’d think gender therapists of all people should know not to misgender their patients -and you’d be wrong. Can’t say I received bad care, but it’s grating.
Incidentally, I really hope concerns about pronouns will finally lead to the well-deserved demise of nurses referring to patients as “we”!
Except MPD patients?
Psychiatrist: “I need to see you again in two weeks”
[turns to nurse]
Psychiatrist: “Please tell Susan to find a time on Thursday for [HIM/HER] if possible.”
The trick is to imagine more than two people existing in the world at the same time.
Gender detection is mostly a system 1, unconscious process: if you look and sound like a woman, people will intuitively think of you as a woman. For most people it will take cognitive effort (system 2) not to call you “she”, which means that they’ll slip whenever their attention is focused on something else.
System 1 is trained by trial and error, so people who are accustomed to you may have internalized calling you “notshe” or whatever pronoun you like, but you can’t expect this from unfamiliar strangers.
If I am paying someone $150/hour to help with my mental health conditions I certainly do expect that they will not actively take actions to make my mental health worse. If they are concerned about their ability to provide this service they are welcome to, for example, stop taking referrals for transgender clients.
Couldn’t there be serious professional consequences for a doctor who stopped taking transgender referrals?
Reasonably confident it’s a “Career Self-Destruct” button.
stop taking referrals for transgender clients.
Wouldn’t that be illegal at least in some places to refuse treatment because of gender identity? And I imagine it would be a pretty solid ground for termination from whatever employment one has, unless one is self-employed.
I’m a mental healthcare provider. Ozy definitely gets to expect healthcare providers to use correct pronouns with their patients. Doctors and therapists aren’t strangers, but licensed professionals whose licenses require them to uphold certain ethical standards. In the U.S. anyway, professional ethical codes in healthcare require providers to have basic cross-cultural competencies that would include proper pronoun usage, among many other things.
Also, declining to take transgender referrals would be of dubious ethical acceptability — there’s been some litigation around this and the providers refusing care have lost. We have a duty to treat and to be competent to treat people from a wide range of backgrounds. Now, if a patient is looking for someone who specializes in transgender issues because that’s why the person is seeking help, a clinician can say they don’t have that specialty and refer them to someone who does. But we aren’t allowed to just refuse to provide healthcare services to transgender or any other kind of person just because of who they are.
I understand why that would make sense for something like an emergency medicine doctor, for which there are few other options, but I would much rather a psychiatrist who has a problem with treating trans people refer me to someone else.
Yeah, I hear you about that. I still think it’s a good thing that the expectation for mental health professionals is that they don’t get to opt out of situations that may be challenging for them for one reason or another.
And while we’re not ER doctors, most mental health professionals deal with people in crisis on a regular basis and we don’t always get to know ahead of time the particulars of any given patient before they are in a crisis; we still need to be able to treat people ethically, and that includes using correct pronouns.
My daughter actually did some original research for her undergrad involving the availability of psychiatric care that addressed the needs of people who are trans. IIRC the upshot was that generally trans patients felt that there specific needs were not being met by the profession. Basically just a set of survey questions that was directed to those who self-identify as trans.
Admittedly the paper had a W.E.I.R.D. issue, and in addition drew heavily from undergrad populations only. But, the underlying research drew upon and extended work that had already been done. If you are trans it’s tough to find good psychological care.
There’s a lot of cases where “I’d rather have somebody who likes me or at least doesn’t hate my guts to provide me a service than somebody who is forced by the government to do so” but that’s not how it actually works, as it seems, at least where the non-discrimination law is concerned.
I think the whole point is that it’s a mistake and not deliberate. That means even if someone is trying not to do it, it can still happen. It could happen to anybody, even the most woke person in the world.
It wasn’t clear to me that Ozy’s whole point is that it was a mistake. My point is that we’re talking about licensed professionals with ethical duties that go well beyond expectations for the general population.
@cuke
Being a professional doesn’t make one superhuman.
