
[I am not a sleep specialist. Please consult with one before making any drastic changes or trying to treat anything serious.]
Van Geiklswijk et al describe supplemental melatonin as “a chronobiotic drug with hypnotic properties”. Using it as a pure hypnotic – a sleeping pill – is like using an AK-47 as a club to bash your enemies’ heads in. It might work, but you’re failing to appreciate the full power and subtlety available to you.
Melatonin is a neurohormone produced by the pineal gland. In a normal circadian cycle, it’s lowest (undetectable, less than 1 pg/ml of blood) around the time you wake up, and stays low throughout the day. Around fifteen hours after waking, your melatonin suddenly shoots up to 10 pg/ml – a process called “dim light melatonin onset”. For the next few hours, melatonin continues to increase, maybe as high as 60 or 70 pg/ml, making you sleepier and sleepier, and presumably at some point you go to bed. Melatonin peaks around 3 AM, then declines until it’s undetectably low again around early morning.
Is this what makes you sleepy? Yes and no. Sleepiness is a combination of the circadian cycle and the so-called “Process S”. This is an unnecessarily sinister-sounding name for the fact that the longer you’ve been awake, the sleepier you’ll be. It seems to be partly regulated by a molecule called adenosine. While you’re awake, the body produces adenosine, which makes you tired; as you sleep, the body clears adenosine away, making you feel well-rested again.
In healthy people these processes work together. Circadian rhythm tells you to feel sleepy at night and awake during the day. Process S tells you to feel awake when you’ve just risen from sleep (naturally the morning), and tired when you haven’t slept in a long time (naturally the night). Both processes agree that you should feel awake during the day and tired at night, so you do.
When these processes disagree for some reason – night shifts, jet lag, drugs, genetics, playing Civilization until 5 AM – the system fails. One process tells you to go to sleep, the other to wake up. You’re never quite awake enough to feel energized, or quite tired enough to get restful sleep. You find yourself lying in bed tossing and turning, or waking up while it’s still dark and not being able to get back to sleep.
Melatonin works on both systems. It has a weak “hypnotic” effect on Process S, making you immediately sleepier when you take it. It also has a stronger “chronobiotic” effect on the circadian rhythm, shifting what time of day your body considers sleep to be a good idea. Effective use of melatonin comes from understanding both these effects and using each where appropriate.
1. Is melatonin an effective hypnotic?
Yes.
That is, taking melatonin just before you want to get to sleep, does help you get to sleep. The evidence on this is pretty unanimous. For primary insomnia, two meta-analyses – one by Brzezinski in 2005 and another by Ferracioli-Oda in 2013 – both find it safe and effective. For jet lag, a meta-analysis by the usually-skeptical Cochrane Collaboration pronounces melatonin “remarkably effective”. For a wide range of primary and secondary sleep disorders, Buscemi et al say in their abstract that it doesn’t work, but a quick glance at the study shows it absolutely does and they are incorrectly under-reporting their own results. The Psychiatric Times agrees with me on this: “Results from another study reported as negative actually demonstrated a statistically significant positive result of a decrease in sleep latency by an average of 7.2 minutes for melatonin”.
Expert consensus generally follows the meta-analyses: melatonin works. I find cautious endorsements by the Mayo Clinic and John Hopkins less impressive than its less-than-completely-negative review on Science-Based Medicine, a blog I can usually count on for a hit job on any dietary supplement.
The consensus stresses that melatonin is a very weak hypnotic. The Buscemi meta-analysis cites this as their reason for declaring negative results despite a statistically significant effect – the supplement only made people get to sleep about ten minutes faster. “Ten minutes” sounds pretty pathetic, but we need to think of this in context. Even the strongest sleep medications, like Ambien, only show up in studies as getting you to sleep ten or twenty minutes faster; this New York Times article says that “viewed as a group, [newer sleeping pills like Ambien, Lunesta, and Sonata] reduced the average time to go to sleep 12.8 minutes compared with fake pills, and increased total sleep time 11.4 minutes.” I don’t know of any statistically-principled comparison between melatonin and Ambien, but the difference is hardly (pun not intended) day and night.
Rather than say “melatonin is crap”, I would argue that all sleeping pills have measurable effects that vastly underperform their subjective effects. The linked article speculates on one reason this might be: people have low awareness around the time they get to sleep, and a lot of people’s perception of whether they’re insomniac or not is more anxiety (or sometimes literally dream) than reality. This is possible, but I also think of this in terms of antidepressant studies, which find similarly weak objective effects despite patients (and doctors) who swear by them and say they changed their lives. If I had to guess, I would say that the studies include an awkward combination of sick and less-sick people and confuse responders and non-responders. Maybe this is special pleading. I don’t know. But if you think any sleeping pill works well, melatonin doesn’t necessarily work much worse than that.
Sleep latency statistics are hard to compare to one another because they’re so dependent on the study population. If your subjects take an hour to fall asleep, perhaps melatonin could shave off thirty-four minutes. But if your subjects take twenty minutes to fall asleep, then no sleeping pill will ever take off thirty-four minutes, and even an amazing sleeping pill might struggle to make fifteen. I cannot directly compare the people who say melatonin gives back ten minutes to the people who say melatonin gives back thirty-four minutes to the people who say Ambien gives back twelve, but my totally unprincipled guess is that melatonin is about a third as strong as Ambien. It also has about a hundred times fewer side effects, so there’s definitely a place for it in sleep medicine.
2. What is the right dose of melatonin?
0.3 mg.
“But my local drugstore sells 10 mg pills! When I asked if they had anything lower, they looked through their stockroom and were eventually able to find 3 mg pills! And you’re saying the correct dose is a third of a milligram?!”
Yes. Most existing melatonin tablets are around ten to thirty times the correct dose.
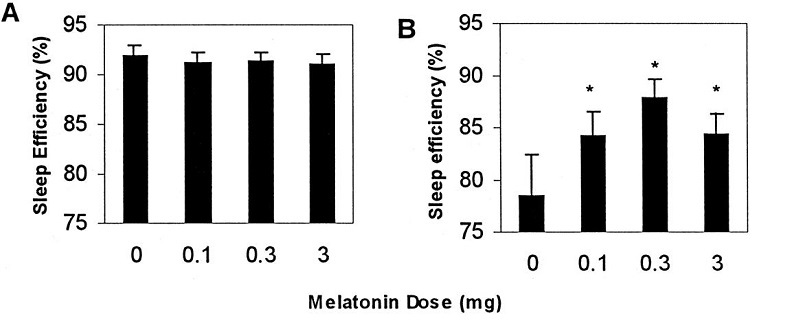
Many early studies were done on elderly people, who produce less endogenous melatonin than young people and so are considered especially responsive to the drug. Several lines of evidence determined that 0.3 mg was the best dose for this population. Elderly people given doses around 0.3 mg slept better than those given 3 mg or more and had fewer side effects (Zhdanova et al 2001). A meta-analysis of dose-response relationships concurred, finding a plateau effect around 0.3 mg, with doses after that having no more efficacy, but worse side effects (Brzezinski et al, 2005). And doses around 0.3 mg cause blood melatonin spikes most similar in magnitude and duration to the spikes seen in healthy young people with normal sleep (Vural et al, 2014).
Other studies were done on blind people, who are especially sensitive to melatonin since they lack light cues to entrain their circadian rhythms. This is a little bit of a different indication, since it’s being used more as a chronobiotic than a sleeping pill, but the results were very similar: lower doses worked better than higher doses. For example, in Lewy et al 2002, nightly doses of 0.5 mg worked to get a blind subject sleeping normally at night; doses of 20 mg didn’t. They reasonably conclude that the 20 mg is such a high dose that it stays in their body all day, defeating the point of a hormone whose job is to signal nighttime. Other studies on the blind have generally confirmed that doses of around 0.3 to 0.5 mg are optimal.
There have been disappointingly few studies on sighted young people. One such, Attenburrow et al 1996 finds that 1 mg works but 0.3 mg doesn’t, suggesting these people may need slightly higher doses, but this study is a bit of an outlier. Another Zhdanova study on 25 year olds found both to work equally. And Pires et al studying 22-24 year olds found that 0.3 mg worked better than 1.0. I am less interested in judging the 0.3 mg vs. 1.0 mg debate than in pointing out that both numbers are much lower than the 3 – 10 mg doses found in the melatonin tablets sold in drugstores.
UpToDate, the gold standard research database used by doctors, agrees with these low doses. “We suggest the use of low, physiologic doses (0.1 to 0.5 mg) for insomnia or jet lag (Grade 2B). High-dose preparations raise plasma melatonin concentrations to a supraphysiologic level and alter normal day/night melatonin rhythms.” Mayo Clinic makes a similar recommendation: they recommend 0.5 mg. John Hopkins’ experts almost agree: they say “less is more” but end up chickening out and recommending 1 to 3 mg, which is well above what the studies would suggest.
Based on a bunch of studies that either favor the lower dose or show no difference between doses, plus clear evidence that 0.3 mg produces an effect closest to natural melatonin spikes in healthy people, plus UpToDate usually having the best recommendations, I’m in favor of the 0.3 mg number. I think you could make an argument for anything up to 1 mg. Anything beyond that and you’re definitely too high. Excess melatonin isn’t grossly dangerous, but tends to produce tolerance and might mess up your chronobiology in other ways. Based on anecdotal reports and the implausibility of becoming tolerant to a natural hormone at the dose you naturally have it, I would guess sufficiently low doses are safe and effective long term, but this is just a guess, and most guidelines are cautious in saying anything after three months or so.
3. What are circadian rhythm disorders? How do I use melatonin for them?
Circadian rhythm disorders are when your circadian rhythm doesn’t match the normal cycle where you want to sleep at night and wake up in the morning.
The most popular circadian rhythm disorder is “being a teenager”. Teenagers’ melatonin cycle is naturally shifted later, so that they don’t want to go to bed until midnight or later, and don’t want to wake up until eight or later. This is an obvious mismatch with school starting times, leading to teenagers either not getting enough sleep, or getting their sleep at times their body doesn’t want to be asleep and isn’t able to use it properly. This is why every reputable sleep scientist and relevant scientific body keeps telling the public school system to start later.
