
This is an entry to the Adversarial Collaboration Contest by Mark Davis and Mark Webb, who sent the following introduction along with their entry:
Mark Davis is a naturopathic doctor. Naturopathic medicine is a century-old profession in the United States, but it’s small, with fewer than 10,000 NDs licensed to practice naturopathic medicine in the US in 2018. The profession has been historically highly skeptical of vaccination in general, and the modern profession is contentiously split on the topic, with vocal advocates of CDC-scheduled routine childhood vaccination and vocal dissidents both offering continuing medical education for NDs. Mark Davis’ main goal in this adversarial collaboration was to argue that there is enough reasonable doubt that routine childhood vaccines could contribute to hyper-inflammatory disease, and enough reduced harm from vaccine-preventable diseases from other medical and public health interventions (in countries with greater economic resources) that parents should be given wide latitude to make individual choices re: routine childhood vaccines despite the clear benefits to individual and public health from preventing those diseases. He became more convinced in his conversations with Mark Webb that widespread childhood vaccination is in the best interest of public health.
Mark Webb is a clinical researcher – with a current focus in oncology. He completed a PhD in immunology, specifically focused on the mechanisms driving the development of asthma. Mark Webb’s main goal in this collaboration was to argue that atopy and autoimmunity are likely not driven by vaccination, and that this idea is a distraction from finding the real causes of the increase in these diseases. Throughout the collaboration, he was reminded of the nature of safety surveillance with all drugs, and of the sensitive nature of vaccination as a medical intervention. He became persuaded that policy should not just reflect the best evidence currently available, but should also reflect a certain degree of humility that there will always be something we don’t know.
Setting the parameters of the debate
Why are vaccines the target of both intense support on the one side, and intense skepticism on the other? In part, this is because of the nature of how vaccines work. On the side supporting vaccination, there is strong evidence that vaccination changed the face of epidemic disease in the 20th century. Smallpox is effectively extinct, and polio is nearly there. What agent caused this veritable miracle? Vaccines did. Some diseases are harder to create vaccines against, like HIV or herpes, but eventually we can envision a day when vaccine development can – not just cure – but prevent huge numbers of people from ever having to worry about the deadly diseases of the past. Vaccination is clearly a proven tool for promoting public health. It has been successful at eradicating diseases that used to be endemic to various regions; and where diseases haven’t been eradicated vaccination has been very successful at preventing outbreaks and disease spread. What could possibly be bad about vaccination?
Perhaps the biggest reason vaccination has received the degree of skepticism it does is because of how it is administered. Any medical intervention that is targeted toward a high percentage of the population should be scrutinized. Indeed, it would be irresponsible not to undergo continual safety surveillance of a medical intervention that is administered to 90% or more of the population. Vaccines are also administered in multiple doses to one of the most vulnerable population categories: children. There is a strong tradition in clinical research to ensuring high levels of oversight toward children and other vulnerable populations.
Finally, vaccination is a medical intervention intended to produce a permanent effect. It is especially important to be vigilant about therapies whose effects are intended to be persistent. A drug that temporarily relieves asthma symptoms is generally less suspect than one that actually cures asthma. This is because if the expected effects disappear over time, any unknown and unexpected effects are more likely to disappear (although this is not always the case). However, if we’re looking at a treatment with long-lasting effects, unknown long-lasting effects could also appear.
This does not, in itself, mean we shouldn’t implement medical innovations meant to be permanent, targeted toward children, or that would have widespread impact. That would be like suggesting we cease all pediatric cancer research. But it is important to understand why the conversation about vaccine safety is necessarily an ongoing inquiry, not a one-off check of whether “vaccines are safe”. It is also not irrational for a subset of individuals to continue to be wary of possible missed adverse effects, no matter how much research fails to demonstrate any harm.
Before we introduce the parameters of this debate, we wish to emphasize that vaccination is a method of intervention, not one specific intervention. The statement “vaccines are safe” cannot be applied across the board to all vaccines that ever have or ever will be created, any more than you could say, “prescription drugs are safe” for all current and future prescription drugs. This question would hinge more on our confidence in the clinical approval process to ensure drug safety – an interesting question, but one entirely beyond the scope of this essay. In that sense, any general complaint you might make about prescription drug approval or safety could equally apply to any vaccine. In addition, a dozen studies demonstrating the safety of the DTaP vaccine do not demonstrate that MMR is safe. Studies for MMR have to be conducted independently, just as studies about amlodipine do not tell us whether olmesartan is safe.
These, then are the parameters surrounding vaccine safety:
- Vaccination has proven benefits to public health
- Vaccination has all the hallmarks of an intervention with the potential to cause harm
One more consideration should be noted here. In general, the benefits of widespread adoption of routine childhood vaccination in countries with fewer economic resources are clear and not disputed between the collaborators. Nations with little access to medical care are likely to see greater benefits from vaccination than nations with highly accessible medical care infrastructures. For example, an infection that would be lethal in parts of sub-Saharan Africa might be easily treated if contracted in France. Thus, a risk-benefit analysis for economically developed countries will require a more stringent requirement for clear benefit over risk than in the developing world.
From this, we will consider two proposals for economically developed nations such as the US, Europe, Canada, Japan, etc.:
- Mandatory vaccination is necessary to achieve public policy objectives for vaccines.
- Public policy should encourage parents to not vaccinate, or should at least normalize parents’ decisions to avoid vaccination.
Should vaccination be mandatory?
In order to recommend that vaccination, as a matter of public policy, should be mandatory, we would need to show that:
- Vaccination achieves a legitimate public policy objective
- This public policy objective cannot be achieved without making vaccination mandatory
When considering vaccine benefits (and indeed virtually everything about vaccines) it is important not to generalize the best or worst aspects of one vaccine with another vaccine, or a vaccine used in one socio-economic context with a vaccine used in another. The benefits of the smallpox vaccine have been significantly greater than, say, the rotavirus vaccine, and rotavirus vaccine provides more benefits in countries with few healthcare resources. Even so, rotavirus vaccination still conveys positive benefits that should not be ignored; those benefits should simply be put in context, and any potential adverse effects of rotavirus vaccination should be factored in.
Let’s continue with rotavirus for a minute to highlight what we mean. In most people who contract rotavirus, the greatest concern is dehydration. Most deaths from rotavirus currently occur in the third world, not because rotavirus isn’t transmitted in the US, but because among those who do contract rotavirus hydration therapy is highly successful. In other words, if you’re living in a place where you have to hike 3 miles to collect dirty drinking water that made you sick in the first place, you’re going to struggle with this disease. If you live in Germany and have ready access to quality healthcare services no matter where in the country you live, you’re probably going to be fine.
That doesn’t mean the rotavirus vaccine does nothing. Most people who get the vaccine will be spared the debilitating diarrhea and possibly the trip to the ER. So it’s a meaningful intervention, but it’s not really a life-or-death intervention in resource-rich countries. A similar story can be told for some – though not all – of the other vaccines on the US CDC’s recommended schedule. Generally speaking, not contracting the disease produces the positive good of preventing morbidity and other costs to individuals, but it’s mostly not a life-or-death event. This distinction is important, because “has strong benefits” can be weighed against potential downsides. On the other hand, “keeps you from dying” is hard to weigh against even debilitating or disfiguring downsides. This is basically how something like chemotherapy can become a real treatment, instead of a particularly cruel “enhanced interrogation” technique.
If you live in a totalitarian dictatorship, it’s much easier to make something mandatory. You just tell everyone to do it and if they don’t, you line them up against the wall. In a democratic republic, where the perception of the people often shapes public policy, it’s important not to make enemies of the general public. And although this is not a bar against a mandatory policy, it suggests any such policy should be tempered with the aim of ensuring it is strongly justified, is not rigidly unyielding, and therefore does not become burdensome and unpopular. In the US, in most states, mandatory public vaccination tends to meet this bar (with some qualifications).
First, the policy is not rigidly unyielding in most states. Every state in the USA has some form of mandatory vaccination policy in order for children to attend public schools. Since education is mandatory, and public schooling is freely available to all children, this amounts to a strongly coercive opt-out system. Parents who do not wish to vaccinate are forced to pay a price for their dissention by finding some other way to educate their children than through the public education system they cannot opt out of contributing to through taxation.
Some exceptions are allowed, depending on the state you live in. For example, every US state allows exemptions for medical reasons, since, for example, some small percentage of people are allergic to some of the components of vaccines. All but three states allow religious exemptions, for those whose religion prohibits vaccination (CA, MS, and WV only allow medical exemptions, representing less than 15% of the total US population). But if you don’t belong to a religion that prohibits vaccination, you’ll need to live in one of the 18 states that allow exemptions for personal beliefs as well (these include AR, AZ, CO, ID, LA, ME, MI, MN, MO, ND, OH, OK, OR, PA, TX, UT, WA, and WI representing about 35% of the US population) if you want your children to attend public school without getting them vaccinated.
There is, perhaps, a general concern about totalitarian tendencies here. The concern is that, with physicians as gatekeepers of medical care, they are in a particularly coercive position when it comes to individual patient decisions. Say a patient is strongly opposed to some aspect of vaccination, and wants to opt out of the system. When they try to do this, perhaps their doctor refuses to play along, preferring to use their position of authority to compel the parents to following standardized guidelines. This is certainly the case in some situations, but is it the norm? According to a survey of Washington State pediatricians in 2011, a majority reported they are willing to follow an alternative vaccination schedule to the one advocated by the CDC if a parent requests one. Interestingly, 77% of the pediatricians surveyed reported parents sometimes or frequently make these requests. So not only are parents asking pediatricians to follow different guidance than what the CDC recommendations, most pediatricians report that they are willing to comply. As these are statistical results, this means that there are some parents asking to follow a different vaccine schedule who are refused by their pediatrician; but it appears that (at least from what we know of Washington State) these parents need only go looking for a readily-available second opinion and they will find a pediatrician who is willing to go along with the vaccine schedule they prefer.
Despite this, the argument, “vaccination should be mandatory” must contend with one uncomfortable fact: in many European nations vaccination isn’t mandatory, and those nations often achieve higher vaccination rates than in the US. The table below lists different nations’ vaccination rates. In addition to comparing these rates to one another, it is necessary to compare rates to the threshold required for “herd immunity”. One compelling public health argument in favor of vaccination is the potential of a vaccine to stop the spread of a disease because an infected person will be unlikely to spread the infection prior to recovery because everyone they meet is already immune. It’s a little more complicated than this, but fortunately it can be easily simplified into one number that represents the percentage of the population that needs to be vaccinated in order to ensure the disease will slowly die out faster than it can spread. This is represented by the “threshold” row in the table below.
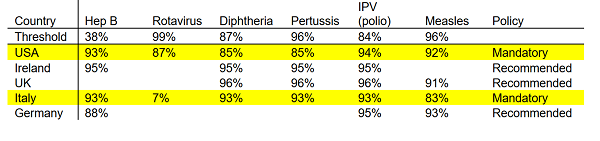
Notice that for hepatitis B less than 40% of the population needs to be vaccinated in order to achieve herd immunity. Hepatitis B is usually the first vaccine babies get, with current recommendations being to give this prior to leaving the hospital. The specifics of why this vaccine is recommended this early are probably beyond our scope, but from the perspective of “intended to stop the spread of the disease” we’re probably more aggressive than we need to be. Meanwhile, for rotavirus nearly everyone has to get the vaccine in order to achieve herd immunity. We’d have to live in a totalitarian dictatorship to get the kind of levels we’d need to eradicate rotavirus through vaccination alone. It’s important here to note that the vaccine does confer protection to an individual who receives it. But since rotavirus is so highly contagious, really high vaccination rates are not enough to stop the spread of the disease. Thus, as a personal healthcare decision the rotavirus vaccine appears highly attractive. However, as a matter of public policy rotavirus vaccination cannot be expected to prevent outbreaks. It might make them a little less severe, or perhaps they’ll spread more slowly, but they’ll still happen.
The important observation from the table above, however, is that nations like Ireland and the UK have much higher vaccination rates than the US without making them mandatory. Often, these rates are much higher. For example, the US rate of vaccination against diphtheria is below what is required to achieve herd immunity, in contrast to diphtheria vaccination rates in Ireland and the UK, which exceed the level required for herd immunity. This is not to say that eliminating mandatory vaccination will increase vaccination rates. Each nation has different, and unique, health care systems, laws, policies, and behavioral norms. This is probably more complicated than “Let’s just copy what the Germans are doing.” But it is not possible to argue, “Without mandatory vaccination we cannot achieve herd immunity; people will be dying of disease in the streets!” Although we should be cautious about sudden, dramatic changes to a system that is largely working, both authors concede that in developed nations such as the US mandatory vaccination is probably not necessary to achieve public health objectives.
Should health authorities normalize parental decisions not to vaccinate?
Any medical intervention comes with some level of risk, both known and unknown. For vaccination, the most common, well-documented, known risk is the potential for an allergic response to some component of the vaccine. The most common allergic component is egg, and people with severe egg allergies are instructed to consult their physician prior to vaccination. How common are allergies to vaccines? A good estimate is about 3 per one million doses. This would be the equivalent of about 200 people in France, or 35 in the US state of Ohio. This is the biggest recognized, known risk of vaccines. But are there significant unrecognized risks of vaccination that could impact the risk/benefit assessment of vaccine safety?
In order to make a general recommendation against vaccination as a matter of public policy, any identified harm would need to outweigh the benefits which those vaccines confer upon their recipients. There are a number of theories about potential harm that could come from vaccines. Much ink has been spilled about vaccines and autism, and it is not our intent to cover that ground again here. Both authors agreed that the evidence does not support a link between vaccines and autism.
There is another, more subtle linkage that we would like to consider here; this is the hypothesis that vaccines might contribute to autoimmune and autoinflammatory diseases such as multiple sclerosis, type I diabetes, inflammatory bowel disease, rheumatoid arthritis, etc., or to atopic diseases such as asthma, eczema, and food allergies. These diseases have been increasing for decades – the same decades during which we have increasingly been administering more vaccines, earlier and earlier in childhood and into infancy. Thus, it is appropriate to consider the possibility of a causal link between these two phenomena: do vaccines lead to autoimmune and allergic disease?
Are kids who are vaccinated more likely to develop these immune system diseases? Despite a large number of studies into this area, the results so far have been mixed. On one hand you could argue, as above, that vaccines lead to increases in immune system diseases. And indeed, you can find researchers who have demonstrated just such a link for DPT, tetanus, MMR, etc.
- DPT (article; article)
- Tetanus specifically
- Tuberculosis (BCG vaccination doesn’t prevent allergic disorders, but positive TB test does)
- Measles (article; article)
Meanwhile, other researchers have hypothesized that vaccination protects against development of allergic disease and autoimmunity. How might this be? There is strong evidence that increased antibiotic use in early childhood is associated with increases in developing immune system diseases; childhood use of antibiotics can shift the balance of commensal bacteria in a way the hygiene hypothesis would predict makes you more susceptible to immune system diseases. So it’s also possible that not vaccinating could lead to increased antibiotics use if your child does get infected with measles, mumps, pertussis, etc. Regardless of whether antibiotics are the mediating factor, some studies indicate certain vaccines having a protective effect against atopy:
- Tuberculosis (meta-analysis)
- Measles (article; article)
- MMR (article)
Finally, some studies find no difference between vaccination and natural infection in development of immune system disease:
- Multiple vaccines (article; article)
- DPT (as a marker for all vaccines)
- Pertussis (We were only able to locate one genuine placebo-controlled RCT of a routine childhood vaccine in which the authors looked for atopy – they found no significant difference in atopy between the placebo and real pertussis vaccine groups at ages two and a half and seven)
This topic has been reviewed multiple times in the scientific literature, and the conclusions have been the same each time: there is no demonstrable impact of vaccines driving immune system diseases. Given these conflicting studies, we can’t say that there is convincing evidence that vaccines either cause increased immune system disease or that they protect against development of these diseases.