My point (trying again) is that Ozy is right to EXPECT a mental healthcare provider to use correct pronouns — indeed, intake forms should ask what pronouns are desired so they can be used correctly.
I am not saying licensed professionals are infallible. I was responding to the reaction that these professionals are just “strangers” like anyone else and cannot be expected to get the pronouns right. That is incorrect, from an ethical/professional/licensing point of view: it is an expectation of the field that they get the pronouns right, just like it’s an expectation of the field that they guard confidentiality, not commit insurance fraud, and a whole host of other expectations.
I would find that a more convincing argument if it wasn’t illegal to provide the service without being licensed.
I have no problem with an organization, public or private, making its stamp of approval conditional on meeting its standards. But the situation described is one where it is illegal to provide psychological services unless you are willing to pretend to attitudes that you may not actually hold.
DavidFriedman, I don’t know if you’re still reading these comments, but you raised a rather important point (to me anyway), so I thought I’d respond.
Our duty is to treat the conditions people come in with and to treat people respectfully in that process. We are not there to have political arguments with people, share our social/political/cultural attitudes with them, or to approve or disapprove of them.
If you’re a therapist who disagrees with divorce and are going to judge couples during couple’s counseling for wanting to get divorced, you’re not going to be able to help them or do your job ethically. Same goes for infidelity.
If you are an atheist and you’re counseling a devout Catholic, you’re not going to help them if you feel like you’re “pretending” by not disagreeing with their belief in the existence of God or their ideas of what’s sinful. My attitude towards God is not relevant when I’m counseling a Catholic person; it’s their attitude towards God that matters.
If a trans person comes in and wants to be treated for anxiety or depression or whatever, what I think about their choice of preferred pronouns is not relevant. I don’t need to “hide” my attitude; it’s that my attitude is not material to the work we’re doing.
If they are coming to me for counseling around gender transition and that’s not something I have expertise with (as opposed to say anxiety or depression or career change or whatever), then I would refer them on. Not because I may or may not disagree with their use of pronouns, but because I lack the expertise to treat what they’re coming in for.
There’s no need to pretend about attitudes because the job isn’t about judging people’s behavior or beliefs or preferences as morally right or wrong based on your attitudes. It’s not to agree or disagree with them about their world views. It’s to help them solve their problems as they’ve defined them.
It’s a given as a therapist that you will work with people all day long who you might otherwise disagree with about any number of things. The therapist’s attitudes are not relevant except as they pertain to things like “what’s your understanding of how anxiety works and what’s your approach to treating it?”
I do reasonably often get new clients who come to me for something like anxiety — but whose life circumstances they feel are unusual and they want to make sure I’m okay to work with them given what they feel are their unusual circumstances. So I’ve had people say to me, “Do you feel you can work with me, because I am….” and then this has been followed by: a homeschooler, polyamorous, Jewish, in a non-traditional gender role marriage, not vaccinating my kids, a heroin user, in an abusive relationship that I can’t leave yet, lying to my wife about affairs, a shoplifter, etc…
My answer to these people — if I think I can otherwise be useful to them for what they’re coming to therapy for — is the same, and is along the lines of “I work with all kinds of different people in all kinds of different situations. My job is to help you suffer less in your life and to meet the goals you set for yourself to do that. It’s not my job to sit in judgment of you.”
This is mind-boggling. How come even the average educated person isn’t that mad. Obviously, pharma companies are unpopular. But the ‘medical establishment’ seems like it is at fault here too. Shouldn’t it be considered ridiculous to plaster the main psychiatry convention in drug ads? Maybe it is too hard to pin down where ‘individual doctors who are not really at fault’ ends and the ‘establishment’ starts. Maybe the public just puts all the blame on the drug companies and little to none on the APA.
Out of the tens of thousands of attendees the few who organize these events are going to be of that manner of conviction.
Maybe they could at least have a few sessions encouraging doctors to look into cheaper alternatives before prescribing the expensive new drugs?