When a this kind of late sleep schedule persists into adulthood or becomes too distressing, we call it Delayed Sleep Phase Disorder. People with DSPD don’t get tired until very late, and will naturally sleep late if given the chance. The weak version of this is “being a night owl” or “not being a morning person”. The strong version just looks like insomnia: you go to bed at 11 PM, toss and turn until 2 AM, wake up when your alarm goes off at 7, and complain you “can’t sleep”. But if you can sleep at 2 AM, consistently, regardless of when you wake up, and you would fall asleep as soon as your head hit the pillow if you first got into bed at 2, then this isn’t insomnia – it’s DSPD.
The opposite of this pattern is Advanced Sleep Phase Disorder. This is most common in the elderly, and I remember my grandfather having this. He would get tired around 6 PM, go to bed by 7, wake around 1 or 2 AM, and start his day feeling fresh and alert. But the weak version of this is the person who wakes up at 5 each morning even though their alarm doesn’t go off until 8 and they could really use the extra two hours’ sleep. These people would probably do fine if they just went to bed at 8 or 9, but the demands of work and a social life make them feel like they “ought” to stay up as late as everyone else. So they go to bed at 11, wake up at 5, and complain of “terminal insomnia”.
Finally, there’s Non-24-Hour-Sleep Disorder, where somehow your biological clock ended up deeply and unshakeably convinced that days on Earth are twenty-five (or whatever) hours long, and decides this is the hill it wants to die on. So if you naturally sleep 11 – 7 one night, you’ll naturally sleep 12 – 8 the next night, 1 to 9 the night after that, and so on until either you make a complete 24-hour cycle or (more likely) you get so tired and confused that you stay up 24+ hours and break the cycle. This is most common in blind people, who don’t have the visual cues they need to remind themselves of the 24 hour day, but it happens in a few sighted people also; Eliezer Yudkowsky has written about his struggles with this condition.
Melatonin effectively treats these conditions, but you’ve got to use it right.
The general heuristic is that melatonin drags your sleep time towards the direction of when you take the melatonin.
So if you want to go to sleep (and wake up) earlier, you want to take melatonin early in the day. How early? Van Geijlswijk et al sums up the research as saying it is most effective “5 hours prior to both the traditionally determined [dim light melatonin onset] (circadian time 9)”. If you don’t know your own melatonin cycle, your best bet is to take it 9 hours after you wake up (which is presumably about seven hours before you go to sleep).
What if you want to go to sleep (and wake up) later? Our understanding of the melatonin cycle strongly suggests melatonin taken first thing upon waking up would work for this, but as far as I know this has never been formally investigated. The best I can find is researchers saying that they think it would happen and being confused why no other researcher has investigated this.
And what about non-24-hour sleep disorders? I think the goal in treatment here is to advance your phase each day by taking melatonin at the same time, so that your sleep schedule is more dependent on your own supplemental melatonin than your (screwed up) natural melatonin. I see conflicting advice about how to do this, with some people saying to use melatonin as a hypnotic (ie just before you go to bed) and others saying to use it on a typical phase advance schedule (ie nine hours after waking and seven before sleeping, plausibly about 5 PM). I think this one might be complicated, and a qualified sleep doctor who understands your personal rhythm might be able to tell you which schedule is best for you. Eliezer says the latter regimen had very impressive effects for him (search “Last but not least” here). I’m interested in hearing from the MetaMed researcher who gave him that recommendation on how they knew he needed a phase advance schedule.
Does melatonin used this way cause drowsiness (eg at 5 PM)? I think it might, but probably such a minimal amount compared to the non-sleep-conduciveness of the hour that it doesn’t register.
Melatonin isn’t the only way to advance or delay sleep phase. Here is a handy cheat sheet of research findings and theoretical predictions:
TO TREAT DELAYED PHASE SLEEP DISORDER (ie you go to bed too late and wake up too late, and you want it to be earlier)
– Take melatonin 9 hours after wake and 7 before sleep, eg 5 PM
– Block blue light (eg with blue-blocker sunglasses or f.lux) after sunset
– Expose yourself to bright blue light (sunlight if possible, dawn simulator or light boxes if not) early in the morning
– Get early morning exercise
– Beta-blockers early in the morning (not generally recommended, but if you’re taking beta-blockers, take them in the morning)
TO TREAT ADVANCED PHASE SLEEP DISORDER (ie you go to bed too early and wake up too early, and you want it to be later)
– Take melatonin immediately after waking
– Block blue light (eg with blue-blocker sunglasses or f.lux) early in the morning
– Expose yourself to bright blue light (sunlight if possible, light boxes if not) in the evening.
– Get late evening exercise
– Beta-blockers in the evening (not generally recommended, but if you’re taking beta-blockers, take them in the evening)
These don’t “cure” the condition permanently; you have to keep doing them every day, or your circadian rhythm will snap back to its natural pattern.
What is the correct dose for these indications? Here there is a lot more controversy than the hypnotic dose. Of the nine studies van Geijlswijk describes, seven have doses of 5 mg, which suggests this is something of a standard for this purpose. But the only study to compare different doses directly (Mundey et al 2005) found no difference between a 0.3 and 3.0 mg dose. The Cochrane Review on jet lag, which we’ll see is the same process, similarly finds no difference between 0.5 and 5.0.
Van Geijlswijk makes the important point that if you take 0.3 mg seven hours before bedtime, none of it is going to be remaining in your system at bedtime, so it’s unclear how this even works. But – well, it is pretty unclear how this works. In particular, I don’t think there’s a great well-understood physiological explanation for how taking melatonin early in the day shifts your circadian rhythm seven hours later.
So I think the evidence points to 0.3 mg being a pretty good dose here too, but I wouldn’t blame you if you wanted to try taking more.
4. How do I use melatonin for jet lag?
Most studies say to take a dose of 0.3 mg just before (your new time zone’s) bedtime.
This doesn’t make a lot of sense to me. It seems like you should be able to model jet lag as a circadian rhythm disorder. That is, if you move to a time zone that’s five hours earlier, you’re in the exact same position as a teenager whose circadian rhythm is set five hours later than the rest of the world’s. This suggests you should use DSPD protocol of taking melatonin nine hours after waking / five hours before DLMO / seven hours before sleep.
My guess is for most people, their new time zone bedtime is a couple of hours before their old bedtime, so you’re getting most of the effect, plus the hypnotic effect. But I’m not sure. Maybe taking it earlier would work better. But given that the new light schedule is already working in your favor, I think most people find that taking it at bedtime is more than good enough for them.
5. I try to use melatonin for sleep, but it just gives me weird dreams and makes me wake up very early
This is my experience too. When I use melatonin, I find I wake the next morning with a jolt of energy. Although I usually have to grudgingly pull myself out of bed, melatonin makes me wake up bright-eyed, smiling, and ready to face the day ahead of me…
…at 4 AM, invariably. This is why despite my interest in this substance I never take melatonin myself anymore.
There are many people like me. What’s going on with us, and can we find a way to make melatonin work for us?
This bro-science site has an uncited theory. Melatonin is known to suppress cortisol production. And cortisol is inversely correlated with adrenaline. So if you’re naturally very low cortisol, melatonin spikes your adrenaline too high, producing the “wake with a jolt” phenomenon that I and some other people experience. I like the way these people think. They understand individual variability, their model is biologically plausible, and it makes sense. It’s also probably wrong; it has too many steps, and nothing in biology is ever this elegant or sensible.
I think a more parsimonious theory would have to involve circadian rhythm in some way. Even an 0.3 mg dose of melatonin gives your body the absolute maximum amount of melatonin it would ever have during a natural circadian cycle. So suppose I want to go to bed at 11, and take 0.3 mg melatonin. Now my body has a melatonin peak (usually associated with the very middle of the night, like 3 AM) at 11. If it assumes that means it’s really 3 AM, then it might decide to wake up 5 hours later, at what it thinks is 8 AM, but which is actually 4.
I think I have a much weaker circadian rhythm than most people – at least, I take a lot of naps during the day, and fall asleep about equally well whenever. If that’s true, maybe melatonin acts as a superstimulus for me. The normal tendency to wake up feeling refreshed and alert gets exaggerated into a sudden irresistable jolt of awakeness.
I don’t know if this is any closer to the truth than the adrenaline theory, but it at least fits what we know about circadian rhythms. I’m going to try to put some questions about melatonin response on the SSC survey this year, so start trying melatonin now so you can provide useful data.
What about the weird dreams?
From a HuffPo article:
Dr. Rafael Pelayo, a Stanford University professor of sleep medicine, said he doesn’t think melatonin causes vivid dreams on its own. “Who takes melatonin? Someone who’s having trouble sleeping. And once you take anything for your sleep, once you start sleeping more or better, you have what’s called ‘REM rebound,’” he said.
This means your body “catches up” on the sleep phase known as rapid eye movement, which is characterized by high levels of brain-wave activity.
Normal subjects who take melatonin supplements in the controlled setting of a sleep lab do not spend more time dreaming or in REM sleep, Pelayo added. This suggests that there is no inherent property of melatonin that leads to more or weirder dreams.
Okay, but I usually have normal sleep. I take melatonin sometimes because I like experimenting with psychotropic substances. And I still get some really weird dreams. A Slate journalist says he’s been taking melatonin for nine years and still gets crazy dreams.
We know that REM sleep is most common towards the end of sleep in the early morning. And we know that some parts of sleep structure are responsive to melatonin directly. There’s a lot of debate over exactly what melatonin does to REM sleep, but given all the reports of altered dreaming, I think you could pull together a case that it has some role in sleep architecture that promotes or intensifies REM.
6. Does this relate to any other psychiatric conditions?
Probably, but this is all still speculative.
Seasonal affective disorder is the clearest suspect. We know that the seasonal mood changes don’t have anything to do with temperature; they seem to be based entirely on winter having shorter (vs. summer having longer) days.
There’s some evidence that there are two separate kinds of winter depression. In one, the late sunrises train people to a late circadian rhythm and they end up phase-delayed. In the other, the early sunsets train people to an early circadian rhythm and they end up phase-advanced. Plausibly SAD also involves some combination of the two where the circadian rhythm doesn’t know what it’s doing. In either case, this can make sleep non-circadian-rhythm-congruent and so less effective at doing whatever it is sleep does, which causes mood problems.