One hypothesis for how vaccines might contribute to the rise in atopy and autoimmunity side-steps most of the evidence cited above. These articles look at whether vaccination itself causes allergic disease, but what if the opposite is true – not vaccinating protects against allergic disease?
Hygiene Hypothesis
What causes the development of autoimmune, autoinflammatory, and atopic disease? A full answer to that question – one that could lead to prevention of these diseases – would probably be worth at least a Nobel prize in medicine; which is to say we don’t entirely understand it. However, the current leading explanation in vogue amongst immunologists and epidemiologists who study the recent trend in which we see these diseases increasing dramatically in the developed world is call the hygiene hypothesis.
First proposed about thirty years ago, the hygiene hypothesis is the idea that some of the bacterial and parasitic infections that modern medical technology has eliminated might have been performing an important function in the human immune system – and when you take them away you start seeing problems. For example, if you go back 5,000 years in human history, few people would be completely free of parasitic infections, such as hookworm or whipworm. These parasites might make you mildly ill after you first get infected, but so long as your immune system maintains control of the infestation you may not notice it. There is a constant, low-grade battle between your immune system and the parasite. This battle doesn’t just go on your entire life, but has gone on for generations of humans (and their common ancestors), such that this is the normal state of affairs. Fast forward 5,000 years, and modern water treatment suddenly prevents millions of people from ever experiencing a type of infection that was a constant throughout humanity’s evolution. As a result, the immune system doesn’t know what to target. There has never been a time when there was nothing to fight, so it begins to fight itself, accidentally.
This hypothesis isn’t just high-level theoretical hand-waving. Parasites, such as hookworm, have been shown to induce the same kind of immune mediators that are commonly seen in autoimmune diseases. In fact, some people with diverse autoimmune, allergic and autoinflammatory conditions have started intentionally infecting themselves with hookworm. Based in part on this movement, clinical trials have been conducted, and more are currently under way investigating whether re-introducing parasitic infections such as hookworm can be used to treat Crohn’s and other autoimmune diseases.
If the hygiene hypothesis is correct, and removing certain persistent infections is driving the increase in autoimmunity, autoinflammation, and atopy; does that mean there is a hygiene hypothesis explanation that links vaccination with these diseases?
This hypothesis is much more difficult to test, in the case of vaccination, because it’s not saying the vaccine itself causes allergy and autoimmunity. Instead, it argues that getting rid of diseases such as measles and pertussis causes the increase in allergy and autoimmunity. Thus, it doesn’t really matter whether you get the vaccine or not, what matters is whether you get measles or pertussis or not. If everyone around you gets vaccinated, herd immunity will kick in – the very effect public policy is looking to achieve – and you will never get the chance to catch measles. So no matter how large or well-designed or randomized/controlled, a study that compares US children who are vaccinated with those who aren’t won’t be able to test the hypothesis that endemic measles outbreaks protect against development of allergies and autoimmunity.
The closest we can come to addressing this question are some of the measles studies cited above. One of these compared individuals in Guinea-Bissau who were either naturally exposed to measles or who had been vaccinated; they identified a protective effect for natural measles exposure. Meanwhile, another study in Finland made a similar comparison and found natural measles infection exacerbated atopy and allergic disease. The problem with this approach is that it doesn’t just compare vaccination with not vaccinating – it compares people who don’t vaccinate with those who do. These are not necessarily the same. For example, people with access to vaccines in a nation such as Guinea-Bissau might be of a different socio-economic status than people with no access to vaccines. And socio-economic status has been identified as a factor in development of atopy and autoimmunity.
One way to look at this is to ask whether vaccinated children have different immune system markers, such that they look like they are more susceptible to developing immune system diseases. Researchers at the University of British Columbia looked for exactly this kind of change in a recent study. They took blood from children who had or had not been vaccinated and looked at whether these children’s circulating immune system cells differed from each other. They did not find any of the differences we would expect to find if vaccines caused a general shift in a vaccinated person’s immune system. This study should be taken with a large grain of salt however, as the sample size was smaller than expected, due to the difficulty of recruiting unvaccinated children.
A more targeted way to test this hypothesis would be to randomly assign children to receive one or multiple vaccinations and compare to children who receive no vaccination, then expose all the children to the disease(s) they were vaccinated against and check whether they develop various types of atopic and autoimmune disease. This would have to be done in a nation that currently has endemic levels of the disease in question and/or frequent outbreaks. Also, a nation with no scruples about conducting experiments on children in which you intentionally expose them to infectious agents at an early age.
This does not mean the hypothesis cannot be tested, but it will be a difficult hypothesis to test consistently, and the current state of the evidence suggests a high level of disagreement. In advance of such evidence, we might ask: What are the implications if this hypothesis were confirmed? Would that mean deciding whether to accept – even encourage – endemic disease burdens such as measles, polio, pertussis, etc.? There is no reason to believe that the hygiene hypothesis requires specific bacterial or parasitic infections in order to promote the development of a healthy immune system. It is likely that whole classes of commensal bacteria are protective against the development of atopy and autoimmunity. If there were a group of people, living in a nation that has achieved herd immunity to many of the infectious agents discussed above, and that had rates of allergy and autoimmunity significantly below that of the rest of the population we might study that group to determine whether they are exposed to commensal agents that are protective against atopy and autoimmunity.
Fortunately, the Amish in the US provide an excellent example of just such a case. They experience almost none of the diseases we associate with developed nations. They have far less cancer, asthma, food allergies, MS, etc. You might think, “but that’s because they don’t vaccinate!” except that they do vaccinate. Different communities vary, as each Amish community makes its own rules about what aspects of modern technology to adopt, but one survey of the Amish suggests that about 85% of Amish children are receiving vaccinations. Additional anecdotal evidence suggests this may be a lower bound, but even if we assume 85% of Amish children are getting vaccinated we have to wonder why they see such low rates of modern diseases. Sure, they aren’t at the 90-95% of most of the rest of the country, but it’s hard to see how that extra 5-10% vaccination rate could be leading to such a huge increase in autoimmune diseases – especially without significant numbers of outbreaks running through their communities. Maybe it’s just something about the Amish?
It’s not just something about the Amish. An early observation about the hygiene hypothesis is that people who live on farms have a much lower rate of developing immune system disorders. The belief is that this is because they are more frequently exposed to environmental bacteria and parasites.
A group of researchers identified a different German religious sect, called the Hutterites, which also engages in regular farming. They are closely related to the Amish, and came from similar parts Germany at similar times. However the norms of the Hutterites dictate a much lower interaction between livestock and children/pregnant women (most hygiene hypothesis evidence suggests prenatal, neonatal, up through young childhood exposure is the critical exposure period). This genetically similar group, who had less early-life exposure to the farm environment than the Amish, gets asthma at a rate 5-7 times higher than Amish farmers (Amish asthma rate is 2-3%, Hutterite asthma rate is 15%). The researchers then took dust from the Amish barns and forced mice to breathe it in. They found the dust protected the mice from developing an experimentally-induced allergic response, and that it caused real, measurable changes in the immune systems of these mice, consistent with what we see in humans who are less allergic, and consistent with the differences they saw in the Amish farmers who had low allergic disease compared to the Hutterites.
But not everyone can live on farms (anymore) so current research is also focused at discovering which commensal bacteria humans need to protect against developing immune system diseases. This is similar to the idea of taking the dust from Amish farms, but consistent treatments require us to actually know what elements of the dust actually matter to preventing disease. It’s possible, for example, that modern lifestyles reduce exposure to exposure to mycobacteria. Some promising attempts have been made at reintroduction of killed mycobacteria into atopic individuals. This approach is akin to creating a vaccine against atopic disease, though more recent research has focused on changing the balance of live bacteria instead of simply introducing killed bacteria. This approach attempts to retrain the all-important gut commensal balance through techniques such as fecal microbiota transplantation (poop transplants) or investigating dietary changes that could help push the balance toward protective commensal bacteria and away from sensitizing commensals.
If we create a vaccine that specifically targets the commensal bacteria, or parasites that protect you from developing immune system diseases, we might suspect that vaccine of directly contributing to people who receive it developing those diseases. For example, one such helminth has been the target of recent vaccine development due to the significant harms it causes in the developing world; thus there is a concern on one hand of the persistent symptoms of infection caused by the hookworm infection, and a concern on the other of increasing the risk of allergic infection. In the developing world, where iron deficiency is a major cause of morbidity (large hookworm infections cause iron deficiency as they feed off the blood of hosts), development of an anti-hookworm vaccine could be a significantly beneficial intervention. In economically developed nations these types of infections were mostly eliminated when water treatment eliminated the fecal-oral route many pathogens use to spread from host to host.
Let’s revisit the implications of the hypothesis that the elimination of endemic diseases by vaccines causes an increase in atopy and autoimmunity. Currently, there is not strong evidence that vaccines drive autoimmunity and atopy, although additional research should be done in this area – focusing on disease exposure and not just vaccination status. Even if such a link were to be established in the future, is cessation of vaccination the best approach? Perhaps a better solution to the rise of atopy and autoimmunity is not to actively encourage the return of endemic diseases that are associated with other significant harms, but to encourage exposure to commensal bacteria and parasites that do not come with significant associated morbidity and mortality, such as those that help prevent atopy and autoimmunity in the Amish.
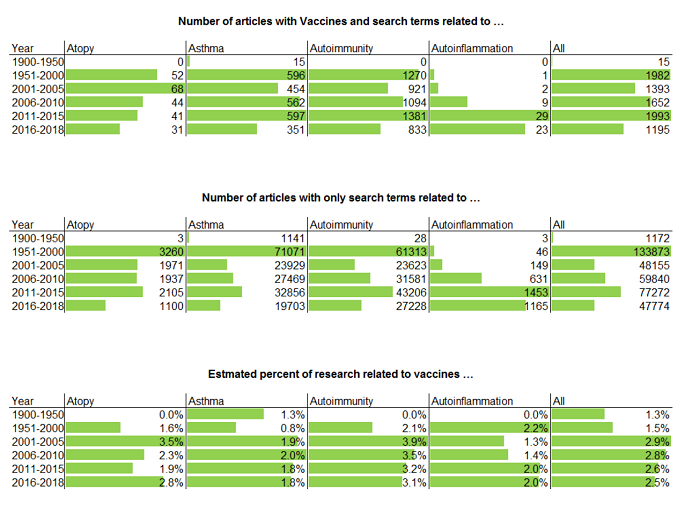
For the vaccines currently recommended today, we haven’t seen convincing evidence of long-lasting or permanent negative side effects. It is important that the medical community continue to monitor vaccines to confirm the relative safety of vaccination, and the evidence of the academic literature is that this is actively happening. Every year, many articles posted to PubMed confirm that ongoing surveillance of vaccine safety is being actively pursued by the scientific research community.
This is appropriate, as we do not ever expect to finally “prove” that vaccines are not harmful. While it is possible to obtain support for a positive declaration such as, “vaccines are effective”, the only way to “prove a negative” with the scientific method is to fail to find support after looking for it. With vaccines, it is important to remember that this is a daunting task. There are many vaccines currently in use, and there are many possible harms to be investigated. In addition, new vaccines are currently being developed, such that we should expect to continue to investigate the safety of various specific vaccines for the foreseeable future.
Conclusions
In the first question, we assessed whether vaccination, as a matter of public policy, should be made mandatory. In essence, this asks whether the benefits to vaccination are sufficiently great that the decision of whether to vaccination should be removed from individual decision-making. Given the sensitive nature of a policy that essentially amounts to dictating private parental medical decisions, we adopted a standard similar to the US Supreme Court’s “strict scrutiny” standard: is it a compelling public health interest, and is it narrowly tailored? This is not generally the standard currently adopted by policy makers today. Mandatory vaccination failed this test, in that it is not narrowly tailored, since herd immunity can be achieved without making vaccination mandatory.
The case of California is an interesting example of how public policy is currently set in regards to vaccination. In 2014, California’s measles vaccination rate was below what is required for herd immunity, and there was a subsequent outbreak of measles at Disneyland. This was a high-profile event. In response, vaccine proponents argued that California’s laws should be strengthened to eliminate the personal and religious exemptions for vaccinations that were then in place. After the law was passed, despite a suspiciously large increase in medical exemptions, vaccination rates rose above the level required to achieve herd immunity, both at the statewide and at the county level. This law also sparked protests from parents who saw the law as removing the rights of parents to make medical decisions for their children. The debate was highly contentious, and continues to be a source of some political animosity.
According to our analysis, future public debates about vaccination do not have to follow this pattern. It is sensible, given the nature of vaccination as a medical intervention, to be skeptical that safety surveillance may have missed something important with respect to vaccines. It is also entirely possible to achieve vaccination rates sufficient to achieve herd immunity without removing medical decision-making ability from parents. A better approach might be to study models such as those of the UK and Germany. In the UK, vaccination is strongly recommended, and vaccines are provided at no cost to the individual. Germany, meanwhile, also strongly recommends vaccination but does not pay for vaccines. A more thorough study of social norms and other factors influencing vaccination rates could provide alternative approaches to the drive for mandatory vaccination, and help alleviate this front of the culture war. This study of alternatives to mandates should be undertaken prior to the next high-profile event, in order to provide policy-makers with a ready alternative that can foment good will between those wary of vaccination and those wary of the potential for outbreaks.
In the second question, we asked whether the public policy toward vaccination should be reversed. It is entirely understandable for concerned parents to adopt a “precautionary principle” approach to vaccination – given the nature of vaccination as a universal medical intervention targeted at babies and young children. However, as a matter of public policy, a general “precautionary principle” approach cannot be recommended in light of the proven harms vaccines protect against. At this time, there is not sufficient evidence that vaccination causes real harms – despite attempts to investigate various mechanisms by which they are theorized to cause harm. This does not mean vaccines cause no harm, but like any medical intervention, we require each vaccine to undergo initial testing for safety and efficacy before regulatory approval, then additional surveillance afterward.
Based on what we currently know, vaccines are an important element of disease control and eradication. Public policy may not require mandatory vaccination, but including recommendations for parents to vaccinate children is a legitimate public policy objective. Vaccine safety and vaccine surveillance are also important and legitimate. Many primary research articles are published each year investigating vaccine risks, and looking for unknown harms.
Ultimately, the question of whether something is “safe” can only ever be either answered:
- “no, we have evidence that it causes significant harm” or
- “we don’t have evidence that it causes significant harm”.
Meanwhile, many of the potential benefits of vaccination are recognized at the level of community adoption – which introduces a coordination problem. Thus, the central conflict we encounter in this area is between individuals who wish to invoke the precautionary principle for themselves and for their families, versus community standards that seek to eliminate a known danger. This conflict (between individual freedom to dissent in order to avoid fat-tailed risk versus a level of community solidarity necessary to combat societal ills) is common to many problems besides vaccination.