All those ads pay for a lot of the costs of the convention. Such a workshop might …
require the convention organizers to get ad funding from manufacturers of generics?
What, you think they would stop buying ads just because they didn’t like the panel topic?
I’m a financial advisor, and used to get a free copy of the Canadian financial advisor newspaper when I was client-facing. As one would expect, it’s free because it has a lot of ads. All of the ads are super-targeted – about half of them are for various mutual funds (advertising historical rates of return, nifty investment strategies, etc.), and about half are for financial advisor jobs.
It never made me mad at all. Obviously companies that make these products want me to know about the advantages of those products. Thing is, I want to know about them too. Obviously, nothing ever lives up to the hype, and as a professional it’s my job to think about the drawbacks and pick what’s right for the client. But knowing my options is an essential part of that process. In the 5+ years I’ve been doing this, many of the best education sessions I’ve been to have been hosted by insurance companies – and I don’t mean “Here’s what Performax Gold whole life insurance can do!”, I mean tax planning strategies and the like. Because giving us real knowledge that makes us credible with clients is helpful to us, helpful to the clients, and helpful to the companies that sell the products which can be used in the strategies they discuss.
I know that they’re doing it because the companies think they can make money from the sales reps. But that’s only a problem if I’m pushing crap, and I never was. Education about decent products is a useful thing. We always stayed skeptical – there were enough “Is that it?” and “I’d rather just ignore that and use [totally unrelated product] instead” moments to make me think we weren’t all star-struck product pushing monkeys. But ads convey information, and I like information. Why would I be offended at that?
I don’t know about offense, but in personal finance, aren’t a few low-expense-ratio index funds and a budget enough for most people?
Yes, and diet and exercise is enough to keep most people in optimal health.
Yet here we are…
When I was a financial advisor, we were constantly being visited by wholesalers trying to push their products on us, and of course, they weren’t all bad. I was always happy to confer with the guys from BlackRock, Vanguard, State Street and Allianz, who all offered good products with low fees, great advice and easy to understand strategies. Others came by, and I’d take one look at their expense ratios and see their propaganda to the trash can. I only made my wrap fee – there was no incentive to push high fee product from third-party firms.
But I was thinking about how similar the situation that Scott describes is; the relationship between pharma salesmen and doctors is remarkably similar to that of wholesalers and financial advisors, and the ethical problems that arise similar as well – and if there’s no hope for physicians, I wonder what hope there is for financial services…
I imagine it would be much easier to sift through all the crap products as a financial advisor, at least compared to being a doctor. It’s not like Fidelity Large Cap Growth doesn’t work for a customer, but Vanguard Large Cap Growth does. Scott talks about how you often have to try different drugs that, based on what we know, really ought to work the same but just don’t because we just don’t understand the human brain that well.
We plaster everything in ads. We plaster racetracks in ads. We plaster race cars in ads. We plaster race car drivers in ads. Times Square is an internationally famous landmark because it is constantly plastered in ads at all hours of the day. Our society runs on commerce, and so a lot of our communication is taken up by commercials.
Pharmaceutical companies plastering a psychiatric convention with ads does not strike me as a particularly important problem, except if it’s treated as a symptom of runaway capitalism.
As Scott has pointed out in the past, there are two huge mental-health-related APAs: the American Psychiatric Association and the American Psychological Association.
I’m not a member of either group, but I had a partner who belonged to the latter, and attended several of the annual national meetings. My spouse badge entitled me to attend panels, poster sessions, etc.
Drug company propaganda was less pervasive at the psychologists’ event, but other than that, it appears that the two meetings are extraordinarily similar.
Psychologists cannot prescribe drugs in general (as I am sure you are aware). So the lack of ads is not a mystery.
And the American Philosophical Association!
(The relationship may be different.)
Great writeup. I was particularly struck by the photo of the fanapt rep. I hope you went over to say hello, he looks like he’s a bit numb to it all.