How does sunrise time affect the average person, who is rarely awake for the sunrise anyway and usually sleeps in a dark room? I think your brain subconsciously “notices” the time of the dawn even if you are asleep. There are some weird pathways leading from the eyes to the nucleus governing circadian rhythm that seem independent of any other kind of vision; these might be keeping tabs on the sunrise if even a little outside light is able to leak into your room. I’m basing this also on the claim that dawn simulators work even if you sleep through them. I don’t know if people get seasonal affective disorder if they sleep in a completely enclosed spot (eg underground) where there’s no conceivable way for them to monitor sunrise times.
Bright light is the standard treatment for SAD for the same reason it’s the standard treatment for any other circadian phase delay, but shouldn’t melatonin work also? Yes, and there are some preliminary studies (paper, article) showing it does. You have to be a bit careful, because some people are phase-delayed and others phase-advanced, and if you use melatonin the wrong way it will make things worse. But for the standard phase-delay type of SAD, normal phase advancing melatonin protocol seems to go well with bright light as an additional treatment.
This model also explains the otherwise confusing tendency of some SAD sufferers to get depressed in the summer. The problem isn’t amount of light, it’s circadian rhythm disruption – which summer can do just as well as winter can.
I’m also very suspicious there’s a strong circadian component to depression, based on a few lines of evidence.
First, one of the most classic symptoms of depression is awakening in the very early morning and not being able to get back to sleep. This is confusing for depressed people, who usually think of themselves as very tired and needing to sleep more, but it definitely happens. This fits the profile for a circadian rhythm issue.
Second, agomelatine, a melatonin analogue, is an effective (ish) antidepressant.
Third, for some reason staying awake for 24+ hours is a very effective depression treatment (albeit temporary; you’ll go back to normal after sleeping). This seems to sort of be a way of telling your circadian rhythm “You can’t fire me, I quit”, and there are some complicated sleep deprivation / circadian shift protocols that try to leverage it into a longer-lasting cure. I don’t know anything about this, but it seems pretty interesting.
Fourth, we checked and depressed people definitely have weird circadian rhythms.
Last of all, bipolar has a very strong circadian component. There aren’t a whole lot of lifestyle changes that really work for preventing bipolar mood episodes, but one of the big ones is keeping a steady bed and wake time. Social rhythms therapy, a rare effective psychotherapy for bipolar disorder, revolves around training bipolar people to control their circadian rhythms.
Theories of why circadian rhythms matter so much revolve either around the idea of pro-circadian sleep – that sleep is more restorative and effective when it matches the circadian cycle – or the idea of multiple circadian rhythms, with the body functioning better when all of them are in sync.
7. How can I know what the best melatonin supplement is?
Labdoor has done purity tests on various brands and has ranked them for you. All the ones they highlight are still ten to thirty times the appropriate dose (also, stop calling them things like “Triple Strength!” You don’t want your medications to be too strong!). As usual, I trust NootropicsDepot for things like this – and sure enough their melatonin (available on Amazon) is exactly 0.3 mg. God bless them.
















Power move: reading this article at 3:00 AM when your circadian cycle wanted you asleep four hours ago.
School is really bad for sleep schedules as a teenager, and I can personally attest to that. I had to wake up at 5:30 AM pretty consistently in order to make time for the bus, and I naturally wanted to stay up until 2:00 AM and wake up at 10:00 AM, so I spent entire weeks sleeping two to three hours at night, going to school, and then napping for five to six hours in the afternoon. I probably should have gone to a doctor about this when I still had to attend, but in typical teenager fashion I didn’t think it was worth bothering with. I’m fortunate enough that it didn’t hurt my grades or performance (somehow) but I still feel the effects of it today, which is why I’m writing this comment while the rest of the eastern seaboard is getting their snooze on.
I’ve made it part of my personal mission since to get someone with any control to recognize what a bad idea the current common school schedule is. Most of the time, when I bring it up, they make some excuse along the lines of “If I have to do it as an adult, they have to do it as a teenager. They don’t get a free pass because they’re lazy.” I haven’t quite found a way to convince this type of person, and I’m beginning to think that the entire school system will be disassembled sooner than they modify their schedules to prevent sleep trouble. Melatonin helps, but I’ve found the biggest help is talking to a sleep specialist, to get the exact kind of advice you’re giving here.
With regards to the “If I have to do it as an adult, they have to do it as a teenager” thing, I think there’s also a strong argument that you *shouldn’t* have to do it as an adult. Flexible hours is more of a thing than it used to be, and there are some jobs where it’s not practical for various reasons, but on the whole our workday is pretty brutal to those people on one half of the bell-curve. Changing the school schedule is a higher priority, but changing work schedules is also important.
Flexible hours is more of a thing than it used to be,
The people in charge of this are the workers at school who do have fixed schedules, so they’ll be the last to believe you. (Even if the school day was moved or rearranged to be more targeted toward’s student needs, the teacher still needs to be there at X o’clock.)
Typical school day, at least where I’m at, ends around 3-3:30. Is there a good reason it can’t be shifted so as to start later and end at the usual 5pm?
Assuming teachers require extra work time that isn’t taken up by class time (and thus work 8-5) can’t they still work 8-5 and just do the grading in the morning?
“Is there a good reason it can’t be shifted so as to start later and end at the usual 5pm?”
So after school sports practices will still be done in daylight and so parents can send their kids off to school before they leave for work.
@James Miller why not just have school sports meet in the morning, at 6:30am or 7am or whatnot.
Because then all the teenagers will say “I am not doing school sports, if it means I have to get up at 5:00 AM”. And if we want our teenagers to average less than 300 lbs at graduation, we probably want to encourage school sports.
@John Schilling
Counterexample: Teenagers in Philadelphia will play hockey at whatever ice time is available. Whether an ice time of 5am means they stay up all night or not I couldn’t say, however. Swimmers also often have to deal with early-morning practice times.
Make practices for the prestige sports at the worst times, and I don’t think you’ll see much of a dropoff.
Part of the problem is the asumption that parents will still be needed to get teenagers to school. If parents could leave for work at 7:30 and leave their kids to get onto the bus later, that would solve a lot of the schedule problem.
I would have gotten myself to school. But I was extremely high-conscientiousness as a teenager. I would probably expect lots of other teenagers to do it, too, because I was unaware of how unusual I was.
I think you misunderstood me. I wasn’t talking about schools and teachers and whatnot; I was making a much broader statement about jobs. “9-to-5” is the expected working hours for a lot of people, and this harms all the “night owls” whose sleep cycle is later. The early people have it fine, because they can have a leisurely breakfast or go to the gym in the morning, but the late people have to wake up too early every damn morning.
There are some jobs where you can work 10-6 or 11-7 and this is very good and healthy and there should be more of it.
(EDIT: as others point out, one of the reasons the school day is early is so that parents can send the kids to school before they go to work. If flexible (or just later) work hours were common then perhaps this would open up the option of making school later.)
You won’t get through to the majority of these people because underlying most of this is the honest fact that if they have to get out of the house for work by 8am, then their kid has to be out of the house by 7:30 or else they have to rely on them to be individually responsible.
IMO, if your fourteen-year-old can’t be trusted to feed and dress herself and take herself to the bus without supervision, you screwed up somewhere in the parenting process.
Or the teenager is not completely neurotypical.
Because teenagers never have executive control dysfunctions, or serious depression, or any of the other myriad side-effects of puberty melting down and rebuilding their brains between the age of 13 to 25, and everything is the parents’ fault for how they raised the kid before puberty….
Wait, who is the scientific progressive and who is the crusty old reactionary here?
I will be blunt: your “IMO” is misinformed, unhelpful, incorrect, wrong, and hurtful.
I generally agree with your commentary, but as the dad of a 13-year-old, I think you are mistaken here.
Most people are mediocre parents, and not just in the “50% of people are average to below average” way. The major message that they hear their whole lives is that to be a good parent you need to get your kids to school, make sure they do their homework and get good grades, and they will have outsourced most of the time and major decisions of parenting because of that. A homeschooling parent can easily spend 20,000 to 50,000 more hours with their kids by the time they are 18 than a working parent. That is an enormous potential gap in skill level between different parenting choices.
Possibly nine months in advance of it, if the strong form of the nature/”parenting styles are irrelevant to personality” argument holds.
What about the other end of the day? School is out by 3, parent’s aren’t off work till 5, Kids have the same 2 hours in which to be irresponsible.
Come to think of it, they will have 2 fully awake hours to get in trouble into, where as in the morning they are much more likely to just sleep thru them.
Many teenagers I knew had after-school extracurriculars, sports, etc. that occupied those afternoon hours. And plenty of them were kids that didn’t much want to do them, but parents half-forced the issue due to work schedules.
And then sleep through most of the school day, with their parents having long since left for work and unavailable to make sure the kids get to school on time and in good order. And the best source of cheap babysitting is local teenagers, possibly the youngest children’s elder siblings, but those aren’t reliably available in the early AM either.
The issue isn’t unsupervised with nothing to do (though many kids do after school activities) it is unsupervised with something they are supposed to do. It isn’t a ‘they will burn the house down’* fear, its that they will be chronically late or absent.
*Sometimes it is, but with those parents either one is going in to work early and leaving early or the kid has after school activities every day or some combination.
I’ll bet most schools near you have both before and after school programs for children who can’t be dropped off or picked up on time. These are probably subsidized for some income brackets.
The other option is parents with two different work schedules.
Exactly this – it’s not so much about optimizing learning but rather about daycare for teenagers. I’ve briefly skimmed the 17 links in Scott’s main post and to my surprise none of them seem to address this. On the other hand several of them call for ‘raising the starting time to 8:15/8:30 am’, which seems close to compatible with a regular 9-5 job?
Well, almost everyone denies that school isn’t just a warehouse for unsupervised kids and claims it’s about education. They’re wrong, but it takes a lot to get them to admit it.
All too true. We can still hope to push for changes around the edges that slightly increase the education that happens accidentally.