We believe this coordination problem may be largely resolved without restricting individual freedom. Individuals who wish to invoke the precautionary principle for themselves and their families should not be penalized for doing so.
















As an anarchist (possibly transitioning back to libertarianism / minarchism) of course my answer is “no”. But I’ll be goddamned if I’ll let your little plague rat come over to my house.
This collaboration was a huge disappointment. There is little or no evidence cited to support the stated conclusion, and in fact, the essay seems to be arguing against itself.
You conclude with “mandates are not necessary to achieve high vaccination rates” despite citing an example (the California case) which shows the opposite. The only evidence ever offered in favor of the conclusion is the higher vaccination rates in Europe, but the essay never addresses confounding factors or seriously argues that the US could magically turn into Germany.
Possibly stupid idea, but I’ll put it out there anyway: Why not implement cap-and-trade for vaccination? Say “we need herd immunity of X%, and population due for this vaccine of Y, so we have X*Y vouchers. The first N are given to those with religious and medical exemptions (with more stringent controls to prevent the issues from CA), and the remaining exemptions (X*Y-N) are randomly distributed to those in the target population (or their guardians).” They can give them away, trade them, sell them, set fire to them, etc.
Of course, there’s all kinds of complication, but this way people can exercise their choice without endangering others, but must also bear a proportional cost of that choice. If there are few anti-vaxxers in a given market, the exemptions would be low-demand, low-cost items reflecting the minimal danger such a small anti-vax population would pose, while in markets with lots of anti-vaxxers, the high demand and thus high cost of vouchers would force them to reckon with the societal costs of their choices, and force them to “put their money where their mouth is” so to speak. Plus, it’s like the lottery – a tax on stupid people.
There’s tons of implementation difficulties (how big are the markets, how to prevent excessive religion & medical exemptions, etc.), but at the least it preserves some aspect of choice while making the cost of that choice proportionate to the externality imposed on others.
This was really, really good, with two caveats: the formatting of the abstract and the headers is needlessly loud, and the end of the essay, as my highschool history teacher once said, falls off a cliff. There should probably be an additional paragraph at the end, or the last one should be expanded a bit.
That said, I think this essay sets the standard for what a “good” project of this sort should look like. It properly identifies two bounds in policy space, clearly states what sort of evidence is needed to support the selection of a policy on either side of those bounds, and then discusses the state of the evidence and the actually-in-use policy in terms of the identified bounds.
I appreciate Mark and Mark explaining their initial viewpoint in the beginning as well as how their views changed as a result of this collaboration.
One thing I am certainly curious about is in the European model where voluntary vaccination rates in certain jurisdictions are higher than in the US, how much of that could be confounded or due to public/subsidized health-care compared to the US? I’m certain Medicaid cover vaccinations for children of poor families, but then after a certain income level,
Hungary has a very high infant vaccination rate. This entry mentions “we’d have to live in a totalitarian dictatorship to get the kind of levels”, which might point in the direction of how that tradition started.
I was born in 1985, and as an infant I got vaccines against at least diphteria, polio, measles, tubercolosis by the BCG vaccine, rubella, and tetanus. (I do not claim to be effectively protected against all these diseases, in particular, the tetanus vaccine is known to give protection only for a short time period. There are a few more vaccines I got as an infant or as a child, but I don’t have adequate documentation to tell what exactly.) People of my age are typically also vaccinated against tick-based encaphelitis, but I am exempted for medical reasons (meaning that I got very sick for an unknown reason shortly after I got the first of multiple shots). The set of vaccines people get have changed since, as https://www.xkcd.com/1950/ illustrates: I am among the Brians, I got varicella as a child because there was no vaccination yet. I am not familiar with the actual policies, neither the ones when I was an infant nor the current ones, but I know there’s been public campaigns to convince adults to get certain vaccines, including the one against Hepatitis B and yearly flu vaccines. Most adults have to pay part of the cost of these vaccines, but certain people in the endangered population get them for free, eg. yearly flu vaccines are free for the elderly and for teachers in primary education.
Obviously the publicity campaigns are there because not enough people get the flu vaccines to prevent epidemic outbreaks in all years. Basically the vaccine situation is much worse for adults than for children.
—–
In Hungary, pet dogs get mandatory rabies vaccination. There are rules for mandatory vaccinations to pets in many countries. These rules are taken so seriously that it is well-known that bureaucracy makes transporting pets through country borders in Europe very difficult, because every country requires different forms of documentation from vets. So I have a question. Do you happen to know of any research studies on how vaccination affects immune system diseases in dogs?
> In order to recommend that vaccination, as a matter of public policy, should be mandatory, we would need >to show that:
> 1) Vaccination achieves a legitimate public policy objective
> 2) This public policy objective cannot be achieved without making vaccination mandatory
You would also need to show that the legitimate public policy objective is worth the costs of regulation–both the financial costs and more fuzzy costs to freedom/legitimacy.
A bad question. The epidemiological differences between the hundreds of different {disease, vaccine} pairs are overwhelmingly important and the question makes no distinctions. The whole thing can be framed more usefully as:
(1) which vaccines should be mandatory under which circumstances?
(2) which non-mandatory vaccines should be encouraged and/or subsidized?
(3) who should decide whether to add or remove a vaccine for the list in (1)?
Once you notice that there are hundreds of vaccines, only a small fraction of which are mandatory, and that there are some vaccines on the list which probably don’t belong there, you will be better equipped to debate this than most of the anti-vaxxers, who lump all vaccines together, and than most of the anti-anti-vaxxers, who never get beyond “the science is settled” and imagine that the list of mandated and recommended vaccines was immaculately conceived rather than hammered out by a messy process involving lots of committees and diverging interests.
On libertarian principles, I’m against mandating vaccinations except when there is a public health emergency. Achieving herd immunity against deadly or permanently disabling diseases is the only reason I would accept mandating vaccinations, but the worst infectious diseases rarely meet this condition (measles is the best example to argue for mandatory vaccination today, but only because smallpox and polio are no more).
That is a fair point. Not all vaccines should be mandatory, certainly.
I thank the authors for their work in what must have been a difficult task. I am a vaccine supporter, but, their review has made me curious as to whether vaccine mandates are the most effective pathway to meeting public health goals via widespread vaccine adoption. They rightly point out that any intervention which permanently modifies the body of a child must be subjected to intense scrutiny.
However, all in all I found this review extremely disappointing. The review fails to describe the well-described beneficial effects of vaccinations, and utilizes faulty reasoning in justifying concerns that vaccines could possibly cause significant harm.
I. The review does not adequately describe the benefits of vaccination
Any medical decision must appropriately balance risk and benefit – meaning, expected value of the treatment of disease, and expected value of the adverse effects of treatment. The authors have attempted to describe a medical decision without making any serious attempt at describing the benefits. This is negligent.
1. Basic public health aims remain undescribed and unaddressed
The very first item of discussion is “1. Vaccination achieves a legitimate public policy objective.” I found no explicit description of that objective.
Despite their stated aims, there is basically no discussion of the consequences of tetanus, diphtheria, pertussis, measles, mumps, rubella, meningococcus, polio, smallpox, H flu, pneumococcus, hepatitis B, hepatitis A, or varicella. There are cursory references to “smallpox is gone, and polio might be soon,” but the review does not describe why we even want smallpox and polio to disappear – this is a staggering oversight.
2. Rotavirus symptomatology is inadequately (and misleadingly) described
The review also describes that, in the third world, rotavirus vaccination can prevent deaths related to dehydration. This falsely implies that the only manifestation of rotavirus infection is diarrhea, and that the clinical syndrome associated with rotavirus vaccination is inconsequential in developed nations such as the US.
Epidemiologically, the authors underestimate the burden imposed by rotavirus gastroenteritis. From Prevention of rotavirus gastroenteritis among infants and children: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2009:
Symptomatologically, the authors fail to describe the entire profile of rotavirus infection. Rotavirus can cause encephalitis, meningitis, and seizures in 2-3% of children. Furthermore, it can cause intussusception, at higher rates than rotavirus vaccination. From Potential Intussusception Risk Versus Benefits of Rotavirus Vaccination in the United States Pediatric Infectious Disease Journal 2013 :
3. Straw argument regarding the public health benefits conferred by vaccination
The review states that “We’d have to live in a totalitarian dictatorship to get the kind of levels we’d need to eradicate rotavirus through vaccination alone… as a matter of public policy rotavirus vaccination cannot be expected to prevent outbreaks.” This is a motte-and-bailey – eradication of rotavirus may not be achievable, but that does not mean the same thing as preventing outbreaks. Neither does it mean the same thing as (or necessary for) significantly reducing healthcare utilization and bad outcomes. The authors essentially claim “If rotavirus is too virulent to be eradicated, it’s not worth vaccinating for from a public health standpoint” and that claim is utterly false.
It is well-demonstrated that rotavirus vaccination has significantly reduced healthcare utilization. See :
Decline and change in seasonality of US rotavirus activity after the introduction of rotavirus vaccine. Pediatrics. 2009
Reduction in acute gastroenteritis hospitalizations among US children after introduction of rotavirus vaccine: analysis of hospital discharge data from 18 US states. J Infect Dis. 2010
Rotavirus vaccine and health care utilization for diarrhea in U.S. children. N Engl J Med. 2011
New Vaccine Surveillance Network. Direct and indirect effects of rotavirus vaccination upon childhood hospitalizations in 3 US Counties, 2006–2009. Clin Infect Dis. 2011
II. The review overstates the case for vaccine harm surveillance
The review goes to great lengths in order to philosophically justify eternal surveillance of vaccine safety :
However it fails to justify these claims, and furthermore, is ultimately inconsistent in its reasoning.
1. The review’s root claims regarding vaccine harm surveillance are isolated demands for rigor
Throughout the review, the root claim regarding vaccine surveillance is “The most we can say is that we don’t have evidence that a vaccine causes significant harm, therefore, no amount of evidence can prove a vaccine is safe.” This is an isolated demand for rigor. No scientific claim could ever meet this standard, and yet, we allow other scientific findings to stand and we allow science to proceed. Vaccine safety, despite its necessary high standards, is not exempt from basic scientific reasoning.
2. The claim that vaccines may cause yet-unrecognized harms must be responsive to evidence
Strength of claim is delimited by strength of evidence. There is an abundant lack of evidence that vaccines cause significant harm – neither large-scale epidemiologic studies nor explorations of indirect pathogenesis has yielded any evidence thereof. From the standpoint of signal detection, the effects local to vaccinations (in temporal, spatial, and pathophysiologic senses) have been very thoroughly investigated already. If vaccinations cause harm, there will be a much greater distance from any instance of vaccination and the effect, and the detection of that signal would be subject to a prohibitive degree of statistical control and alternative pathophysiologic hypotheses. Therefore, detection of a significant harm signal attributable to vaccinations is unlikely ever to occur.
This means that the strength of evidence in favor of vaccine harms is, and likely will remain, extremely weak. Therefore, the claim that vaccines may be harmful is weakened. It is indeed irrational for this claim to remain unweakened by evidence.
3. Vaccine adverse events are unlikely to ever clear the clinical significance threshold even if a signal is detectable
Low-intensity signals should be met with low-intensity responses. The more evidence and surveillance required to detect an adverse effect of a vaccine, the smaller its effect size must be, either in terms of its frequency, its morbidity, or both. As such, the longer it takes to discover these effects, the more they will be outweighed by the benefits that the vaccine confers. At some point, there will be no events of clinical significance left to discover.
4. In light of 1-3, advocating for persistently high levels of vaccine surveillance is essentially petitio principii.
To advocate for continued intense vaccine surveillance (in order to justify vaccine refusal) is to posit three things : that vaccines can never be adequately proven safe, that gathered evidence of vaccine safety need not delimit our ongoing concern for vaccine harms, and that the intensity or clinical significance of a vaccine harm signal need not delimit our response to that signal.
This is essentially begging the question – assuming that one day vaccination will be linked to some harm, and that this harm will justify halting vaccinations.
5. The authors implicitly endorse point 4 when they mention their agreement that vaccines do not cause autism. The line of reasoning the authors use to justify claims of ongoing intense scrutiny of vaccine safety is practically identical to the line of reasoning used to justify claims that vaccinations cause autism.
I didn’t follow the line of reasoning that “things which cause a permanent effect must be subjected to more scrutiny.” Painting my front door blue is a permanent effect. Should the government form a subcommittee to scrutinize whether I can do that? Clearly not.
It would be more reasonable to say that things which look risky should be subjected to more scrutiny. So do vaccines look risky or not? I think both of the authors would agree that they don’t look risky, based on the evidence presented here. On the other hand, letting kids go unvaccinated is known to be risky. It only takes one traveller or visit from a relative to get your unvaccinated kid sick, possibly fatally.
So, to me the conclusion comes out of left field here. Sure, drinking a 24-pack of beer and driving 100 MPH on the highway is known to be dangerous. But what about the risks of NOT doing that? I mean… we can’t find any, but maybe they exist!
Consider the decision to make visible marks on your body. The decision to get a permanent tattoo must be subjected to greater scrutiny than the decision to get a temporary tattoo.
Permanent tattoos involve greater risk: the risk that you won’t like the tattoo in the future. On the other hand, painting my door is not risky, even if the paint is permanent. So again it comes down to risk, not permanency.
Pontifex. I am not saying that we pay attention to permanency instead of risk. Of course risk is the dominant feature of the decision.
I am saying that permanency effectively magnifies risk. We have to be more careful with decisions whose effects can not be undone.
On the point of how well do we actually understand all the harms, your rotovirus stats cited are from 2013? If you look at the current CDC stats, they estimate the risk of intussusception from rotavirus vaccination “to range from about 1 in 20,000 to 1 in 100,000”, which, if I did the math right, is 2-7 times riskier than what your citation claimed.
The biggest problems I see with mandatory vaccination are:
1. There are some vaccines which do have a proven higher risk than reward. Those also tend to change over time as the disease dies out and/or the vaccine becomes less risky/more effective. Based on the current recommendations, I’m not confident in the ability of the political/bureaucratic process of making the best decision on that for everyone else, above my ability to make it for myself.
2. Absent overwhelming evidence the only way to prevent harm to others is to override individual choice, people making their own decisions for themselves is the best system
The paper I cited used a risk of vaccination related intussusception of 1:50,000.
Well done,
The conclusion seems premature. Just because Germany, Ireland, and England can achieve herd immunity does not mean America can. Perhaps what allows them to achieve herd immunity is transferable to America such as bgulino’s suggestion but perhaps it is just the general conformity and deference to authority that Europeans have culturally more than Americans do. The experience with California they mention would seem to undermine the idea that recommended the vaccinations is enough to achieve safety.
Thanks. I felt that the Disneyland example was directed at those who wish to change from mandatory to voluntary vaccinations. What would happen in the real world in, say, Arizona if there were a high-profile outbreak tomorrow? Likely legislators would say, “We need herd immunity, and our neighbors in California got it by using mandates. If it worked for California, it will work here!” So the emergency fix is going to be mandates.
The message to those who oppose mandates is clear: if you want to continue to have vaccination be voluntary, you have to do the work to make that happen. That means crafting solutions that actually boost vaccination rates, and improve protection of vulnerable populations, to prevent the next outbreak. You can make it happen without mandates, but if you wait and hope declining vaccination rates will signal a “wave of popular dissent against vaccination policy” you’ll be doubly disappointed when that wave switches direction because of an outbreak. Because once the outbreak happens, you’re likely to see popular support for mandates.