When I was in middle and high school, I attended two different school districts which both considered moving start times later while I was attending them. Neither time was the altered schedule enacted. The reasoning had nothing to do with moralistic bullshit, or at least the moralists’ rationalizing arguments were good ones:
The first issue is that sports teams want to meet after school, and there needs to be enough daylight after school for students to attend practice for possibly more than one sport. Now you’d think this could be made compatible by having some sports practice before school, but:
The other issue is that a number of families rely on their older child in high school to pick up their younger siblings from elementary school, and that requires high schools to get out earlier. Due to the bus schedules, it’s important for elementary, middle and high schools to begin and end at staggered times. So if you want to make high schools start, say, two hours later, you either have to make elementary schools also start two hours later or say fuck you to the families that have their older child pick up their younger siblings from school in order to avoid paying for childcare (by making elementary schools start earlier than high schools).
The unreasonably early start times of high schools aren’t arbitrary, there are decent logistical reasons for them to be as they are, and students’ health suffers as a result.
There are often benefits that can be claimed, but they are usually gained by a rather small group of people. Looking at your example
Clearly this isn’t much of an issue for families with a stay at home parent, families with 1 child, or families with their oldest child old enough to take care of themselves, families with neighbors or grandparents who can pick up some of the slack etc. In the long run families for whom this will be a definite hardship are going to be a minority in many districts. Why would we make every high school student suffer for such a small benefit?
Seattle Public Schools recently made this change, switching the elementary school to earlier start and the high schools to later start. (The resource to deconflict were the school buses).
IIRC, in recent years some studies have found that later starting times for high schools have a pretty big positive impact on SAT scores and/or grades. Dunno how reliable those studies were, but I’m still surprised the findings weren’t sufficient to generate a sufficient push for later start times from the hyper-competitive tiger-mom/helicopter-parent types trying to get their kids into elite colleges. Maybe it’s because those kinds of parents tend to have the type of personality that regards sleep deprivation in the pursuit of excellence as a badge of honor? The Onion had a funny take on that tendency a few years ago in one of their “American Voices” articles:
“Irreversibly” is a strong word. Most screwups should be considered reversible until you get evidence otherwise.
I’ve been on a N-24 cycle for decades — staying up 17 or 18 hours, then sleeping for 8 or 9. Needless to say, my hours cycle around the clock very rapidly. Unlike some people that I’ve read about, I have no trouble falling asleep, even during the bright daylight. I just pull the covers over my eyes, and I’m out within a few minutes.
Since I was working from home (contract programming), I just put up with this. I’m disabled (paraplegic) and just wrote this off as another stupid physical nuisance I have to put up with. Now that I’m retired, I find it very isolating. People want to do things with me, or I would like to try some class or club, but I’m never awake at the right times.
I’ve tried the high dose melatonin from the grocery store, but they have no effect on me at all. Not even useful as a sleeping pill! I suppose I could try the low dose ones and see if they are different.
Have there been any studies of N-24 and paraplegics? I vaguely remember seeing some reference that it was more common with us guys in chairs.
The sympathetic nerves that stimulate melatonin secretion from the pineal originate from the superior cervical ganglion so people with cervical spinal injuries have been found in some cases to lack melatonin production, sometimes resulting in poor sleep.
Lower spinal injuries do not affect melatonin directly but there may be secondary effects on the sleep wake cycle, for example if the impairments lead to limited light exposure.
In Australia unfortunately we only have one type of of supplemental melatonin: a prescription pill called “Circadin” (not a spelling error)
It’s 2mg, released over an 8-10 hour period. Which of course will look like 200-250mcg every hour for the duration of your unconsciousness. Neurim pharmaceuticals claim this as an improvement over non-prescription melatonin. They even have Neurim funded studies to prove it. But then, of course they would.
Yes we’re from the government and we’re here to help you by making it hard to get the product you need.
Circadin is slow release but you can chew it to defeat the slow release.
In my experience there is little drama with importing melatonin from the US, either by mail order or by having friends bring in say 3 bottles on return from the US. I always declare it to customs and have never had it taken.
Personally I find the slow release forms useless. They do not get me to sleep fast and they leave me tired in the morning due to leftover melatonin. When you look at the studies, the amount of melatonin in your blood in the morning after taking slow release forms is far higher than in someone with normal daily melatonin production. Melatonin should be very low at wake-up time.
A lot of this “take 9 hours before” business may just be workarounds for the slow release forms. I take my MT just before going to sleep and get to sleep fine (which was not the case pre-melatonin).
While on the topic of jet lag, I found the following things help
a. Melatonin helps you get to sleep and perhaps helps reset the cycle.
b. Do not eat or consume any food or calorie containing drinks for 10-12 hours before your first breakfast in the new time zone. The first breakfast should be a good feed. This seems to have an almost magical effect in some people in resetting their time clocks.
c. Other very useful cues to the body/mind are, for day (warm, bright lights/sun, noisy), and for night (cooler, as dark as you can manage, quiet). Cover the christmas tree style lights on the hotel room appliances with tape. Turn the air-cond down. Use eye covers and/or ear plugs.
This matches my experience. Years ago I used 5mg or 10mg, which gave me weird dreams but also seemed to cause depression issues. Since then I’ve discovered that even 1mg pills are too much, and I use a pill cutter to quarter them, approximating your dose recommendation. Also timing is everything.
Rumour on the internet is that melatonin is metabolised into DMT, which is what makes you dream, and why exogenous melatonin causes weirder dreams. No idea whether anyone’s tried huge doses though.
Melatonin feels less effective in me these days, but it’s hard to honestly measure my own performance. And a consistent exercise schedule overwhelms everything else.
One of the weird things about melatonin is that in the US you can just buy it over the counter, but here in the UK you not only need a prescription, but GPs aren’t even allowed to prescribe it off their own bat without referring you to a specialist and getting permission from them.
My 8yo daughter takes it. We think she has delayed phase sleep disorder. Without melatonin, she doesn’t go to sleep until 10, 11, even 12 – even if she’s lying there in a dark room trying to go to sleep, with no book or electronic device (she doesn’t even own a tablet or phone) – and has trouble getting up at 8 for school. With it, she’s usually asleep by 9pm and has no trouble getting up for school.
She takes Circadin, which is slow-release, so in theory should avoid the problems Scott describes in paragraph 5 of having a peak at bedtime and waking five hours later. However, she sometimes does wake at 4 or 5am when she’s taken it. The GP said to double the dose from 2mg to 4mg to try to overcome this (apparentlythe GP is allowed to make that decision now she’s got the initial authoristion from the specialist to prescribe it at all), but maybe the studies mentioned here mean this isn’t such a good idea. Although because it’s slow-release I don’t think she has 4mg in her body at any time.
I’ve had no trouble ordering Melatonin from internet sites here in the UK, though I suppose I’ll have to start paying hefty international shipping rates if i want the 0.3mg dose varieties. I had no idea it was prescription only
I found this in the Spanish Amazon, which is 0.5 mg per pill (close enough, I guess). They allow non-prescription sales of up to 2mg, which is why there are a lot of options for 1 mg pills.
The UK seems to be pretty strict with what gets classed as prescription only (in my experience of this kind of thing).
That said, this appears to have more loopholes than stuff I’ve looked at before: it’s fine to buy it from other countries and ship it here.
I bought it once from amazon.de and then it disappeared because someone reminded them it is prescription only in most European countries. FML. I suppose I can order from a non-EU webshop, as private imports of small quantities of prescription only meds are generally allowed. Anyone can recommend a webshop?
I got that jolt awake with a smile, but what? If your cortisol is low the adrenaline gets high? And the other way around? Does also high cortisol lead to low adrenaline? One med for ADHD is Strattera which inhibits noradrenaline uptake. This might suggest ADHD may be caused by a noradrenaline deficiency. Partially at least.
Could high cortisol cause a noradrenaline deficiency? I mean, for example, kids who gut bullied a lot and thus spent a lot of time in a flight or fight reflex, could they have developed high cortisol, because of that, now noradrenaline and perhaps because of that, ADHD?
It appears to be available to ship to the UK from Amazon(.com).
Edit: On checking properly, the only one that is listed as available for UK shipping is actually for dogs. One of the comments (from the producer) says it’s fit for human consumption too…
Completely off topic: How many people get your screen name reference? My wifi had the same name for a while, much to the confusion of various guests. There was not a single person I’ve ran into that ever caught the reference.
https://www.vitaminexpress.org/de/melatonin-kaufen sells it in Germany. They claim it’s a food supplement, so they can sell it without prescription. Doesn’t make much sense to me, but hey whatever.
They also say that the pills are “sublingual” and are “absorped quickly via the oral mucosa”.
I suspect I’ve DPSD and don’t what that could mean about when to talk the pills.
But in Germany, it seems you can get it at your local drugstore? (0.5mg capsules)
Also, at Biovea I found liquid melatonin. I might try that for my son who has the typical problem of wanting to sleep late and get up late, but doesn’t like swallowing pills or capsules.
Thank you for that pointer! I dropped by at my local DM yesterday, and sure enough, there it was – 0.5mg melatonin. Who knows what cracks in the regulations that slipped through… I’ll give it a shot and see what happens.
Melatonin is available over the counter in many EU countries, such as Italy, and from Italian websites delivering anywhere in the EU. Although start with Robin’s website.
A few years ago as a depressed teenager I used to sleep ~2h a night, wake up at 6AM for school, sleep through 2/3 of my classes (that ended at 1PM), go back home, and sleep more until 5PM. Fun times.
I got into a really bizarre sleep pattern when I was in high school as well. I would sleep immediately after getting home from school, wake up at about 11PM, do my homework, and then play video games or something until it was time to go to school. Rinse and repeat. I did this for quite a while, apparently blissfully unaware of the havoc this would wreak on my circadian rhythms. It was nice though, I have to admit.
Brilliant! I was just telling my melatonin-chugging brother that I thought taking a sleep-signaling hormone at 4am wasn’t doing his sleep schedule any favors, but I doubt he paid me any heed. Now I have a much better, empirically-based thing to club him over the head with. And this is just really useful and interesting besides, especially since I have struggled with sleep issues for a long time. I will be sure to put all of this into practice.
Side note – MMTYWTK posts are some of my favorites on here, especially ones regarding health. Would always love to see more of them. Given the sheer amount of conflicting information regarding the topics, MMTYWTK posts on psychotherapy and/or vitamins/supplements/nootropics would be fantastic. (And no, I will not stop using that acronym.)
I don’t have much else to contribute, other than to be that guy and point out a typo: “your have to keep doing them”.
You either missed an open bracket or incorrectly included a close bracket in section 2: ” Lewy et al 2002)”
Also, section 6: “if you use melatonin the wrong way it will make things work”
Do you mean “worse”?
Is typo correction helpful or just annoying? I realise I don’t actually know if there’s a policy or rule of thumb on this. Sorry if it is annoying.
My problem (I am in my 50’s and I imagine it is an age thing) is that I get to sleep fine but I wake up every other hour and never feel really rested. I’m aware of how addictive sleeping pills are but I may take one once a month or so just to get a full night’s sleep. Not sure from the article if melatonin is much help here.
Anecdotal, but melatonin helps me with sleeping through the night. (early thirties)
Might help, might not. Melatonin isn’t addictive and it’s dirt cheap, so it’s worth a try.
Have you been tested for sleep apnea? Do you have chronic pain? Night sweats? Parasomnias? Do you share a bed with a family member or pet? Besides melatonin, you could try different heating/air-conditioning settings, white noise, earplugs, blackout shades, different mattresses or pillows, etc. etc. etc. All kinds of innocuous things can interfere with sleep.
Wow, thank you! That was exactly as much as I wanted to know about melatonin! I was taking 3mg chewables with the uneasy feeling that was too much. I’m going to switch products immediately.
I haven’t been officially diagnosed, but I’m pretty sure I have Delayed Phase Sleep Disorder. Even as a little kid (3-10 years old) I would lay awake in bed or play in my room, long, long past being put to bed by my parents. It got worse as a teenager. No matter how disciplined I was about going to bed early, I’d be alert until 5 AM, with my middle and high school starting at a (barbaric) 6:50 AM.
Day jobs as an adult? Misery, no matter what I did with timing, exercising, and diet.
I eventually settled on working full-time overnight (though it’s admittedly only been “jobs,” not “careers”), and am much more content for no longer fighting what my body wants to do. I sleep great during the day, although not without some adaptations.
In addition to the common wisdom tips about limiting caffeine and screen time before bed, here are my tips for sleeping well during the day (although it’s applicable to night, too):
1. The Goal is Total Darkness
Never let direct sunlight touch your skin right before or while you need to be asleep. Even the little specks that leak through the cracks of a closed mini-blind will send messages to wake your body up.
Thus: Fuck. Mini-blinds. Forever.
Instead, go for a combination of a light-blocking cellular shade mounted inside the window frame, and black-out curtains outside of it.
I recommend heavy-duty black-out curtains, ideally with velcro closures. I use Eclipse Thermaliner Blackout Panels, sometimes as liners, and sometimes as just white curtains. I mount them as close to the wall and ceiling as possible, to minimize ambient lighting seepage around the top and sides of the window. If you’re really committed, you can put a valance over the rod to prevent seepage entirely.
Ambient light is bad, too, as its impact even through closed eyelids can also keep you wakeful (or wake you). A good rule of thumb is that if you’re trying to sleep, it should be much too dark for you to read.
If you can’t modify your habitat for total darkness, the best sleep mask ever is the Bucky 40 Blinks Ultralight Sleep Mask. The eye covering is contoured so that there is no pressure on the eyelids whatsoever. You can freely open and close your eyes while wearing the mask.
2. The Goal is (Almost Total) Silence
Howard Leight Max Light disposable foam earplugs, and insert EXACTLY as directed (be very careful to gently wiggle the ear and slowly remove the plug when done. If the plug has formed a proper seal, yanking the plug out without first breaking the vacuum could injure your eardrum).
These earplugs are a technical miracle. You will be able to hear piercing sounds, like alarms, and also close-proximity human conversation (albeit both will be a little muffled), but won’t be able to hear ambient bothersome sounds like traffic, construction, neighbors’ voices, footsteps and TVs, rattling fans, etc. I once lived about 50 feet away from a major bus station hub and above a musician at the same time. These earplugs made it possible to sleep.
3. The Goal is to Never Be Bothered
Configure your phone so it won’t wake you up with trivial bullshit. Create a DND setting that mutes all alerts except for calls from whomever you’d want to be able to wake you in the event of an emergency. Make sure the relevant people know your schedule and not to call you (or knock on your door) for anything less than the kind of dire emergency they would want to be woken for themselves at 3 AM.
If you’re comfortable with doing so, set up auto-replies for text messaging and voicemail letting people know that you’re asleep.
This last part is actually the hardest; people can be surprisingly dumb about understanding what “I sleep during the day,” actually means.
I hope this is helpful for any fellow nocturnal readers, or anyone who’s having environmental issues with their sleep space!
I found that doubling up on window coverings worked well, a good-fitting polyester shade to block most of the light, and a heavy curtain over that to catch what seeps around the edges.
As a counterpoint, I bought that sleep mask years ago and I loathe it. A) It cuts painfully into my ears. B) IT consistently falls off; I never have it on when I wake up, which is the time I badly need light isolation.
(Anyone got a second recommendation?)
I use an Alaska Bear mask and find it very comfortable and unobtrusive (although the only things I have to compare it with are cheapo masks from airline amenity bags).
Having tried a variety of conformations of sleep masks, I think you had a product whose design didn’t fit your needs. Try this specific mask.
It has two straps, one below and one above the ears, so it can’t fall off in either direction.
You can wear it loose, so that the straps serve to keep the mask from falling off rather than keep it fixed in place. There should be no pressure from the straps when the mask is in neutral position, but you’ll feel a gentle tug if you try to slide it too far down or up.
The embedded cups also prevent pressure on the eyes, and silk is objectively the best fabric for sleep masks (hygienic, breathable, light, extra soft).
I’ve had the same problem with my old Tempur sleep mask. It was comfortably soft with lots of room for my eyes and had perfect light-blocking but the single strap was just annoying to use. I ordered a cheap double-strap sleep mask from AliExpress to test whether a double strap would work like I imagined without risking too much money. It did work and I use this mask now. There’s a slight gap around the nose that lets in a tiny amount of light which I find to be acceptable. There’s no cups to give space for your eyes like in the one Meister linked but the size of the mask is large enough that by spreading the mask vertically to its maximum the lines across which the straps pull will be on your forehead and cheekbones+nose and not across your eyes. However, although there’s no pressure on my eyes my eyelashes do make contact with the mask. If that is too irritating for you, this might not be comfortable. The best thing about this is the low price of course.
Once upon a time, I covered my windows with aluminum foil (attached with tape) to black them out and prevent sunlight from waking me up. It really worked well…
In my kids rooms we have yoga mats stapled to wood frames inside their windows and blackout curtains over top.
Just so we’re clear, the correct abbreviation (for the correct phrase) “Delayed Phase Sleep Disorder” is “DSPD?” At first I thought maybe it’s a typo, but both that phrasing of the term and that spelling of the abbreviation are used utterly consistently several times in the original post.
I messed up – correct phrase is “Delayed Sleep Phase Disorder”
Really interested to see this information. I pretty clearly have some kind of sleep disorder, hence why I am commenting on this thread at 4am. I went on the go to sleep after school schedule for high school and I’ve gravitated to night shift and flexible schedule jobs as an adult.
I’ve thought about giving melatonin a try, and the information here is a good starting place. However, I also feel a certain resistance to trying to change this part of myself. I feel more alive at night and get most of my best work done then. I’ve managed to stay on a more conventional schedule at various times and I felt like I was exerting enormous effort merely to trade my best hours for shuffling around like a zombie in the morning. Unless it is absolutely required for work or something, being awake in the morning just doesn’t seem worth the trade off.
I think I also have some resentment about being forced into day schedules. It seems like there is an almost moral dimension to how people think about waking times – we have Ben Franklin with the whole “early to bed, early to rise” thing and it seems to bleed into a lot of thinking about work ethic. I wonder how much this is a factor in continuing to enforce early mornings in school and at work. I’ve certainly experienced people assuming that sleeping at noon = laziness without any consideration for how much I might have worked the night before. I’ve yet to hear of someone being called lazy for going to bed early. The link between getting up early and work ethic might have made some sense in an earlier time with more agricultural jobs and less artificial light, but I’m really annoyed that I have to keep making the case that modern society needs night shift workers and I too can be a functional and productive citizen whether I adjust my sleep schedule or not.
Hey thanks for posting this. I have decent control of my sleep and do the whole early to bed/early to rise thing, and only just realised after reading your post I’ve started looking down on people who go to sleep at late/abnormal hours.
Thanks for helping me become more aware of this!
It’s great to hear that my comment brought this to your attention, and that you are open to thinking differently.
There absolutely are lazy people who sleep all day, but the tell is all the other lazy-person things they do and not just the hours when they are sleeping. At the same time there are people who make a great performance of productivity by being up early and don’t actually get much accomplished.
Here is another misunderstanding for the list of totally obvious things some people have somehow failed to understand.
I’ve so far thought incorrectly that sleep phase = circadian rhythm and all sleep phase disorders are about having a rhythm longer or shorter than 24h. I’ve misunderstood delayed sleep phase as >24h rhythm and advanced sleep phase as <24h. I thought you got sleepy with darkness and awoke with light regardless of your rhythm length and that this just pushed you to align your rhythm with sunrise and sunset.
I thought my major trouble falling asleep when I was depressed and somewhat lesser trouble before and after were problems with my mechanism of falling asleep, not when I was trying to do it. It never occurred to me to that I might've slept just fine, if I just went to bed at 3-4AM like I felt like doing.
So, now I understand that actually sleep phase disorder is when you get sleepy out of phase with your exposure to light. Your circadian rhythm is a normal 24h but the sleep timing your body is trying to produce is not congruent with the timing of light and dark you get exposed to. That is, you get sleepy long after it's become dark or long before.