How much do we know about the Disneyland outbreak? Specifically, do we know anything about Patient Zero?
Disneyland is a major tourist destination. The original source, and the majority of those who contracted later, could easily have been from out of state – or even from foreign countries.
If you’re going to place the blame for a disease outbreak at the feet of the legislature of California, Disneyland seems like the least plausible place for such a thing to occur.
In a herd immunity model, why would it be relevant whether patient zero was foreign? The point of vaccinating Californians is that when someone sick comes in, their disease can’t spread. If the measles outbreak was confined to Disneyland itself, fine. If it got out into Los Angeles, then it’s fair to assign blame to the legislature of California.
The legislature of California is responsible to the citizens of California. To the extent there is a major tourist attraction capable of drawing in disease from outside of California, it’s reasonable for the people of California to become concerned that what has been brought from outside California does not spread to the citizens of California. This would be a legitimate concern, whether the outbreak stayed confined to the Disneyland campus or not.
Hypothetically, if the outbreak was exclusively contracted by non-California residents, there would be nothing the legislature of California could do to prevent such a thing.
So the question of interest is, what proportion of those infected were California residents vs not?
The way it was handled in the news was something like, “Outbreak in Disneyland; Experts warn of low vaccination rates in California”. So from a purely academic point of view, you’d be interested to know if some group of Djbouti tourists – none of whom had been vaccinated – all contracted measles and caused an outbreak.
From a practical perspective, if there are a bunch of people spreading measles in my community, I’m going to be interested in preventing that spread to my home and family, no matter where they’re from. If I live in Manhattan and there’s an outbreak of zombieism in Times Square, I don’t really care whether the zombies came from out of state. I’m still concerned they’ll make their way to my home no matter how they got there. That doesn’t mean there’s anything NYC can do to prevent zombies from getting to Times Square. But practical considerations have never been a bar to calls for legislative action.
No one considered how inconvenient it is to administer vaccines for parents. In California, you are issued a yellow postcard which is manually filled out by the doctor’s office administering the vaccine. The parent is responsible for keeping the postcard and showing the card history to the school every year. Lose the card and you have to reconstruct the child’s history which may be difficult if you went to several different doctors. Oddly labor intensive and inconvenient considering all schools and all doctors offices in California have internet access. Also, typically a parent has to miss at least a half a day’s work, and the child must miss the same half day each time a vaccine gets administered. The system seems to be set up to cause maximum inconvenience for parents with minimum inconvenience for Doctors and Schools. Compliance rates would improve if a nurse showed up at the school and vaccinated everybody. Something similar to this is done in other countries and was done here in my childhood.
Compliance rates would improve if a nurse showed up at the school and vaccinated everybody. Something similar to this is done in other countries and was done here in my childhood.
I’m surprised to hear they don’t do that in America as that’s how it’s done in Ireland and, as you say, it has everyone in the class getting the same vaccine at the same time (unless kids are absent that day or the parents refused consent) so it doesn’t need one parent to take time off work and take the kid out of school to go to the doctor for the routine vaccination. And because everyone is getting it at the same time, I think that probably has a certain pressure (mild and unacknowledged) on parents to let their kids be vaccinated; someone who’s a convinced anti-vaxxer or who doesn’t want their child to get this particular vaccine will be sure to refuse permission on the consent form, but the ordinary parent who might otherwise not bother (because they forgot, it’s inconvenient to take a day off that day to bring the kid in, that day they’re all going to visit Granny on her birthday or whatever) just has to sign the form and forget about it.
“Line up and let this government employee inject your children with things” is not something that would go over very well in a whole lot of American communities (and not just rural white ones… a whole lot of minorities are very sensitive to this sort of thing as well, and with good reason).
Parents trust their own family doctors significantly more than they trust the government. Having the injections happen at school would probably increase opt-outs significantly.
The nurse is not a government employee. (In Ireland, she might be, to the extent that health care providers are necessarily employed by the government, but that is not the case in the US.) The system being proposed is that a wholesome family doctor who you already know and trust (or their designated assistant) shows up at school to provide vaccinations more efficiently.
There are maybe one or two hundred students per grade level in a typical American elementary school — their parents aren’t all going to know the same doctors. Still, recruiting a local GP or nurse is probably a better idea than trucking in some random CDC employee from the next state over.
(They’ll probably still be a government employee in that somebody’s going to have to pay them to do this and that somebody is going to be the government, though.)
RANT WARNING. This is a tangent unrelated to vaccinations or this article.
Yeah. The vaccinations I got as an infant are recorded on yellow cardboard too, and so are all the medical records written by my childrens’ ophtalmologist-optometrist. That seemed like a sane decision back in 1985, but we should eradicate that tradition as fast as we can. Ever since black-and-white photocopying got so cheap, those hard to copy yellow papers are causing a lot of difficulties to everyone. My mother and I spent probably a day combined to get a readable photocopy of those ophtalmology records, so we can present them to my adult ophtalmologist while the childrens’ ophtalmologist can get the originals back, since they were handwritten in only one copy.
There should be a principle that all important documents shall be written on white paper. If possible, we should also push for black ink rather than blue in pens and stamps. I’d like to go even further, by banning the use of thermal printers and laser printers for such documents, since the documents printed by those are often unreadable after a few months, but using more long-lasting forms of printing would cost a lot of money. Recipes on thermal paper often have a label on their back that the document is guaranteed to be readable for 8 years if stored between 18°C and 23°C temperature and between 42% and 58% air humidity. Needless to say, private individuals cannot store their documents under such circumstances, and even in libraries and museums, maintaining such conditions to protect old documents have a high cost. Ever since the local public transport company started printing all their tickets and passes with these fancy new laser printers a few years ago, I can’t figure out a way to make sure that my bus pass is still more than barely readable at the end of its three month period of validity, since I must carry the original with me every day.
I’m probably voting for this submission because it has been the most informative
A question re. the common argument about herd immunity: the idea is that vaccination for those who can do it will function as a protection for those who can’t. But the very fact that there exist people whose systems can’t handle vaccination implies that there is at least some burden on the system involved. This, then, begins to sound like a demand that the healthy “take one for the team,” so to speak, because their immunity will protect the less healthy. But I’m not comfortable with that (this is not an argument against vaccination, but an argument against making them mandatory, assuming I’m correct that some level of risk/physiological burden is involved).
Except that vaccination actually benefits the person getting vaccinated (assuming protective antibodies are produced as a result, which is not 100%). So those who get vaccinated are highly likely (it differs based on the vaccine) to become immune to getting sick themselves, thus it’s a concrete benefit to the one who gets the intervention, with a spill-over benefit to society.
This would be like if I told you I would roll a 20-sided dice, and if it came up as anything other than 17 I would pay you $100, and everyone else would get $1. (For 17, nobody gets anything, but we continue around the circle rolling dice based on the same rule.) That’s not asking you to assume a burden at all. You would be missing out on a clear benefit if you chose not to participate in the bargain, but so long as you’re part of the circle, you still get the payout.
Well, yes, obviously there is benefit to the individual. But the case for mandatory vaccination tends to imply, if not explicitly state, that there is zero (physical) cost for the individual to weight against the expected benefit. But if that’s not actually the case, then forcing a choice on people arguably becomes more problematic, even if the cost-benefit ration is very favorable, objectively speaking.
I guess it is similar to the question of mandatory schooling, both because it is imagined to be mostly all benefit for the individual and society and because the “free choice” aspect is complicated by those involved being children.
Good point. At the very least, not getting vaccinated means you don’t have to get poked by a needle. Sure, it’s a momentary pain, but it’s a huge factor in people not wanting to do things like give blood, so it’s maybe non-negligible for some.
As to the assumption that vaccination produces some internal, non-negligible stress to the immune system I don’t think that’s really a concern for most people. The thing to remember is that your immune system is constantly fighting off hundreds (at least) of different types of threats right now, as you’re reading this. One additional faux threat is just another day at the office for your T-cells. People think, “but won’t that make me weaker while my body is attacking the vaccine?” except that there’s a reason we give combination vaccinations. Any living organism incapable of robustly fighting off multiple attacks at once was long-ago selected out of the population.
Right, but if something clearly and uncontroversially benefits the individual – there would be no need to make it mandatory.
I think onyomi’s point is that any argument for mandatory vaccination contingent upon the fact that it will establish herd immunity and thereby benefit those who cannot be vaccinated is, very much, a “take one for the team” sort of argument of the style that demands sacrifice from Group X to benefit Group Y.
My skepticism of mandatory vaccination has always relied upon a similar argument. Something like “If you’re so confident these vaccines work, what do you care if the neighbor kid isn’t vaccinated? Your child will get the vaccine and be protected, right?”
All things are unclear or controversial if you ask enough people and if opposition to those things happens to have become a meme.
If my kid has childhood leukemia, or had to receive an organ transplant, or is on certain medications for their chronic RA or psoriasis, vaccination may not be an option for them.
The benefits to vaccination are sufficient that my children (who don’t have any of the above problems) received all of their vaccinations. The cool thing about herd immunity is that is protects the sick, elderly, or otherwise immuno-compromised in addition to those who receive the vaccine itself.
You’re arguing that this is like if a rich guy invests a bunch of research to find a cure for some disease, and suddenly he doesn’t have to worry about it anymore. But you don’t have to worry about it either, even though you didn’t pony up any money for it. You’re arguing that it’s a positive externality generated by an action that is personally beneficial but has some concrete costs. I’m just asking, what costs?
In order to “take one for the team” there has to be something that’s actually being taken. A poke in the arm? Sure. I’ll take that.
You will, but many won’t.
My point is, the justification for mandatory vaccination depends on one of two unique arguments.
1. A paternalistic argument that individuals should be vaccinated “for their own good.”
2. A “needs of the many” argument that individuals owe a duty to the rest of society (in particular, those who cannot get vaccinated)
Now, it’s possible that both of those arguments are true and morally justified. But that doesn’t make it okay to simply combine them and equivocate them.
More specifically, a lot of people make Argument #2, and then when someone counters with “Gee, that sounds very authoritarian. We don’t generally go for that sort of thing in our society. It’s not cool to force someone to do something they don’t like because some other person might benefit from it,” the response is often “Well it’s for their own good anyway” (argument #1).
Make Argument 1 or Argument 2, but don’t make one, then try and switch to the other as soon as someone challenges you on it.
The type of bait-and-switch argument you outline is certainly employed. But I would like to point out that I haven’t done that here.
My point wasn’t, “It’s good for everyone; wait, you don’t like authoritarianism that sacrifices the good of one for the needs of the many? Well it’s good for the one, too, so make them do it anyway.” Honestly I haven’t maintained a mandate recommendation. I have maintained a “herd-immunity is good public policy however that is achieved” recommendation, while rejecting the claim that this is a trade-off system of the needs of the many/few variety.
I know this is a subtle distinction, but I’m actually responding to the claim above that, “if it helps everyone this implies it at least marginally burdens the individual”; and claiming that’s not supported by the evidence. I’m asking “what is the harm?” Besides a needle poke, or very rare, known, and often avoidable complications where is the harm to the individual?
The philosophical question of whether force should be employed to implement a medical intervention that benefits both the individual and society is a separate question. If we can achieve herd immunity without you having to get the vaccine, that’s great for you and I hope you don’t contract the disease when traveling abroad, or meeting with a large group of similarly non-vaccinating people. Meanwhile, I’m going to get it because I personally benefit from it.
I am not harmed by it.
That’s because central examples of authoritarian things harm one person for the sake of others. If the thing doesn’t harm the person, and in fact helps him instead, it’s a non-central example of authoritarianism and “authoritarianism bad” is implicitly about central examples.
I don’t know – but presumably there must be some, or the individuals wouldn’t resist it so vehemently.
You may counter with “These individuals are misinformed – they think there is harm, but they are mistaken” to which my response would be either
1. It has not been scientifically proven that all vaccines are clearly and obvious free from all harms
or
2. Authoritarian practices and behaviors, in general are considered harmful (in the US at least). The loss of liberty to make one’s own decisions is a harm, in and of itself. Freedom and liberty are positive virtues and being denied them is a harm, even if the end result is “only a needle poke.”
I would not counter with “they are misinformed”. Though that is true for some individuals, others are well-informed of the research that fails to detect any harm, despite really trying to find some. The reason, I believe, that some individuals opt out is not due to harm, but due to perceived risk.
1. It’s impossible to show something is absolutely safe. Everyone has to make judgement calls based on the safety of doing (or not doing) things every day. People who opt out of vaccination are – in my opinion – making a basal judgement that vaccination by its nature is suspect as harmful. I think there will always be people who reject just about any innovation, no matter how innocuous the evidence suggests it to be. (In the early days of printing, people used to be skeptical of reading – and not just because of political/religious revolutionary implications, but as a potentially risky activity in and of itself!) I suspect this may be a survival mechanism for the species such that we don’t accidentally wipe ourselves out in the event that the 1-in-a-million “but there could be some harm we just missed somehow” statement actually turns out to be true.
2. If all government intervention of any kind is “authoritarian” and must be avoided at all costs, you have to either become a non-agression principle anarcho-libertarian, or accept that outside that small group a certain degree of centralized control will always be warranted in civil society. Everyone’s threshold is different, though, and I suspect the poke in the arm (or more practically, the removal of the ability to make a medical decision on behalf of your child) is sufficient for a small percentage of people to pass the threshold of “too much authoritarian intervention for my taste.”
@sclmlw,
In regards to risk of harm, I assume you’re aware that all vaccines have a risk of mild, moderate or severe negative reactions among the general population. Even an organization as pro-vaccination as the CDC recognizes there is no vaccine which is “100% safe” for everyone who has ever been vaccinated for it and some vaccines have even been pulled because of the high number of adverse reactions after their use became widespread and initially recommended, so I’m not sure how your concept of “there is no risk” to rolling the dice with no downsides is an accurate analogy.
Let’s take the polio vaccine as an admittedly extreme example. Not only are there currently many more negative reactions to the vaccine each year than there are cases of polio contracted in the U.S., but there were 3x as many cases of vaccination causing polio paralysis in the world last year than new cases of regular polio. The caveat is that the numbers of all of those are tiny, but it’s a persistent trend, not a one-year thing, the point being that what makes sense (inoculate everyone against X!) one day may make less sense another day.
Another bad risk ratio is probably your mentioned rotovirus vaccine, with somewhere around 1 in 20K to 1 in 100K at risk for Intussusception vs. something like a 1 in 6M risk of death from rotovirus in the U.S., most of those victims with population characteristics which don’t generally get vaccinations anyway.
Despite those examples, I’m not trying to say that no vaccines ever make any sense to use. What I’m saying is that an individual should be able to asses their own risks and make their own decisions (based on plenty of medical advice) on which to choose and when, rather than a one-size-fits-all mandatory program which substitutes centralized and political/bureacratic decision-making for an individual’s local knowledge.
On an unrelated note, the other issue not really addressed in this collaboration is vaccine boosters. Specifically, I question the numbers in the table about herd immunity related to Td. Are they missing the adults in the population? Or assuming if you’re vaccinated as a child, you’re done?