I don't really know for sure what my problem with sleep is as I've brutishly forced my sleep to conform with my desired schedule using a somewhat firm pharmacological fist. At present I'm treating myself with a low dose of 3,7mg (1/4 of 15mg) mirtazapine and what I now consider a high dose of 2mg melatonin every day when I go to bed at 21:30 which is 30min before I begin trying to fall asleep. I have no idea how the mirtazapine is interacting with the melatonin but my subjective feeling is that neither works as well alone in allowing me to control what time I fall asleep. It's possible I've stumbled onto a combo that works well for me personally to effectively take the reins off my body regarding when it falls asleep. The problem I still have is that my sleep is inefficient and I feel like sleeping until 8:00, which is 10h after 22:00, is necessary. According to the SleepRate app I use with my Polar H10 heart monitor, I typically sleep 80-85% of my time spent trying to sleep. So that translates to just over 8h of actual sleep per night. I wake up to go pee at least twice every night. At this point, I may have followed the urge without considering whether I actually it's necessary that it these these wakeups that happen like clockwork at 23-00, 2-3 and 4-5 have been engraved into my brain. When I drink less water I still mostly wake up at these times but just conclude I don't feel like I need to pee.
I now suspect that I've got delayed sleep phase and forcing myself to sleep at these normalish times is what makes me sleep inefficiently. The idea of feeling fully rested every day while spending 9h instead of 10h for the whole procedure of sleep is tempting. But my experience with depression has given me this fear of losing control of my sleep that makes it hard to let go of my currently working solution that's given me consistent control for a few years now.
I commented above about having delayed sleep, and how I’m a little resistant to seriously trying to change it. The reason I don’t say I have insomnia is because like you suspect, if I sleep when my body is ready I get excellent sleep. Being able to sleep well and wake up refreshed is a wonderful thing and I have currently chosen to fight for a schedule that allows that rather than fight with my body over when I sleep.
On the other hand, I am impressed by your discipline at sticking to a schedule. I recognize there are things I miss out on by not being awake in the mornings and if I could find a system that really worked I might give it a try. I have had some bouts with depression and it was hard to tell what was my natural sleeping pattern and what was staying in bed all the time due to being depressed, so I don’t think your concern there is misplaced by any means.
“There are some weird pathways leading from the eyes to the nucleus governing circadian rhythm that seem independent of any other kind of vision;”
I recently read about this. In some animals the corresponding structure is almost literally a third eye: https://en.wikipedia.org/wiki/Parietal_eye
On rare occasions, when I take melatonin and also go to bed a few hours before my natural bedtime, I wake up at 3-4am. I think this might be related to biphasic sleep. If I stay in bed when this happens, I’ll eventually fall back asleep, but if I get up and do anything I won’t be able to get back to sleep.
When I first started taking melatonin, both 1mg and 3mg doses helped me fall asleep, but on 3mg I woke up groggy and with a slight headache. Later, after taking 1mg each night for several months and starting Vyvanse, I felt like I needed to take 3mg in order for it to work at all. But I could have been imagining it.
A good alternative to f.lux on Windows 10 is Night Light, which comes automatically installed these days. A good alternative to f.lux in general is redshift, which is like f.lux but free software.
Given that we spend ever increasing amounts of time indoors, exposing ourselves to artificial light, is circadian rhythm disturbance being investigated as a potential causative factor for increases in psychiatric disease? I know it’s mainly changes in diagnosis, but given how inconsistent diagnosis tends to be, I’m not sure we can really tell if there are subtle factors that affect incidence.
Maybe starting with a causal factor that we know changed is a smarter approach. Probably there would be all kinds of natural experiments in the exposure available too (electrification of rural areas, new streetlights, a new shift system, new employment underground ..?).
I guess we know shift workers are pretty fucked, but apart from that I don’t know any literature. Glad for any pointers.
When I tried taking melatonin, the crazy dreams were so intense that I would actually wake up repeatedly through the night from them. Which kind of defeats the purpose.
I was lucky to discover melatonin many years ago, when the common pill size was 300ug. (0.3) Results of my experimentation were: you have to take the amount that will be “burned off” by morning, or else you’ll still be sleepy in the morning and it looks like it’s “not working”. For me, that’s 2 pills (600ug) for the usual 6-7 hours I can squeeze in, or 3 (900ug) if I actually get the chance for 8+ hours. Anything more is too much. One pill will put me right out, but if I get up to pee…too bad, that might be the end of it and it’s sleepover-party-syndrome time. 😉 Taking any amount, any time other than “right before bed”, means…I will be asleep (or at least mentally nonfunctional) within 15mins. The only thing worse is Benadryl. (!)
I’m still voting for any candidate who will abolish the standard 8-5 workday. 😉 Many of us are NOT meant to be awake from 6am until 11pm, and we’re not performing anywhere near peak ability…not to mention, how to get anything done when everything is closed as soon as you’re off work, because all the workers at the places you need to go are ALSO now off-work. The US work schedule is terrible, imo.
I have been taking around 3mg a day for about 28 years. At first the melatonin gave me vivid dreams that caused me to wake up, but this has long since stopped. I take melatonin about 20 minutes before bed and I perceive that it makes me drowsy. The problem I took it for was that I would “naturally” stay awake until dawn and then sleep for eight hours. I perceive that melatonin has made a huge positive difference in my ability to function in the world.
Yep. Same here…it lets a night owl function in a Day World. 😉 My natural bedtime is 5-6am. Too bad that’s when I need to get up!
I’ve been taking 0.5mg for about a year and a half, it’s been a dramatic decrease in the amount of time I take to fall asleep, the consistency of when I fall asleep, and the likelihood of me sleeping through the night. My natural sleep cycle is like 2am-10am, with melatonin I’ve pulled that back to midnight-8am pretty easily.
If you want other things to improve your sleep, also consider sleeping with earplugs, if there’s noise where you sleep (if you’re in any city, for example, or have any roommates). A memory foam mattress also helped me a lot, although they start around $800 for good ones, so try the cheap stuff first.
Great guide – thank you! I have hopefully quick questions:
1. Are there any research-based dosage guidelines for children (say ages 3-13)? Alternatively, is there perhaps any change to the dosage guideline by weight?
2. How should I interpret the fact that Labdoor did not test Nootropics’ brand of melatonin? In other words, on what basis can you recommend the Nootropics brand? (I’ve never read this site before so pardon my innocence here…)
Thank you!
I don’t know enough about children to be comfortable saying anything about them, and I’m not sure which guidelines to trust there.
I trust ND because they have a good reputation within the community and other (scattered) purity tests have always come back good. I think LabDoor has tested some of their other stuff with good results.
I assume that means I also don’t get advice about how best to dose my baby so he can sleep through the night.
Goddammit.
most child brand melatonin is 0.3 mg! just so happens to be the only way you can get 0.3 mg tablets at the moment.
Can I also beg for an answer to the children question? I’m hoping to use melatonin soon to reduce the jet lag caused by an international family vacation, and it would be wonderful if the whole family could do the same.
Edit – I should have refreshed the page before commenting. Thanks!
Gwern talks a bit about using melatonin on children – he’s not a doctor, but he does cite a few studies. There hasn’t been much done, but what has been done suggests the safety for children is similar to that of adults, i.e. unlikely to cause any bad effects and it’s not going to cause any effects that don’t go away when you stop taking it.
Ask your actual doctor, I guess? They might know.
My personal anecdata: I take melatonin about 2-3 times a week. I don’t have serious sleep problems – I’m just naturally a little bit of a night owl, and on some nights I want to be able to fall asleep around 9 or 10pm instead of 11+.
I used to bite off a piece of a chewable 0.5 mg pill (Trader Joe’s brand) – 1/4 to 3/4 of a pill depending on how early I was going to bed. A few months ago I switched to the 0.3 mg Nootropics Depot version (which is not divisible – I fall back on the TJ brand if I want a very small dose). My dreams were often particularly vivid (but I wouldn’t have said crazy/weird) on nights when I had half or more of a chewable pill. With the ND 0.3 mg pills, I occasionally have a vivid dream, but much less frequently. Maybe the dosing in the TJ pills was inconsistent? Even when I had what should have been under 0.3 mg via the TJ pills, I had more vivid dreams than I get with the ND pills.
I do frequently wake up refreshed about 6 hours after I take the pills. Slightly larger/smaller doses move this time later/earlier, and also increase/decrease the feeling of suddenly being awake. I usually get up to pee and have no trouble falling back asleep afterwards.
Tangent: As a teenager I had a typical teenage sleep cycle. In college I felt that my natural circadian rhythm was 25-26 hours, but maybe I was just confused by my body wanting to go to bed at like 3AM. Anyway, I had two terms where my schedule was very amenable to six ~28-hour days per week (I think my day ending at 4pm Wednesday was 30 hours, another was 26, most were 28), which I did happily.
One factor that has likely influenced the available and recommended doses is that MIT had a recently expired patent on low-dose (less than 1 mg) melatonin. This has been cited as the reason 1mg was the smallest dose available for some time.
gwern also wrote an extensive post on melatonin that may be of interest as further reading.
I took a melatonin last night so I could get to sleep early and wake up early.
And of course I spent the whole night dealing with crazy vivid horrifying dreams. The stuff my brain comes up with on that shit is nuts. God damnit melatonin, I just wanted to wake up early, not go on a fucking vision quest.
Wait, so sleep is not supposed to be a horrifying vision quest? I must be doing something wrong.
I love having nightmares. I enjoy telling my brain in the morning, “this is why it makes sense to prefer the real world.”
I hate having pleasant dreams for the same reason.
Looks like of the rated products (and aside from the liquids), the GNC 1mg delivers closest to the recommended dose at 0.89mg. It’s a lozenge; if it can be split in half it would be really close, and widely available in the US.
Interesting!
So as someone who experiences SAD and was also a shift worker on the DuPont Schedule for several years I have plenty on anecdotal information on sleep scheduling. Interestingly, my SAD was less pronounced when I was on shift, possibly because I would rather quickly get up and go to work where it was continually well-lit, and stay there for 12 hours. When I switched to a normal schedule where I spent more time outdoors it became much worse.