The media and medical establishment seem to super-focus on children getting vaccines and not on adults getting the ones they need. In terms of herd immunity, there are a lot more adults than children in the population. I have various skeptical answers as to why that would be, but perhaps someone has a non-skeptical explanation as to why adult immunizations don’t matter as much.
@Matt M
I pretty much agree with the counterargument you then put in the mouth of your opponents, and disagree with your arguments against it.
The “harm” is that it overrides/disagrees with stupid beliefs not based on real evidence, and doesn’t let the individual “harmed” get away with making decisions for someone else on the basis of their own incompetent or biased judgment.
Anti-vaxxers seem to me to come in two categories
– credulous ninnies
– would-be free loaders, who want to benefit from herd immunity personally, without contributing to it, and without having specific medical reasons why they cannot/should not participate.
I don’t much care if the credulous ninnies refuse vaccination on their own behalf. But I’m somewhat concerned for the health and safety of their offspring, and to a lesser extent for that of those of their neighbours who do have medical reasons not to be vaccinated.
Culturally, we have a history of letting people do any damnfool thing they want for religious reasons. It only gets controversial in the edge case, when non-believers in the religion in question see someone refusing treatment on behalf of a minor who will, predictably, die without treatment. (Blood transfusion cases, generally.) We routinely let them impose silly risks on their children for religious reasons.
But let’s at least not extend that tolerance to non-religious source of damnfool decisions that harm other people.
That’s not to say that I think all vaccines should be mandatory. Just that I’m heartily sick of people claiming to have a natural right to have their ill-informed and generally evidence-ignoring opinions treated as if they were reasonable.
You can have any opinion you want. But if you acting on that opinion is causing harm to others, you should still be held accountable for the harm you cause, and in some cases prevented from causing it in the first place. And that’s true even if you don’t believe in that harm.
I’d find it a lot easier to discuss which vaccines should be mandatory, if any, with people who shared that basic starting point.
[Edit – there’s also what seems to be an evidence-based objection to some vaccinations, as raised by sharper13. When the total harm being caused by the vaccine approaches the total harm being caused by the disease, we’re in an entirely different situation. But given the numeracy level of the average person, I’d be amazed if most of those deciding against vaccination would be capable of making a realistic, data driven argument of that kind.]
Some % of people are lazy, and/or too stupid to pour piss out of a boot. Mandatory means that they too have to do what they ought to do, but wouldn’t otherwise do because they believe some snake oil salesman, or are too busy sitting around watching TV.
Others make bad judgments about relative importance, or urgency. (Welcome to my job, where ‘urgent’ regularly crowds out ‘important’.) It’s not very important whether you get the vaccination today or tomorrow or next week … but that pretty easily turns into never. Mandatory deadlines convert important-but-not-urgent into must-do-it-right-now.
In some cases, something is mandatory for stupid reasons – it really wasn’t that important – because voters and politicians are equally prone to failings as humans acting in other capacities. (Welcome to some of the rules about air travel, post-9/11.) In very few of those cases, it’s also harmful enough to be worth circumventing the rule. But that’s extremely rare, in spite of “rugged individualism” memes to the contrary.
TL;DR – I think making some things mandatory is good.
I recall reading, years ago, some interesting research suggesting that vaccination stress may cause benefits in itself.
What I remember – hopefully correctly – is that the researchers vaccinated children in some 3rd world villages in 2 waves, 2 or so years apart, examining all the children on both visits, recording some basic statistics. The ones vaccinated in the early wave grew more in the intervening period. The researchers had some reason to believe that this was not because the unvaccinated ones caught whatever the others were vaccinated against. (Perhaps it was something that tends to be lethal.)
I can pretty easily poke holes in that single study, and the hypothesis being tested was benefits of physiological stress, not of vaccine stress in particular – they just wanted an ethical way to impose stress on half of a set of children. There’d need to be a lot of followup to take this as more than a hint, and I’ve no idea if additional studies were ever done. But it seems to me to be worth considering, when ‘protecting’ one’s children from vaccine stress.
Well, that’s a straw man, as is the stated debate subject. The trouble with these debates is that the devil – well, actually the essence – is in the details. Broad and inclusive statements of a thesis such as the above miss the details and therefore the essence.
isn’t it obvious that for a disease like smallpox or diphtheria, there is a stronger case for mandatory vaccination than there is for chicken pox? Doesn’t the answer depend on how virulent and how serious the condition is that we are vaccinating against? I think both sides in the public discussion tend to miss this point, which is really very far from subtle. The quoted statement, unqualified, misses it, too, as does the question posed for debate.
If the question was, “Should childhood vaccination against a disease ever be mandatory?”, I would vote Yes immediately. But as stated, the debate topic naturally leads to the interpretation, “Should childhood vaccination against known diseases always be mandatory?” I would equally vehemently weigh in against such a thesis.
If effective vaccination against the common cold became possible, how many of the pro-vaxers would say all children must take it? If vaccination against ebola suddenly became available in the midst of an ebola epidemic, how many of the anti-vaxers would oppose mandatory child vaccination against ebola?
Good point. They mentioned this up-front, but it wasn’t part of their conclusions as it should have been.
Thinking about all three of the ACC’s so far, it seems that they often resolve to “here is a set of evidence that we can agree on.” That’s pretty reasonable, and you can’t write about everything, but as a reader, I’d sort of like to see “Of the common arguments for/against the position, here is the evidence we agree is reliable, the evidence we agree is unreliable, and the foundations of our remaining dispute.”
I hope our follow up writing will do this.
This is a fairly minor side point, but I’m not sure the statistic about doctors’ willingness to change vaccination schedules means quite what the authors seem to imply. Having discussed this with a decent number of pediatricians over the past couple years, my anecdotal impression is that most say roughly the same thing: They find anti-vaxx parents immensely frustrating, but believe the best practice is not immediately to cut them loose as patients but instead to accede to a delay and revisit the issue at the next checkup. The assumption is that by a combination of steady pressure and growing confidence in their doctor’s intentions, the vast majority will eventually shed their discomfort with vaccines and get back on a normal schedule.
So for at least some doctors, changing the schedule is seen as a first-line intervention precisely for the purpose of buying time to exert the kind of soft-authoritarian influence on parents’ ultimate choices that the authors are worried about in that paragraph. Put another way, it’s a means of separating the truly convicted anti-vaxxers from those who are merely confused/distrustful and likely to change their minds as they become more persuaded of the doctor’s personal credibility.
Just to be clear, I’m not saying any of this is a bad thing. Only that I’m skeptical that the quoted statistic really reflects a general willingness to accommodate patient preferences in this area over the long term.
Having read the article, I concur.
I’d go further and say the article is irrelevant to the conclusion taken in the adversarial collaboration:
1) Delay up to 4 weeks is considered an alternative childhood immunization schedules (ACIS). This is nonsense in light of the fact that schedule differ between countries (despite in each case being based on first world doctor’s consensus), several vaccines have large windows when they can be applied and 4 weeks is the kind of delay that can very easily be caused by busy schedules and flu season even when parents try to stick to the schedule.
2) If one compares recommendations between countries (e.g. here: https://en.wikipedia.org/wiki/Vaccination_schedule) it becomes obvious that reasonable people differ on some recommendations (while agreeing on the important stuff). For instance, rotavirus immunization was only recommended in Germany in 2013 and then with a lots of caveats, saying it’s not cost effective and warning of intussusceptions. Yet in 2011, the article above treats refusal to get rotavirus immunization as an ACIS. The UK apparently does not recommend varicella vaccination, yet the authors treat failure to get it as an ACIS.
In light of 1 and 2 above, the following sentences from the adv. collab are misleading:
.. and we don’t differentiate important fro irrelevant or contentious deviations
The study does not address this. Maybe the next and the one after is just as willing to delay 4 weeks or skip varicella, that doesn’t mean people who want to skip MMR can find a willing doctor without a lot of effort.
There are parents who are nervous about vaccines but not completely opposed. They want to get their kids vaccinated, but they also don’t want a large number of vaccines at one time.
People who are strongly in favor of vaccines are against this because they’re concerned that it makes getting all the vaccines more difficult and less likely, but I haven’t seen any research on the subject.
Call me crazy, but giving a “naturopathic doctor” (scare quotes for the same reason as one might scare-quotes “young earth creationist geologist” or “atomic theory denialist physicist”) a platform to talk about vaccination seems like a really bad idea. Not that “pros and cons of mandatory vaccination” is a bad discussion to have, it’s just… Well, imagine a discussion about the safety of a new GMO with unclear safety results where one of the involved parties is Stefanie Seneff, and you’re kinda where I am. To the degree that the label “Naturopath” means anything specific, what it means really should not be encouraged or given a platform. Maybe Mark Davis doesn’t offer the typical grab-bag of alternative therapies; maybe he labels himself a naturopath in spite of (rather than because of) the naturopathic tendency towards things like homeopathy, iridology, aromatherapy, reiki, etc. Why he’d call himself a naturopath in that case I’m not sure. But that alone is a huge red flag that I’m surprised nobody has brought up yet, simply on “sanity waterline” grounds. Naturopaths aren’t doctors.
https://www.youtube.com/watch?v=uDYba0m6ztE
Just hook it on to the carpet.
Though to note:
https://aanmc.org/resources/licensure/
In many US states naturopathic physicians are state licensed etc so I don’t think that one blog debate stacks up much against the state itself endorsing them.
But we’re supposed to be better than that, dangit.
I think we ought to be able to handle hearing anti-vaccination arguments, young Earth arguments, and anti-atomic-theory arguments and consider them all on their merits. Up to any individual to decide whether it’s worth the investment of time to get into the weeds of these issues but I can’t agree that it’s a “bad discussion.” I also think dismissing one side based on the qualifications or occupation of the author is misguided. I think lots of the authors of these submissions have no qualification as experts in the subjects of these adversarial collaborations and yet they may make valid arguments that need to be assessed on their merit and not on the identity of their authors.
This falls under epistemic learned helplessness. It’s always possible that some naturopath, or creationist, or Holocaust denier, will come up with something that I can’t refute because he’s spent a lot more time on this subject than I have, because he’s better at arguing, and because he’s managed to say things that are so outrageous that no scientist has even bothered trying to disprove them. My response would be to say “screw this, convince some scientists first”, not to believe his argument because I couldn’t refute it. I’m not a perfect reasoner, after all.
That’s your prerogative but others are entitled to investigate and form their own conclusions. I’m just saying that your pragmatic decision not to look at an issue until it reaches a critical mass among authorities you respect doesn’t mean that others with a current interest have to or should make the same judgment.
I think we ought to be able to handle hearing anti-vaccination arguments, young Earth arguments, and anti-atomic-theory arguments and consider them all on their merits.
Agreed. Not because I think that [dangerous arguments] are not dangerous, but because I don’t trust any group to – year-over-year – maintain a solid record of rejecting *only* [dangerous arguments] without including [uncomfortable arguments] in the mix.
Agreed.
https://www.dartmouth.edu/~milton/reading_room/areopagitica/text.html
One of the questions for the ACC is whether people with strong disagreements can discuss issues constructively. In that context, I think this was a great pairing, and it looks like the answer is in some cases, yes.
I agree. The purpose of this experiment is to let authors who strongly disagree with each other fight it out behind the scenes and agree in presentation the facts.
I know that I am biased against anti-vaxx (some of my coworkers are dangerously skeptical of the medical environment, luckily the influx of trustworthy and sympathetic medical professionals into our workplace has helped them). But I think it was hugely beneficial to have these two Marks work together. The benefit is that they agreed to present the facts together and were mostly successful. Even the places where there are important unanswered questions, or self-contradictions are helpful for future discussion.
I see ACC as a preliminary foundation to much longer conversations. ACC cools the temperature of the conversation, so that instead of stepping on coals, we walk on cool grass.
Though there are obvious problems with general prevalence of belief (as opposed to prevalence of belief among recognized experts) as an index to truth, I think it might be a reasonable index for whether or not an issue is worth addressing. That is, the only ideas not worth addressing are those both deemed stupid by experts and which hardly anyone believes anyway. If a significant number of people believe something stupid, then refuting it is a useful exercise, if nothing else, while simply ignoring them just gives them more reason to continue creating a separate epistemic bubble because cover-up, etc.
A few points.
For a young and reasonably healthy person, sure. But make sure to factor in a rotavirus outbreak spreading to older people and immune compromised people.
For example on an eating disorder mental health ward an outbreak of rotavirus or norovirus can pose a massive risk of death to patients because they’re often already on deaths door with their sodium/potasium etc levels already all over the place and bouts of uncontrollable vomiting and diarrhea can very easily push them over the edge.
It’s not all about risk to the individual, it’s really important to count the already sick kid of the person you shake hands with as well.
We have a weird cultural exception (mostly based on history from when it wasn’t possible to get vaccinated) where people get given a free moral pass for unintentionally killing immune compromised people by means of passing preventable infections to them but “keeps you from unintentionally killing other people” still matters.
Add in that we’re pretty much at the point where we have the tools to track the spread of infections at the individual (bob->sally-ann) level and there’s no longer any reason to keep the tradition of courts not imposing civil liability for people spreading infections to others when they could have prevented it by taking reasonable steps.
I’d be interested to see what would happen to the vaccination rates in the US after the first anti-vaxer was ordered to pay lifetime care costs for a kid who suffered brain damage from a measles infection spread from their own unvaccinated kid.
Philosophically it’s no different to a property owner uphill from someone else’s property who is told about the risk of landslides and is advised to take some standard reasonable steps to stabilize their own property and chooses not to and then a landslide happens and maims some people down-slope.
if no protective measures are possible or all reasonable steps were taken then it makes no sense to hold the uphill owner liable, on the other hand if they are standard, cheap and reasonable then it’s entirely reasonable to hold the uphill owner liable.
So no need to remove peoples choices, but freedom of choice doesn’t mean freedom from consequences, particularly if your choices harm others.
The results from clinical trials are largely not promising.
https://journals.plos.org/plosntds/article?id=10.1371/journal.pntd.0004944
– For asthma there seems to be no benefit from parasitic worms.
– For grass pollen alergies there was no benefit found from hookworm and whipworm.
– In some trials patients suffered stomach problems.
– For allergic rhinitis there seems to be no benefit from parasitic worms but patients did suffer pain, flatulence, and diarrhea.
– For Inflammatory bowel disease using whipworm there were some promising early trials but better run ones showed much smaller benefits with some improvement for patients with ulcerative colitis.
– There were trials done to try to treat Crohn’s disease but they were stopped early because it wasn’t working.
– There was a trial testing hookworm against Crohn’s disease that showed no benefit after 45 weeks.
– There was a trial testing hookworm against celiac disease which showed no improvement in symptoms.
– Hookworms have been tested against Multiple sclerosis and while the trial patients showed slightly fewer new lesions (one of the effects of the disease) on scans they didn’t show any change in other symptoms.
I too would like to see some anti-vaxxers sued for the consequences of their neglect – either by their own grown children severely damaged by an illness they could have been vaccinated against, or by those severely harmed by an illness spread by unvaccinated people. Some small percentage of people will die, become sterile, be born with birth defects, etc. etc. because of illnesses that give most people nothing worse than a severe cold. Given the way US law works, the standard/libertarian remedy would be for those people, or their heirs, to sue.
And I’d really love to see the person who faked the vaccines-cause-autism research – already banned from practicing medicine – charged with something criminal like conspiracy to cause any/all deaths resulting from people not being vaccinated because of fears of autirm.