My most fun anecdotal fact from that time is that when driving home in the summer around sunrise, the worst thing was to actually see the sun. The ambient light was tolerable, but one glimpse of the sun itself would ruin any chance of getting to sleep cleanly. I would literally hold my hand over the sun as it rose to avoid seeing it directly.
I’m a fan of Trader Joe’s peppermint-flavored 0.5mg chewables: https://www.amazon.com/dp/B004OLL190
I like those because I can bite off a smaller piece to modulate my dose (the earlier I’m going to sleep, the more I take), but I have more vivid dreams with TJ’s pills than I do with NootropicDepot’s (even when I’m only having half a TJ pill and should have a smaller dose than the ND pill). Not sure what’s going on there. Though it is possible that I just stopped having the vivid dreams over time, about when I switched over to the ND version.
My melatonin observations:
1) At one time I was taking a very low dose of 0.25mg. This was super effective at getting me to sleep. Over time I got lazy about cutting pills into tiny pieces and started taking 3mg and later 5mg that I bought on amazon. These were equally effective at getting me to sleep (I don’t think they were _more_ effective) but they had a nasty side effect of making me super groggy in the morning. It seems to me there’s no point in going to sleep earlier if I’m going to be extra tired in the morning, so I’ve been lowering my dose over time. I’m currently taking a 1mg supplement, and I think this is still too much.
For context: I’ve never had significant trouble falling asleep, and I generally keep an early-ish schedule. Left to my own devices, I fall asleep between 23:00 and 01:00 and wake up between 06:00 and 08:00
2) 100% confirm the crazy dreams thing. My dreams are much more vivid when I’m taking melatonin. I wouldn’t say they’re particularly crazy, or negative, or whatever. They’re just more vivid.
3) I typically take melatonin 1-2 hours before going to sleep. If I take it at, say, 20:30, then I’ll almost certainly be asleep by 23:00. If I’m not in bed, sleeping by then, I will be incredibly tired and a little bit loopy.
4) Paradoxically, if I somehow power through that incredible sleepiness, and am still awake ~4+ hours after taking melatonin, it makes it harder for me to get a good night’s sleep. I still fall asleep nearly instantly, but instead of getting a good rest, I end up tossing and turning and waking up repeatedly at night. This effect appears to be stronger with higher doses. I don’t know how to reconcile this with the recommendation in this post to take it ~5 hrs before bed.
5) I take melatonin every night. I used to worry that this is bad, like my body would adjust to it and then it would be impossible to fall asleep without it. But this hasn’t happened yet, and we’re like a year and counting since the last time I took a melatonin break.
What’s the difference between time-release and normal melatonin? I’ve been taking the former, 1mg, on the basis of bro-science reasoning – my issue is less falling asleep, and more waking up in the night to go to the washroom and then not being able to get back to sleep.
What are the possible side effects?
Years ago, I was a on again off again smoker. I’d smoke a pack a day, roughly 6mo out every year, quitting and starting over (with each quitting being more difficult than before). The introduction of electronic devices made “quitting” the burning kind of tobacco very easy, but putting away the electronic stuff just as hard, and picking it up even easier (I do a lot of cycling. I can immediately tell the effects of the burning kind of smoking. I can’t tell the effects of electronic based nicotine delivery. That makes it very easy to convince myself that this isn’t really bad for me, or at least no too bad). The reason I bring this up is that one reliable side effect of nicotine withdrawal is insomnia. Typically lasts 2-3 days, and its a real drag. When I mentioned this to my doctor, she said to go get melatonin. I mentioned that to my wife who told me of people who managed to completely screw up their sleep cycles in terrible ways. Maybe it was nothing, maybe it had something to do with over the counter doses being far too high. For 2-3 days, I’d rather not take the chance. But I also prefer to sleep normal, all the time.
Thank you for this, I have struggled with sleep problems for years and even visited a sleep specialist. This provided more info than I have gotten so far!
Looks like the NootropicsDepot is not actually available on Amazon, but apparently you can get it direct from Nootropics.
Excellent article, Scott. Here are some additional sources of information for those with circadian problems.
The Circadian Sleep Disorders Network is a patient support and advocacy organization, incorporated in the US as a 501c3 organization, but with board members from many countries. Our medical advisory board includes many of the top names in the field. The web site has an extensive bibliography.
We are creating a patient registry for circadian disorders. If you have such a condition, please answer our survey which can be done anonymously.
There is also the DSPS blog where I have written a post specifically on the use of low dose melatonin.
Scott may be interested in this case of psychiatric misdiagnosis of a child with N24, which happens too often.
There is also the Non-24-Hour Sleep-Wake Disorder Support Group on Facebook. We have advocated for the chronobiotic use of melatonin (low doses around 6 hours before sleep) for most persons. There is a wide range of responsiveness to melatonin (partly due to a 28-fold variation in metabolism. The group is open to anyone who thinks they have N24 or has a child with the condition. It is a closed group and we keep it polite and generally science-based.
There are also a couple of well-run Facebook groups, here and here, on DSPS.
There is a Nite Owl mailing list focusing on circadian disorders.
I have co-authored, along with Dr Katherine Sharkey of Brown, a report on N24 for the National Organization of Rare Disorders, with particular emphasis on its biological underpinnings.
Interesting fact: If you isolate cells, for example fibroblasts (connective tissue cells), from patients with N24 and grow them in culture, the cell cultures also show an abnormally long circadian cycle.
Clearly these lazy shiftless cells lack a proper work ethic and require a stiff dose of tough love. Give them an ultimatum: 30 days to get a job and move out of their parent’s Petri dish, or you’ll put their stuff out on the curb and change the locks—no excuses. That’ll whip ’em into shape.
Scott, if you think that you, personally, have a larger response to melatonin than other people, maybe you should use an even smaller dose. Of course, if you’re just experimenting for fun, maybe you shouldn’t bother at all, but if you ever actually need it (eg, for jet lag), you should try the smaller dose.
If melatonin makes you wake up at 4am, have you ever tried extended release?
Has there been any research about children? I know someone who gives melatonin daily to her kids. I wonder if there are any long term side effects.
There have been a number of small N case series and reports. The largest study followed 51 Dutch children treated with melatonin for an average of 3.1 years and has not found any long-term side effects. This is reassuring but at the same time that is a small group.
The motive for the Dutch study was particularly to find an effect on pubertal development since melatonin does have an effect on sexual development in some mammals, but those mammals tend to be those with seasonal breeding patterns.
It is probably prudent to reserve melatonin for children whose sleep problems cause significant impairment and to use the lowest effective dose. Low doses given early in the evening mimic the normal physiological levels of melatonin, but at an earlier time. Long term side effects from such levels are unlikely. The use of high hypnotic doses at bedtime is a bit more troubling although the Dutch study did not find problems even with high doses.
I am not a doctor, but IIRC you can build a tolerance to caffeine relatively quickly (this is why long-term coffee users need multiple cups of coffee to get the same charge as one cup used to give them – you wake up essentially caffeine deprived and need caffeine to get back to normal). You can also lose tolerance in the same way – slowly reduce your dose of caffeine (slowly or you’ll get headaches) over a period of weeks. I can’t speak to exactly how much to reduce each day as I’ve never had to do this, but the equivalent of one less cup of coffee a week should be comfortable.
Or, cold-turkey. For me, it was just a few days of feeling shitty. YMMV
Years ago I found that dosing roughly following an exponential decay model helped me manage caffeine withdrawal pretty comfortably. I can’t remember exactly how I did it, but it was something like take 25% off whatever daily dose I started at, wait 3-5 days, then take another 25% off, and so on, until I was down to a negligible dose.
Gwern has a magisterial article on melatonin, with largely the same conclusions: https://www.gwern.net/Melatonin
I’ve been using liquid melatonin since it’s the only thing available from my local drugstores that lets me take less than 1 mg at a time. (In particular, Finest Nutrition liquid melatonin, which has 1 mg per full dropper; I try to take about 1/3-1/2 of that each time. Though after reading this and also after noting that going down to a target of 0.3 mg per dose seems to have maybe coincided with me having more trouble falling asleep, I might try increasing this (my issue is something between delayed phase and non-24-hour, I guess, hard to tell because I’ve been sleep deprived for a really long time).)
The linked Labdoor list has three liquid melatonins, but they all have higher doses per full dropper:
– NutritionWorks (84.3 score) – 3.3 mg per 2 droppers (1.65 mg per dropper)
– NOW Foods (84.2) – 3.54 mg per dropper
– Solgar (82.4) – 7.91 mg (!) per mL (which I expect is the dropper size, as mine is)
In the past I’ve definitely noticed melatonin from the drugstore working to make me sleepier (not immediately, though, but closer to my bedtime – I take it 5 hours before, might try 6 or 7 hours before based on this post). I’m not sure if it’s working currently and now I’m wondering if I picked up a different brand than before without noticing (though there are also other possible explanations, like me being more depressed recently or, on the other hand, me finally beginning to catch up on sleep after many years’ sleep deprivation).
Wait, what exactly is the problem? Waking up feeling refreshed and bright-eyed and smiley sounds pretty spiffy to me, even if it’s not the exact time of day you’re accustomed to being awake. I’d be interested in hearing more about when and how this turns into a negative; does the early waking time combined with the shorter sleep phase mean you start getting drowsy at 5 PM the next day? Can this effect be remedied by taking the protocol for “move my sleep schedule to later in the day” = another small dose of melatonin at 4 AM when you wake up?
I vaguely recall this being sort of the case with me the last time I tried a melatonin regimen, but lately I’ve been waking up way too late (almost making me late for work), and also feeling extremely drowsy throughout the day. This article is well-timed for me; I’m now strongly considering another trial with melatonin, this time using a dose as close as I can get to 0.3 mg (though dividing tiny pills into tenths or thirtieths sounds really hard).
I’m actually hopeful that I can produce a result like waking up at 4 or 5 AM consistently; I’ve found that if I have free time before work, I spend it on exercise and meal prep, whereas if I have free time after work, I spend it on video games, shopping, and eat at restaurants.
I have a non-24 hour sleep disorder and I’ve also started taking melatonin recently (as in, maybe 4 months ago?), at the 10mg dose. I have actually found it extremely effective to take it about 30 minutes before I go to bed, knocks me right out with no negative side effects that I have noticed at all.