Wakefield definitely deserves to go to jail. For fraud, in the least. He should have known better, and he clearly did it for money.
Would you apply a similar standard for other government guidelines? For example, if a parent allows their child to eat a diet that is not within the official government recommendations, and then that child gets obese/diabetic/metabolic syndrome/non-alcoholic fatty-liver disease/etc. should the parents be held legally liable?
My reasoning is not based on it being a government guideline.
A big thank you to the collaborators for what was undoubtedly a very challenging project.
I thought that in the end, this adversarial collaboration was less successful than the others. It just doesn’t feel like the authors moved very much from their original positions. Reading between the lines, it sounds like Davis became more convinced that there is no good evidence that vaccines cause substantial amounts of harm, but that this ultimately didn’t shift his policy position very much.
Take these three sentences in the conclusion:
– “It is entirely understandable for concerned parents to adopt a “precautionary principle” approach to vaccination”
– “as a matter of public policy, a general “precautionary principle” approach cannot be recommended”
– “Individuals who wish to invoke the precautionary principle for themselves and their families should not be penalized for doing so.”
At the end of the essay, I genuinely don’t understand whether the collaborators believe the precautionary principle is legitimate or not legitimate or not in this case. I suspect the generally soft conclusion came about because in spite of all the research and collaboration, there remained a huge amount of space between the two authors. In the end, you settled on a pie-in-the-sky proposal that “we can achieve an extremely high rate of vaccination without mandatory rules.” Clearly this would be great — but given our present state, there seems no clear path to becoming more like Germany.
I suspect this collaboration was less conclusive because it was the most normative and least positive of the collaborations so far. Adversarial collaboration seems most promising for positive empirical questions, where the substance of debate is largely the analysis of a body of evidence, to reach consensus on what facts can be gleaned from the evidence. It seems least promising for normative questions. The position that “vaccines might cause harm in some yet undiscovered way, thus I would like to invoke the precautionary principle” may not be utility-maximizing or a good rule for society, but it is a position that is virtually impossible to assail with empirical evidence.
That’s a very good analysis of what happened here. I read the other collaborations and thought, “where was all the argument?” Perhaps they just hid it better than we did, but I suspect it’s more likely what you’ve outlined.
There are a lot of (legitimate) complaints in the comments about the soft conclusions we came to, but in the end that’s more a function of what we were able to agree to than what would have been produced from a committee vote composed of the two of us as well as 5 objective observers with no horse in the race.
Perhaps this kind of result could be tempered in the future if there were a third, arbitrating collaborator who is not persuaded by either side at the outset?
Well done to the collaborators, your efforts are greatly appreciated.
Whenever I read an essay dealing with “whether X practice should be mandatory” I expect to see some discussion around the ethics of enforcing a mandate. Lots of things are mandatory where I live, such as wearing a seatbelt in a car. If you drive without a seatbelt, you do so knowing that the state can collect a fine from you and revoke certain privileges thereafter. In-principle opposition to vaccines may come from sections of society who will be undeterred by state threats, or for whom the level of state force required to change their behaviour is unknown. In such cases, insofar as mandatory vaccination represents the “right” of a child to be healthy, this right would have to be balanced against the rights of the parent. I would be interested to read how this balance has been assessed by the state in previous cases, and how one might devise a system of punishment for violating a mandate.
Somewhat of a digression, but this phrasing bothers me. If you had told six-year-old me she had a right to be vaccinated, she would have said some possibly-less-eloquent version of “Great. I choose not to exercise that right, now get your needles away from me.” “You have a right to have painful procedures performed upon you against your wishes, and no you cannot opt out” is kinda dystopian for a serious decision of real-world policy.
Arguing that the other people around you have a right not to be infected by your lack of vaccination is one thing, or even “the rights of society”. And six-year-olds, to put it bluntly, are not always good at cost-benefit analysis; there are times when parents need to override them. But I think phrasing it as “the right of the child” (to be forced to do something we think the child ought to do) is both sketchy and dangerous phrasing.
I have a right to free speech, but that doesn’t mean I have to say whatever comes into my head. A right is not the same thing as an obligation.
Arguably, one of the reasons our Western nations have such highly accessible medical care infrastructures, is because we don’t have a large portion of the population who are constantly sick with diarrhea, measles, parasites, etc. Instead, they remain healthy and productive. Granted, perhaps making vaccinations mandatory is not necessary to maintain this state of affairs; but still, this implies that normalizing avoidance of vaccination may be highly unsafe.
Just a note on hep B vaccination – the reason this is delivered at birth is because a substantial proportion of transmission is from mother to child during labor, but vaccination can protect kids exposed at birth if given early enough. The reason the herd immunity threshold is low is because most transmission occurs within families (since hep B is only spread via body fluids) and sexual partnerships, so the average person with no relatives or sexual partners with hep B is effectively at zero risk. So, hep B vaccination at birth is very important, but it’s not equally important for everybody the way say, measles vaccination is. You can achieve a lot with hep B even if you only vaccinate babies at high risk.
In my experience, much opposition to vaccination is generated by this very early administration of the hep B vaccine. Parents of neonates scare more easily, and the more so if some medical intervention causes their baby to cry or feel pain. Perhaps if physicians offered to allow parents to pay to test the mother for hep B as an alternative to the free hep B vaccine that would alleviate some fears.
“You want to wait a couple of months to get the vaccine? Sure, how about we just run a quick test to see if your baby is at risk?” It’s probably more cost-effective to just give the vaccine to everyone, but there’s a potential benefit to helping parents not become skittish about vaccines after their first experience with them, thus leading to them opting out of all future vaccinations (for all their children). Maybe it won’t work, but it’s worth a try.
As with all of the adversarial collaborations, major props for the collaborators for putting in a ton of effort on a different question.
I especially appreciated this team’s work, though, because in contrast to the first two teams, they accomplished the following things:
1. Framed the question in such a way that their results were directly relevant to typical discussions of the issue
2. Clearly stated the initial expectations of each collaborator and what they learned / how their beliefs changed
3. Reached, explained, and defended specific conclusions, using insights from sides and making clear what factors the answers might depend on
4. Kept their analysis relatively concise without sacrificing useful information
Well done. I’m expecting to vote for this entry.
Yes, I agree. This one is the most like what I expected an adversarial collaboration to be. There’s a clear yes/no question, and the collaborators’ initial positions are stated, with one being pro and one being anti. The essay discusses the evidence for and against the question, and the collaborators agree on what conditions would have to hold for them to change their minds.
By contrast, the other two essays so far felt like vague, waffly explorations of a topic.
Yes, this is clearly the best one so far, in terms of presentation, mode of analysis, and effectiveness.
While I agree that this collaboration achieves your points 1-4 better than the previous entries and that this is good, I will not be voting for this entry, because it is nowhere near to a balanced treatment of the topic. As other commenters have noted, it is inconsistent, includes medical errors, omits any economic analysis and is too perfunctory in its consideration of the legal position.
I think the only good one so far is the education one. I don’t think this one actually meets the criteria you describe. The motte is that people should have the right to reject vaccines because modern medicine is wrong about vaccination, and the bailey is that people should have the right to reject vaccines because they can’t know 100% that they are safe and should have a right to decide. This collaboration is arguing for the bailey and ignoring the motte.
People of higher SES are likely to have children later in life, which means more potential for genetic load, which means more potential for immunological entropy.
“More potential for genetic load, which means more potential for immunological entropy”
Do you have a source for the claim that there is an impact of the different genetic load of babies born to older parents on children immune system – or better, a clear explanation for what you mean by the nonsense phrase “immunological entropy.” (Entropy of the distribution of immune cells has been shown to be a clinical indicator – https://physics.aps.org/articles/v7/57 – but that’s clearly not what you mean.)
People of higher SES probably have lower genetic load to begin with. Also, how big of a target is the immune system in our genome?
Many immune system genes are close to impossible to analyse in genetics because they’ve got such crazy high variation. Which is kinda what you want to get the best chance of surviving novel diseases.
Outside of hyper-variable regions/HLA, which parts are crazy-high variation?
Re: Ireland, you state that the vaccination programmes are not mandatory, and while that is true it is not the whole story. There is the usual schedule of vaccinations offered by GPs, which is a free programme and there’s a reminder about coming in for vaccinations when the usual after-birth visits and check-ups are done. As a data point in favour of the naturopath reservations, I note the warnings on the page about fever and blocked gut from two vaccines:
There is also the School Programme for vaccinations. I don’t know if the US has something similar on a national basis, or whether it’s up to individual states to adopt such policies, but over here since we’re small enough, it’s for all the country.
Now, it’s changed since my day – in 6th class we got the BCG vaccination, a procedure I remember to this day because I think it gave me my discomfort with needles and injections. I’m old enough to remember queuing up as a child for the sugarlump with the polio vaccine in the mass public vaccination. Measles vaccine was not common (indeed, it was not introduced into Ireland until 1985) so I got the measles as one of the standard childhood diseases (interestingly, there was a measles outbreak in Dublin in August, and a European surge in cases around the same times; it looks like people are falling behind on vaccinations possibly due to the lingering fears over autism and the MMR vaccine?). I remember the public service advertisements on the television about getting vaccinated for rubella because of the dangers exposure posed to pregnant women – probably wouldn’t pass muster today, but it involved showing a deaf child being diagnosed as deaf via testing, and the heavy-handed statement that deafness was one of the ill-effects of infection with rubella during pregnancy.
But returning to the Schools Immunisation Programme, all the recommended childhood vaccines given in the schools immunisation programme are free. Parents can opt out (there’s a consent form that has to be signed) of having their children vaccinated, but in practice it means that parents don’t have to make a doctor’s appointment and bring their children to be vaccinated, or try to remember the schedule, it all happens at school automatically. As I said, the schedule has changed and there’s a lot more vaccines since I was a child (the introduction of the HPV vaccine is the latest), but in effect it is mandatory vaccination programme.
Ya, I remember getting shots in school too.
I suspect there’s quite a few parents who are fairly apathetic and if vaccines are given through schools by default then only a few will explicitly opt out.
it’s a little like like opt out vs opt in organ donation.
Fever does not cause injury. It’s merely uncomfortable. Moreover, if a vaccination causes fever, that is evidence that the immune system is reacting to it, IE, that the vaccine is working.
It is utter nonsense to suggest that we should alter vaccine schedules in order to minimize fever.
Huh? A sufficiently high fever can cause brain damage, or kill.
This vaccine reaction may or may not ever be in that category. But your statement about fever is just plain wrong.
That’s not true.
Exogenous hyperthermia can injure or kill. Malignant hyperthermia (a rare genetic disorder) can injure or kill.
But endogenous fever associated with an immune response is nothing more than uncomfortable.
Am I reading this wrong? What you describe does not sound like a mandatory program. Just like it’s not mandatory that you sign a waiver for your kid to go to the field-trip to the zoo, it sounds like parents don’t have to let their children get vaccinated at school. They just have to opt-out, and instead of waiting (and hoping) for parents to bring their children to the pediatrician you go to where the kids are. That won’t get the children who are home-schooled, but it sounds like a very effective program to boost vaccination rates.
In the US, my sense is that it would be poorly-targeted, since we require parents to come with their children already vaccinated. So if you want to go where the unvaccinated kids are you need to look elsewhere.
We have a similar program of vaccinations in schools in Spain. The way it works is, you got the childhood vaccines as a baby, and then you get the reminder shots. There are few vaccines that are given at school that are not reminders.
I wish a health economist had reviewed this post, but since I don’t see one, I’ll chime in. (My background is in public policy, including several research projects on infectious diseases and risk analysis. I know some health economists, but it’s not quite my expertise.) Before I start, though, I want to note that the article overall is excellent. Despite that, there are some problematic claims and explanations. I’m going to focus on Rotavirus, since it seems like the least critical of the vaccines discussed.
First, there is a frankly silly claim that in first world countries vaccines don’t prevent deaths, they only provide economic and health benefits. Even the “mild” example of rotavirus kills dozens of US children per year, despite current vaccination levels. See: https://www.cdc.gov/rotavirus/surveillance.html
Second, vaccination below the herd immunity threshold is still a really big deal. The reproductive success of a virus asymptotically trends towards zero as the threshold is reached. (This is actually a cool mathematical result, and can be seen with a fairly simple differential equation model.) Anyways, it’s not all or nothing, and reducing the disease burden is a big deal. What this means is that getting a slightly higher vaccination rate can have tremendous population-level benefits. The claim that “since rotavirus is so highly contagious, really high vaccination rates are not enough to stop the spread of the disease. Thus… as a matter of public policy rotavirus vaccination cannot be expected to prevent outbreaks. It might make them a little less severe, or perhaps they’ll spread more slowly, but they’ll still happen.” is wrong, and wrong, and wrong, and bad. I can’t emphasize this point enough. Here’s a study; https://jamanetwork.com/journals/jama/fullarticle/187492 – a moderately effective program will prevent an extra 13 babies from ding a year, and have a benefit-to-cost ration of ~2, with “a net savings to society of $296 million.” We can double our money, but we can’t seem to bother picking up the money sitting in the street.
Lastly, the way the essay treats “mandatory” vaccination seems strange to me, since economists usually treat laws as costs. If you’re concerned about individual liberty, don’t make it mandatory – that’s fine. Instead, change the system to require 2 different doctors and a parent/guardian to sign any vaccinate exemption, and require the signatures to be notarized together. That will increase costs 10x as much as the “mandatory” label. No matter what, people who really don’t want vaccines will find sympathetic or apathetic doctors – the only question is at what cost. In the current mandatory system, if 77% of doctors let parents change the schedule, it takes approximately 0 effort to avoid them. If 10% did so, it might be tempting to think that parents who wanted to avoid vaccines would need to really try hard to shop around for one, but there’s this thing called the internet, and parents do a quick google search or ask their friends on facebook, and the amount of effort to find a doctor who will let them not vaccinate changes from 0 to, say, 1, on a scale from 1-10.
Helpful example and neat to hear about the asymptote! I also like your point about laws as cost, which is a great method for restricting supplies on goods to only those who really need or want them. In this case the “good” in question is an exemption from vaccinating.
The biggest problem with this essay is that while it talks about each vaccine being different, it then comes to a common conclusion for all vaccines.
In my childhood in Canada – many years ago now – there was a rather shorter list of vaccines more or less every child received, than the list in California currently. I believe they were (newly) free, or free options were available. I’m pretty sure we got vaccinated against whooping cough (pertussis) and smallpox. Probably polio too? And probably scarlet fever – another nasty disease my grandmother remembered from her youth. But we also simply caught many classic childhood diseases – including rubella, measles, chicken pox, and mumps.
I don’t recall anyone mainstream who objected; there were some religious objectors, generally regarded as nutters by everyone else – and I think they were allowed to follow their religious preferences. (I’m not even sure that vaccination was mandatory, actually.)
I’m currently somewhat bemused by the length of the list of childhood vaccinations where I now live. Given the popularity of the hygiene hypothesis, I’d kind of like to see tables including mortality rates, common life time side effects (and their rates), and other nasty issues (e.g. the effects of rubella during pregnancy) as well as herd immunity levels.
Armed with such a table, we could compare the amount of harm non-vaxxers do to their neighbours as well as to their own children, for each case, and pick the right ones to strongly reccommend, or even require, as well as which ones to give only in special cases.
Meanwhile, the numbers not vaccinating locally are high enough that whooping cough has once again become a problem; immunity does lessen over time, so now responsible local doctors are offering booster shots to already-vaccinated middle aged adults. I’m not looking forward to potentially having medical issues with immune response in old age, and perhaps vaccines as well, in an area where herd immunity is generally wanting.
“I’m currently somewhat bemused by the length of the list of childhood vaccinations where I now live. Given the popularity of the hygiene hypothesis, I’d kind of like to see tables including mortality rates, common life time side effects (and their rates), and other nasty issues (e.g. the effects of rubella during pregnancy) as well as herd immunity levels.”
Since you were a child child mortality rates have probably dropped by half an order of magnitude in Canada.
graph:
https://www150.statcan.gc.ca/n1/pub/91f0015m/2014011/c-g/figureb1-eng.gif
I’m not really a fan of the concept of “orders of magnitude” in general, but this has got to be one of the most intentionally opaque ways possible to state a numeric claim. Why not just say “rates have probably fallen by about 70%”?
And just out of morbid curiosity… were you or anyone else who cares to comment actually aware that a drop of “half an order of magnitude” is 68%?
And that’s a very good thing.
But how much of that is because of vaccinations for measles, german measles, mumps, and chicken pox, to name 4 that I and my siblings caught and recovered from?
In that time, we’ve had universal public health care instituted in Canada, which has got to be a huge confounder. Medical science/technology has also improved rather a lot, and people are living with chronic conditions that used to simply die of them.
Also, what’s happened to the rates of problems that might be exacerbated by too much vaccination? Allergies are the go-to example from the hygiene hypothesis.
…did you mean to reply to me?
@Michael Watts – oops, no, that should have been a reply to BlindKungFuMaster
As an example, I believe that the chicken pox vaccine is recommended in the US, but not in the UK, because there are apparently public health benefits for widespread chicken pox in children.
On the other hand, chicken pox is a herpes and it will never leave your neurons once you’ve contracted it. When your immune system weakenes in the old age, might it not cause harm to your brain like some other herpeses are suspected to do? I’m not sure if this would counterbalance the harms to grownups described in the article you cite, deciding this would need quantitative data that we don’t have.
I’m on the side of getting the chicken pox vaccine. My children got it, because I’d rather spare them shingles later in life.
I had chicken pox shortly before the vaccine was standard in the US. I can’t say I’m wild about the possibility of future shingles.
Shingles is a possible complication from measles which can happen decades after the first infection.
Shingles vaccine
It has to, because one of the collaborators is a naturopath, and naturopathy is pseudoscience that opposes all vaccines. He *doesn’t* think each vaccine is different, but since he’s collaborating with a scientist, he can’t say that, so he has to let the scientist write about the differences in vaccines and then make an argument that doesn’t depend on it.
This seems unnecessarily hostile and unkind.
Jiro, your statement “naturopathy is pseudoscience that opposes all vaccines” is inaccurate, I’m not sure if you have a source of information to cite or if you’re making an assumption. I explained in my introduction that naturopathic medicine “has been historically highly skeptical of vaccination in general, and the modern profession is contentiously split on the topic, with vocal advocates of CDC-scheduled routine childhood vaccination and vocal dissidents both offering continuing medical education for NDs.” For example, a group called “NDs for vaccines” (ndsforvaccines.com) delivers CE lectures at ND conferences all over the country.
Since you made such a broad generalization about NDs, I want to point out two things:
1. Attitudes towards EBM in the ND profession have shifted dramatically over the past decade or two (https://www.sciencedirect.com/science/article/pii/S2212958817300952).
2. There have only been small trials looking at what happens if you randomize patients to see naturopathic doctor, but they generally seem to indicate that patients who get naturopathic care get better outcomes with cost-savings to the system (https://www.markdavisnd.net/whole-practice)
Wikipedia calls it pseudoscience in the first sentence and says “Naturopathic practitioners generally recommend against following modern medical practices, including but not limited to medical testing, drugs, vaccinations, and surgery.”
So I’ll change that to “generally opposes all vaccines”. At least, the fact that someone is a naturopath is substantial Bayseian evidence that he opposes vaccines, especially if he’s in an adversarial collaboration about vaccines and his adversary supports vaccines.
Of course, if the naturopath coauthor were to state that he does, after all, believe in most vaccines I would take him at his word. But by default I will think he opposes vaccines.
Studies that come in small numbers can prove anything.
Most of this argument could be made substituting “fluoridation” for “vaccination”, so I smell a lot of isolated demands for rigor.
And, in general, allowing people to invoke the precautionary principle when almost all of the invocations are based on having a poor grasp of the facts, *and* there is a collective action problem, is a bad idea. If for some reason there was a meme going around saying that auto insurance causes cancer, we would not allow people who believe in that meme to drive without insurance based on letting them invoke the precautionary principle.
Fluoridation isn’t the same, though, because one house can’t effectively opt out except by choosing not to use city water. That’d be like somehow putting vaccines in the air and let everyone in a city breathe them in – in that case, it’d be prohibitively difficult to let someone invoke the precautionary principle without leaving the city altogether. But as it actually is, if we choose to allow it, someone can easily opt out of vaccines by not getting the shot.
Right, but the other similarity to the fluoridation debate is that fluoridation is unusual in the rest of the developed world, and things are fine. Less than 4% of the population get fluoridated water in Western Europe – have our teeth all fallen out? Err, no, because topical fluoride in toothpaste is much more effective – and voluntary!
The strange thing about US debates in these (and many other) areas is that so many people act like the rest of the world doesn’t exist. When other countries get better public health results with freer policies, why do people who purportedly care about public health still advocate for the more authoritarian policy? Is it the illusion of control?
Fluoridation is a non-central example of an authoritarian policy. The authoritarian element is based around mandating something that has low cost, is opposed by very few people, and causes negligible actual harm. It’s less authoritarian than plenty of policies which don’t garner similar opposition (like, I don’t know, European taxes, or European censorship laws). And like vaccination, it’s opposed mostly by conspiracy theorists who use the authoritarianism as an excuse, not by people who actually oppose authoritarian policies on principle.
You may find one or two people here who oppose it on principle, but you may also find one or two people here concerned about wild animal suffering.
No, those features are typical of real-world authoritarian policies. Consider mandatory church attendance in an almost-entirely Christian country, or banning strange and unpopular books. But I guess the bigger point is that it probably depends on your perspective. We get used to the laws and customs around us. The first time I heard about American fluoridation laws I could barely believe it. If I was American I’d probably shrug.
I’m sure you know that plenty of Americans are bitterly opposed to European tax levels and systems, and opposition to higher taxes is a central feature of American politics, compared to which fluoridation is non-existent. What are you trying to say here?
These
1) cause little harm on the average, but cause lots of harm to the individuals they do affect
2) involve bad goals–that is, they are causing harm in the service of causing more harm, rather than causing harm in the service of doing good.
Fluoridation is opposed mainly by scientific crackpots and conspiracy theorists who retreat to “well, it’s authoritarian” as the bailey to their motte. They don’t oppose equally (or greater) authoritarian things except by coincidence. The remaining ones are mostly Internet contrarians who still don’t oppose other things that are equally authoritarian (which doesn’t just include European taxes, but any taxes). Principled, consistent, opposition to fluoridation is basically nonexistent.
I agree that Flouridation is a bad example, but for entirely different reasons.
It’s not really authoritarian in the sense that it doesn’t really aim to get involved in people’s personal lives. It doesn’t aim to force everyone to consume flouride. It’s simply the owners and managers of a particular asset (in this case, the city water supply) deciding how to best manage their asset.
Anyone who wants to escape it can simply not drink tap water. They can buy bottled water, they can move into the country and have a well, etc. This isn’t authoritarian in the sense of other laws and regulations requiring people to do X for X’s sake.
If you’re going to set up a society such that the state owns the water supply, then the state is going to regulate the water supply as it sees fit. Flouridation, in this sense, is no more or less “authoritarian” than states who choose not to put flouride in their water supply.
So-called “negligible amounts of harm.”
Yes, water fluoridation is unusual in the rest of the developed world. I’m not necessarily for it — it seems that it is quite wasteful (since most fluoridated water doesn’t get used for drinking) and might have negative health impacts. However, it is certainly worth mentioning that, according to the article you linked, milk and salt fluoridation is widespread in European countries, which is definitely less wasteful but also definitely not topical.
>salt fluoridation
Interesting. I hadn’t heard of that before.
If the salt is also iodized, does bromine feel left out (also astatine, but it decays…)?
I have trouble with the logic of saying that mandating vaccination is unwarranted because if vaccination is voluntary, everybody will still be vaccinated. This would suggest that if people didn’t want to be vaccinated (and vaccination had the same effects), mandating vaccination would be the right thing. But “we won’t make you get vaccinated, as long as you voluntarily choose to get vaccinated” is even less of a grant of freedom than the legendary “any color you like, as long as it’s black”. You couldn’t get a Model T in red, but you didn’t have to buy one at all. I do not believe that the population’s tendency to vaccinate or not can logically figure in to whether it is warranted to mandate vaccination. Cost-benefit analysis, sure, but it appears to me to be a mistake to include an assumption about counterfactual vaccination rates in the analysis of whether to mandate vaccination.
Edit: and per False’s comment right above mine, that assumption is not even correct.
You’re confusing individuals with the population. It’s totally fine if Jack Randomguy isn’t vaccinated, as long as everyone around him is – herd immunity will stop there from being any epidemics, and protect Jill Allergic who can’t get vaccinated. The problem is if there’re enough Jacks to take us below the herd immunity threshold.
So, if everyone else would voluntarily choose to get vaccinated anyway, it’s totally fine to make vaccination optional and let Jack choose not to get it. But if a lot of people would choose not to, then it needs to be mandatory. I suppose you could conduct a lottery and let a few people win the “prize” of being able to choose, but that’d be fairly elaborate to set up.
What people will choose when vaccination is voluntary is subject to change over time. That makes a policy such as
inappropriate. You appear to be arguing for the exact policy I decried in my comment:
This is deeply dishonest, and requires staging big fights every time public opinion shifts by a minor amount. But fundamentally, this policy breaks down into two smaller policies that combine to be exactly equivalent:
Hey, we’ve had American politicians argue that taxes are voluntary, because after all, you can choose not to pay them and go to jail instead.
You’re right that my proposed policy can lead to problems over time if more people start opposing vaccination. However, I still think your characterization of it equivocates on “you.” I’d rather say:
This could lead to problems over time, but the same thing applies to a whole lot of policies with small externalities: a few defections are fine, but not too many.
The reality is that the reverse is often true:
That’s effectively what the Disneyland case demonstrates. So if you’re opposed to mandatory vaccination, you need to find a way to ensure all your friends get vaccinated. The opposite is often the case, though.
That’s the same boat as a whole lot of things that someone needs to do: “Choosing chores is voluntary. What’s that? Everyone volunteered to sweep, and no one wants to clean the latrines? Okay; latrine duty is now mandatory.”
And you’ll notice that the policy response to that very common issue is to make latrine duty mandatory as a matter of policy regardless of current opinions. You don’t change the schedule just because the current crop of people in boot camp are oddly tolerant of cleaning toilets. That would mean having to change it back very quickly.
Let me put my position in other words: if there is some threshold of compliance below which enforcement would be needed, then enforcement is always warranted. Letting people believe they have a choice is a mistake.
@Michael, I’m still not convinced. Boot camp does things that way because they want to get recruits used to taking orders, they don’t have time to manage people’s preferences, and they know another batch of recruits with different preferences is coming in a few months. But, in a more stable situation, you really can settle things differently. For example, one of my two housemates really doesn’t mind cleaning toilets, and I really don’t like it. So, on housecleaning day, he always does the bathrooms while I vacuum or clean the kitchen or something else.
Or, in some towns, you don’t need rules against asking people for money because next to nobody does it. If you get too many beggars, people start wanting rules against it – but that doesn’t mean every place should pass them preemptively. (Also, they usually get struck down as against the First Amendment, but that’s another issue.)
That’s not the only policy response possible. For example, you could have a policy that rank-orders chores by desirability, then provides incentives commensurate with the nastiness of the chore.
Maybe you get the same result as just mandating that certain people do certain chores, but that doesn’t mean the mandate system doesn’t come with its own set of problems. What happens if you don’t clean the latrine when it’s your turn? Perhaps we will force you to, or punish you or whatever. We still expend resources ensuring latrine duty is done.
But in a voluntary system at least we aren’t creating disgruntled reactionaries who preach the evils of latrine duty, and make up reasons why it’s dangerous.
As much.
I think you may be confusing “opt-in” with “opt-out”. I am fully confident that if we make opting out easier, while keeping vaccination as the default, that vaccination rates will remain well above the herd immunity level for stuff we care about. People (myself included) are predictably lazy in that fashion.
I think that’s consistent with the opt-in/opt-out literature in economics. I would add that any US state that allows for “personal exemptions” is effectively an opt-out state, and I don’t think that system fares worse than mandate states.
Right. What I have yet to see is any sort of proof that states not allowing opt-out manage to achieve herd immunity levels for particular diseases that states allowing opt-out do not.
In the absence of such evidence, allowing opt-outs seems like the superior alternative.
What about the Californian measles outbreak mentioned in the post?
I see two big problems with mandating and not allow an opt-out:
1. Local knowledge of conditions is superior. Let’s say your family has a history of adverse reactions to vaccinations, but your children haven’t yet personally been affected. When it comes time to decide to vaccinate or not, you may rationally believe their risk factor for complications is higher than average. See also the concepts behind The Use of Knowledge in Society. This issue tends to become worse over time. Initially, you might get widespread agreement that 5 key inoculations must be required for everyone, then over time companies lobby for their vaccine to be added to the list. A bureaucrat with friends in the AMA decides to make one a pet project of his, because despite the evidence of rarity, his kid caught that one rare tropical disease which isn’t already on the list, etc…, etc… You may think this type of process unlikely, but there is at least one required vaccine where according to the CDC’s numbers, if you don’t travel outside the U.S. regularly, you’re more likely to have a severe negative reaction to the vaccine than you are to ever catch the disease. The people affected in either case is small enough that no one really talks about it, but anyone who actually considers it can see the same result.
2. Philosophically, the default assumption should be respect for individual choice, in that we don’t force people to do something to themselves or their children without overwhelming evidence of harm to others if they don’t. Removing someone’s autonomy over their own life isn’t something to ever do lightly. When the desired result has been achieved in multiple places by means other than removing individual choice in the matter, then it’s apparent there may be a different way to achieve the goal while still respecting an individual’s right to choose for themselves.
This collaboration seems deeply labored in order to account for the views of the “not mandatory” side. There seems to be no compelling clinical data regarding any real harm caused by vaccines, and the position amounts to “maybe there could be harm in the future we don’t know about, even though we have no reason to believe this is the case”. When this sort of logic is taken to the extremes, it leads one to conclude that almost nothing can ever be considered free from harm.
Invoking the U.S. Supreme Court’s “strict scrutiny” standard as the final nail in the coffin to come down against mandatory vaccination is bizarre considering the case law on this issue (see Jacobson v. Commonwealth of Massachusetts) clearly permits the government to enforce mandatory vaccinations, even when applying the strict scutiny standard (see Workman v. Mingo County Bd. of Educ.)! How the authors feel qualified to apply this standard without any discussion of the case law nor the rationale as to why the strict standard standard even relates the issue of vaccines is a question crucial to evaluating the conclusions reached in this piece.
This is to say nothing of why non-mandatory vaccination works in the U.K., etc. There is no discussion in this piece of what factors lead those countries to reach herd immunity. Is it the medical system? Is it differences in overall cultural understanding? Does Ireland, for example, have a large anti-vaccination movement? Why or why not? If herd immunity is the only important threshold when it comes to the usage of vaccines, what are the alternatives to mandatory vaccination that would allow us to reach that threshold?
The most glaring ommision in this article is discussion of the potential harm caused by anti-vaccination rhetoric. Despite mandatory vaccination, the U.S. often does not meet the herd immunity threshold. Why is this? Are anti-vaccination misinformation campaigns to blame, in part? How can you discuss this issue without taking into account clinical studies on the harm caused by choosing not to vaccinate. You mention that there is no evidence to show that vaccines have a casual relationship to the emergence of autoimmune diseases, but there is actually data to show the opposite, that vaccines actually lower the chances of developing conditions like asthma (https://www.jacionline.org/article/S0091-6749(13)01860-5/abstract)! There is actually a plethora of data showing many other seemingly random benefits of vaccines (decreased risk of heart disease, increased iq test results).
While the previous two entries worked hard to present a balanced survey of their respective issues, this article seems to go out of its way to coddle the weaker position by providing no evidence in favor of as well as ignoring crucial evidence against the non-mandatory position.
“There seems to be no compelling clinical data regarding any real harm caused by vaccines” There are some real, if rare, harms – and they are not only for allergies. For example, intussusception after Rotavirus vaccination is rare, but dangerous – https://www.nejm.org/doi/full/10.1056/NEJMoa1303164
The problem with saying we need clinical proof for detecting increases in very rare events is that the sample needed for statistical significance makes this an impossible standard – often larger than the total possible sample in the US. For example, if a disease changes from 1 in 1 million to 2 in 1 million, if the vaccine coverage rate is 75%, the fact that 7 kids instead of 4 get the disease each year isn’t going to be able to prove anything. You need so much data that by the time you could have gathered it, they’ve changed the formulation twice.
But they are rare enough so that the benefits outweigh the harms, and the argument here is silly because it claims that this is a coordination problem, instead of a net expected benefit for all participants. The only way this isn’t true is if we consider the subjective “harm” of vaccination to those opposed to it to be due to requiring the vaccine, instead of more reasonably attributing it to its but-for cause, fear-mongering. (I claim it is a but-for cause, and vaccines are not, because safer vaccines would not prevent the harm.) The fear-mongering has measurable and proven if causally distant effects, and should be prosecuted as unauthorized practice of medicine when these individuals provide medical advice – unless they are doctors, in which case it should be a licensure issue. (And if you want to claim that it would be stifling free speech, at this point should be treated like shouting fire in a crowded theater.)
the argument here is silly because it claims that this is a coordination problem, instead of a net expected benefit for all participants
No, it is a coordination problem, because the net expected benefit to an individual gets smaller as the disease gets rarer (since your chance of catching the disease if you’re not vaccinated gets smaller as the disease gets rarer). Also, if you know you live in a population that already has herd immunity, the net expected benefit to you of vaccination gets smaller. So even if, averaged over all of society, the net expected benefit of you getting vaccinated is positive, it could still be that the net expected benefit to you, personally (or, more to the point, to your child, personally) of getting vaccinated is negative.
Gross individual benefit to vaccination is non-zero so long as the vaccination target has not be eradicated (so, not smallpox); and is non-negligible so long as the target is endemic to the region the individual resides in within their lifespan.
If you oppose vaccination, and associate with people who are like-minded, your risk of non-negligible exposure rises significantly. Additionally, if you believe the proposal that vaccines cause autoimmunity through a hygiene hypothesis related mechanism, anyone in your community may resolve upon a strategy of intentional exposure to pathogens to “inoculate” against autoimmune disease.
In practice, people act in groups, and that has group-level implications for herd immunity and non-vaccination risks.
I there’s a 1-in-a-million delta risk of a vaccine, it’s rare enough to round to zero in actual medical calculations. Even if it’s fatal.
But that’s not true of public policy, because “300 families of dead children” is a group with a lot of political power.
I agree with most of your analysis. It’s fair to say we should have looked at legal case law for strict scrutiny on this topic, but I’m not a legal scholar so I missed that. Then again, SCOTUS aren’t medical researchers, so the way they apply the legal standard will be different from how we might apply it. The case in favor of strict scrutiny in the case of mandating a medical intervention is fairly obvious, I think, when considering the history of mandated medical interventions in the US – and for vulnerable populations. Freedom to decide what permanent medical interventions are applied to you and your family seems like it should – in the least – be protected under the penumbra of right to privacy. Mandatory sterilizations or lobotamies, etc., of the past should at least give us pause when considering mandating medical interventions.
All that being said,
You’re right that there’s a lot of language that basically balances statements like, “we did not find convincing evidence of any harm” with “but that doesn’t mean there’s no harm – we just didn’t find it when we looked really hard for it.” I think that if there were any actual evidence of harm from vaccination we would see actual changes in administration/recommendations/laws for whatever vaccine causes that harm. In fact, I tried to go out of my way to point out that it’s not like we aren’t looking – constantly – for harms. We just aren’t finding them.
But I don’t think people opposed to vaccination are driven by evidence of harm. I think you probably know that, but in my interactions with my collaborator I learned to listen a little closer to the more fundamental concerns of their group. Basically, it’s always going to be the case that an intervention such as vaccination is going to produce the kind of backlash movement that we see with anti-vaxx. I’m fairly certain that once we figure out how to protect against autoimmunity and allergies the anti-vaccine side will move on to something new. It’s not based on the evidence, but on the nature of the intervention. So if you want to make headway on this movement, you’re going to have to first understand that their main argument is that they are not accepting unknown risks – however remote – because they’re suspicious of administering them to newborn babies everywhere. That’s not evidence-based, but it’s not wholly irrational, either. If you want them to follow the evidence, you’re out of luck. If you can find an alternative that doesn’t require them to vaccinate neonates, you’ll make much more progress. (For example, we could start a campaign to vaccinate women who are or expect to become pregnant, to promote protection through maternal antibodies.)
So why recommend against making vaccines mandatory?
Well, at the outset of the collaboration we staked out claims – and what it would take for us to reject our claims, prior to diving into the research. I noted that my objective was to achieve herd immunity, as a public policy objective that is legitimate and pressing. If that could be achieved without mandatory vaccination, then I’d concede it wasn’t required. We found nations where herd immunity was achieved without mandates, and we found that mandates weren’t sufficient in many places in the US to achieve herd immunity. That’s the goal, so clearly mandates are neither necessary nor sufficient to reach that goal. I had no choice but to concede – and I think that was the right thing to do. Meanwhile, as you pointed out, my collaborator didn’t really provide a specified alternative to mandates. In the piece I related the Disneyland case, which basically demonstrates that whether you like it or not mandates are 1) the default people turn to when an outbreak occurs, and 2) effective at increasing immunization rates. I feel like the mandate to research alternative methods of boosting herd immunity, prior to the next outbreak and casting about for solutions, falls squarely on the shoulders of those opposed to mandates. If you favor mandates, no action is required to ensure they continue, and I don’t expect a blog entry with a weak, “well they aren’t required but we don’t know how it works without them” conclusion to change that.
Finally, I agree that the language about the evidence supporting vaccines was weak, and I think that’s my biggest regret from the collaboration. However, I’m fairly certain that without that language we would have only had 3 submissions, as opposed to 4. Perhaps that’s not the best defense, but it was what I had to work with.
I would note that there seems to be no compelling clinical data regarding any real harm caused by vaccines is true on average. I do not believe there’s any dispute that there are some people harmed by them.
Note that I have second-hand experience with both the risks and the benefits of vaccines. My niece ended up with Acute Immune Thrombocytopenia as a three-year-old, which was almost certainly caused by the MMR vaccine; my nephew ended up with whooping cough at 6 months old, almost certainly caused by his parents’ delay in vaccinating him.
Same parents?
No, two different sets of parents.
And the mother of the one who got sick is one of the more forceful advocates of not delaying vaccinations, even after her daughter got sick. (She’s a nurse with PICU experience–she has a clear idea just how bad whooping cough can be.)
The two doses of MMR are given between 12-15mths and >4 years old.
How would a three year old have an immune response resulting in ITP to a vaccination given two years earlier?
” How the authors feel qualified to apply this standard without any discussion of the case law nor the rationale as to why the strict standard standard even relates the issue of vaccines is a question crucial to evaluating the conclusions reached in this piece. ”
They explain that the policy goal of herd immunity does not require mandatory vaccination. That’s a finding that would be sufficient for mandatory vaccination to fail strict scrutiny, which Jacobson V. Mass did not test.
Upholding the law on the mere basis that vaccination is at least an effective means to the policy goal, and claiming that the only way to invalidate such a rule is if it has “no real or substantial relation” to the purported goals or “is, beyond all question, a plain palpable invasion of rights” (emphasis added) is the furthest thing from requiring strict scrutiny- it is the minimum possible scrutiny.
Ref: J. V Mass
Yes, this is exactly my point. The supreme court did not believe that the strict scrutiny standard was necessary here. This begs the question of why the authors feel this is an appropriate standard, then.
Futhermore, if you take a look at the second case I aluded to, where a court did apply the strict scrutiny standard, they still find that mandatory vaccination is not an invasion of rights. That then begs a second question, that of, if a court found that mandatory vaccination does pass a strict scrutiny standard, how do the authors feel confident in saying it doesn’t?
Something of a tangent, but I’m feeling increasingly that inflammation is more responsible for more problems than is currently commonly accepted, including maybe depression and obesity.
I recently saw a video where Jordan Peterson explained to Joe Rogan how he lost a ton of weight and supposedly cured a bunch of autoimmune and depression-type symptoms by adopting a diet of nothing but meat. Apparently his daughter had done the same with even more dramatic results. He also suggests the interesting idea that maybe excess adipose tissue is serving some adaptive function in many overweight people beyond just energy storage–perhaps it helps the body better manage its processing of substances its immune system has programmed it to react to, for example. This could explain why so many nowadays seem to have higher appetite-regulated “set points” than in the past: perhaps a particular level of inflammation encourages the body to maintain a particular level of adiposity in order better to deal with whatever’s causing the inflammation.
A related, not mutually-exclusive possibility: I’ve learned over the past several years that avoiding gluten eliminates mysterious aches and pains I used to get and have also noticed that, the first time I went off it, I craved it in a strange way, and also that in cases where I accidentally ate it, I felt a sudden loss of control over my appetite (I remember inhaling a large quantity of what I thought were pure glutinous rice-based Chinese sweets that I later learned had wheat flour after investigating, the next day, the cause of symptoms). One suggestion I’ve heard for this is that, because the antibodies to the thing may harm the body’s own cells in the absence of the thing, the body ironically craves the thing as a “target” for the antibodies, though this results in more long-term production of said antibodies. If a lot of people are, unbeknownst to them, mildly allergic to a lot of foods, this could also explain what seems like a failure of appetite control.
My personal view on this is not that an all-meat diet would be healthy for everyone, but rather that some people benefit tremendously from being in ketosis, sometimes for extended periods. For reasons I don’t fully understand, ketosis seems to be a very anti-inflammatory state, so my hypothesis why ketogenic diets are so beneficial for some is that a large number of people now are suffering from problems that, at root, are all about too much inflammation.
Whether vaccines are a cause of people today being more inflamed than in the past (assuming I’m right that people are more inflamed now than they were in the past), I don’t know, but it seems possible, as does over-prescription of antibiotics and, of course, the failure of everyone to live on a farm anymore.
Not sure that farm-life was the panacea so many of us idyllically make it out to be today. People died of anthrax; people likely suffered higher rates of prion diseases and incurable degenerative lung conditions from huffing hay and livestock dander particles all day long–and this says nothing of pesticide exposure, higher rates of melanoma from being in the sun all day, etc. Also being a pre-industrialization farmer meant your body was prematurely broken from daily backbreaking labor; being a post-industrialization farmer means a greater rate of obesity-related illnesses than the general population.
“people likely suffered higher rates of prion diseases…” I’m skeptical that this is true for other reasons, but a source for this claim would be really helpful to me (for reasons unrelated to this post or discussion.)
Yeah, while I’d agree that there could be a higher incidence of prion- related disease…that’s a) relative and b) not supported by what we know.
First, the rate of prion-related disease in the UK from the BSE/nvCJD outbreak is still a rounding error on all infectious disease, neurological disease, and/or zoonotic disease. And that was a major outbreak with the full force of Western epi aimed at it.
Secondly, scrapie is a classically described disease of sheep that even today, in the wake of the BSE outbreak, is not known to jump to humans. There were also more cannibal cultures in human history than just in the New Guinea highlands – yet prion diseases are not (yet) found elsewhere.
There are a multitude of downsides to farming lifestyles – I would not put much on prions.
I mean, I’m not saying living on a farm was all advantages and no disadvantages, but it could be that an advantage was lower probability of autoimmune disorders, which may be related, I’m suggesting, to obesity and depression. And it may be that some of the very same microorganisms that protect farmers from autoimmune problems make them more prone to other problems.
The ideal, of course, would be to capture whatever advantages may have existed about farm life without actually having to work on a farm (unless that’s something you enjoy), or accept the disadvantages that go with it.
I’ve recently been reading historical accounts from the mid-1800’s. The striking feature of the accounts is how often people are sick from ‘malaria’, ‘ague’, etc. I don’t think it is sufficiently appreciated how often people used to get sick before we cut off the fecal-oral route of disease transmission.
Even if it caused good allergies and the like, we still dramatically changed the human condition for the better. The next step is to fix those pesky knock-on effects. And hope the fix doesn’t create any more.
Hookworm infection used to be quite ubiquitous, and still is, I believe, in places where people still poop outside with any frequency (its life cycle requires the eggs to mature in the dirt and the larvae to burrow into people’s bare skin, most likely around the foot or ankle). People probably underestimate the all-around health effects of plumbing and near-universal toilet usage.
Being a post-industrialization farmer also means greater risk from the machinery.
I don’t know how it cashes out in terms of lifespan.
Maybe raising chickens as a hobby makes sense in terms of health even though it’s a money-loser.
Prior to industrialization, there weren’t machines to be in danger from. Instead, there were mills (including millraces), bulls, falling trees, festering infections from bites, lung infections from sleeping above the cows, and so forth. Plus general ill health from poor nutrition in the down season.
It absolutely cashes out in the positives for post-industrialization.
Having said that – yes, being a gentleman/hobby farmer where one engages in daily physical labor and interaction with animals, with calorie intake limited (but not driven) by labor input – that is probably the best of both worlds.
Dunno how many surgeons I want mucking out chicken houses in their spare time, though…
>the failure of everyone to live on a farm anymore.
I’m amused that this correlation showed up in the post, given the early history of vaccines…
In fact, the very word “vaccine” https://www.etymonline.com/word/vaccination can be traced
to Jenner’s use of dairy farm cowpox to prevent smallpox. Best of luck to the researchers looking for the
active agent in the farm dust to prevent some autoimmune and related illnesses.