But based on this, I ordered the .3 mg version to see if I can get the same effect without the potential downsides.
> This model also explains the otherwise confusing tendency of some SAD sufferers to get depressed in the summer.
Thanks for being the first person to point that out (to me) that this isn’t unknown. Always thought that is strange.
So my problem isn’t getting to sleep, it’s staying asleep long enough. I get tired at a reasonable time of night; I go to bed and get to sleep reasonably quickly; I snap awake when the sun rises, be that 5 AM or 7.
(Yes, I know what blackout curtains are. No, they don’t help at all; black out curtains mean that it’s dim, but it’s still hugely obvious that the sun went up. If it is bright enough to read, which it is from light around blackout curtains, I will wake up. In previous living situations I’ve physically boarded up windows or covered them with aluminum foil (yes, really. I look exactly as crazy to people who see my bedroom as you think I do.) That helps, but even then cracks around doors or whatever mean I don’t sleep in well at all.)
Given that this was a sleep problem that had something to do with a circadian rhythm, I thought melatonin would help. Knowing that normal pills were “too big” I cut them in half (so I take 1.5mg, still way too much, thanks for the heads up on that!) and take them ~30 minutes before bed (wow, that’s way later than I should, again, thanks for the heads up!) I’ve done this consistently for ~5 years or so; it seems to help a bit, but I still don’t sleep well enough.
Since I can’t go to bed at 8 PM without destroying the rest of my life (see a previous OT for this) I’m really hoping for a better solution. Any other advice? Is smarter melatonin use a good idea here? Are there other pharmacological interventions worth considering, or do I need to build a hermetically sealed sleep coffin in my new apartment (since I can’t block the window…)
What are some of the common side effects of melatonin ? How does it affect fat people with high blood pressure, especially if they have to take a pill every day to keep their fat blood pressure in check ? Asking for, uh, a friend. Yeah.
I take melatonin almost daily, 1-2mg right before bedtime if I’m not feeling too tired but want to sleep. I find that I reach peak tiredness around 20-40 minutes after taking melatonin, and that if I stay up an hour after taking it I have a much harder time falling asleep.
Is this completely out of line with consensus recommendations and observations? Should I be taking it hours earlier?
I think the routine and mental cue of taking it right before sleep might create a placebo effect even more powerful than the melatonin’s true effect. Taking melatonin helps me not procrastinate going to sleep by watching another Netflix episode, instead forcing me to fall asleep within the hour. If this placebo effect is widespread, taking melatonin directly before bed might prove more effective than taking it hours earlier.
Could melatonin have 5-HT2 receptor activity? This would explain the vivid dreams, and the structure works.
One of the odder things about melatonin is its legal status. In America the FDA classifies it as a dietary supplement, not a medicine, which means it needs to meet the much less strict regulations around foods and can be produced by essentially anyone without prior approval.
Meanwhile in several European countries, it’s a prescription medicine. I wouldn’t be surprised if it’s a full controlled substance somewhere.
Neurologist here. I recommend melatonin very frequently for sleep induction, given how safe and ubiquitous it is.
I usually tell people to start with 3-5 mg and increase until A. they consistently get what they want out of it, or, B. they wake up too sleepy in the morning, in which case they should reduce their dose. This is based on my own experience (recommending it, and taking it), the experience of the neurologists who trained me, and the general recommendations of the sleep doctors with whom I collaborate.
None of my patients has ever reported waking up too early – not once. The simplest explanation for the waking-up-too-early phenomenon is not some arcane neurologic phenomenon, but something akin to “Your dose wore off too early.” The fact that you can take enough melatonin that you feel sleepy in the morning is further evidence thereof.
If I don’t take melatonin, I don’t wake up early, so I’m not sure how this can just be a dose wearing off.
Yes but if I or one of my patients takes melatonin at a higher dose than you, I/they don’t wake up early, either. So my polyanecdata directly contradict yours.
We know that insomniacs also have trouble with waking up earlier than they wanted to. In identifying this early-waking-with-melatonin phenomenon, we may have identified some people who are waking up early because of their insomnia, for which they have given themselves an insufficient dose of melatonin. And in doing so, we are comparing “I had insomnia, I took a tiny dose of melatonin, and still woke up early” to “I didn’t have insomnia, I didn’t take melatonin, and I didn’t wake up early.” Not a valid comparison.
Furthermore, the half-life of melatonin is about an hour. From log{2}(3 mg / 0.3 mg), we know that a 3 mg dose ought to last 3-4 half-lives longer than a 0.3 mg dose, or, 3-4 hours. A 0.3 mg dose decays to subhypnotic levels by 04:00. Therefore, a 3 mg dose should decay to subhypnotic levels by about 07:00 or 08:00. That corresponds rather perfectly to my
polyanecdataclinical observations.Taken together, the full set of effects seems to be :
– Insomnia + 0 mg melatonin : fully disordered sleep
– Insomnia + 0.3 mg melatonin : go to sleep but wake up earlier than you intended
– Insomnia + 3-5 mg melatonin : go to sleep and wake up at a normal time feeling good
– Insomnia + [too much] mg melatonin : go to sleep and wake up at a normal time but feeling overly sleepy.
That looks exactly like a dose-dependent effect spectrum, rather than some unusual effect exerted by low-dose melatonin.
—
Here’s the kicker : if arguendo the waking early is an unusual neuromodulatory effect that a suprahomeopathic amount of melatonin exerts, and you don’t desire that effect, why not just take the dose that doesn’t exert that effect?
Personally I would love to wake up fully-rested at 04:00. That sounds absolutely fantastic.
Somewhat unrelated to melatonin per se but all this talk about vivid dreams raises something I’ve been curious about for a while: as far as I can tell, I don’t seem to dream under normal circumstances. When I do dream, it’s normally either when I’m sick with a temperature well in excess of normal, or if I’m influenced by some kind of chemical (codeine is the most likely culprit, although excessive alcohol or pain meds have also triggered dreams). This is uncommon, however, and I’d estimate that I dream maybe one or two times a year.
When I do dream, it doesn’t quite seem to have the impact that other people use to describe their dreams. I’m always in a situation that’s perfectly normal (at work, visiting my family, back in college) I’m always feel like I’m under some kind of low-level stress (report needs to get done or something) and I’m almost always aware that I’m dreaming. Again though, this happens at most once or twice a year.
As far as I know, I’ve always been like this; talking to my parents they don’t ever remember me talking about dreams as a kid. Does anyone have any insight into why someone just wouldn’t dream?
I’ve heard/read that everyone dreams, and that people who claim to not dream simply don’t remember their dreams. I have no idea if this is true or even how one would attempt to verify it. It used to be very rare for me to dream (or to remember my dreams, as the case may be), but since I started taking melatonin it’s become much more frequent (probably almost daily).
yeah, that tends to be the reply I hear most frequently when I talk about never seeming to dream. On the one hand, I suppose it could just be that my ability to remember dreams is significantly below normal, but on the other hand I feel like the whole “it happens, but you don’t remember it” argument could be used to justify any unlikely entirely subjective experience.
Even accepting it’s true, it just raises the question up one meta-level to “why would someone as a rule not remember their dreams?”
I frequently remember the experience of having just awoken, thinking “that was a really cool dream and I hope I remember it for more than fifteen minutes”, and nothing more. With deliberate effort, I can pin down key details of a dream as long-term memories-of-memories.
When I was in high school, an AP Psychology assignment was to sleep with a notepad next to our bed, and make a conscious effort to awaken after each of our dreams and record them. I was successful, but ever since (for the last 15 years) I’ve awoken much, much more frequently after I dream. Usually I get back to sleep, but it’s certainly lowered my perceived sleep quality.
I have one or two stories of sudden mental alterations from innocent tinkering:
One day when I was a kid, I remember I was at a fair with a friend, I either (I forget which, but it was one of these two, or something very much like it), A. simply realised that other people had an internal sense of time (I could never guess without a clock), or B. my friend explicitly told me that the skill was easy, when I was all like ‘woah dude..’ how the hell that’s magic, and, -in basically the same spirit as people will try and see whether they have psychic powers-, I tried then and there to conjure up such an ability in myself, and well-it-totally-worked, -since then I have a vague sense of time elapsed, so something must now be ticking away in the back of my head. I haven’t tested it recently, but when I tried I could even decide when exactly I wanted to wake up without an alarm, though not quite reliably enough to forego said alarm.
I’d take it back if I could though, because I remember perceiving (in the same way/at the same level that I found/coalesced the trick) that it made my mind that tiny bit more rigid, like I’ve reserved a tiny corner of my mind for that purpose, so it’s no longer free (or as free) for other things. (Maybe I will someday, -if one way why not the other?)
_
I’ll mention the two other instances I remember off the top of my head:
1. somewhat similiar experience with slowing down my perception of time: It was the day of some passing of a year or another, perhaps a birthday, and I remember thinking how this time last year could have been just yesterday, how fast everything seemed to pass, all the days between now and then seemed blurred together in a single indistinct haze, like I might as well have just stepped from then to now with nothing in between, -and I had the thought that if this kept up I’d be old before I knew it. –So I (in the same morbidly-curious, expecting-nothing, spirit) tried to find what makes “time fly” when you’re having fun or otherwise, and tweak it, and something did change.
2. One day on the way to school, I forget what exactly I was thinking or what I was doing, except that I was tinkering/poking at things inside my own head, -and I must have pulled on the wrong thread because it was like an evil spirit attacked me, complete with ‘schizophrenic whispers’ (no idea how representative/accurate this depiction is in general), and stayed with me for quite a while.–It turns out that my uncle is full blown ‘in a facility’ schizophrenic, though he was clearly set off by definite instances and in particular a definite instance of trauma. -So I wonder if this could happen to anybody pulling on imaginary threads like a cat with ball of string, or if it might be a reflection of some latent capacity for such conditions, or thirdly whether perhaps the action itself could represent a/the (if there is one) genetically linked schizophrenia risk rather than the result- e.g. cat-killing or morbid curiosity, interest in vague indistinct meanings one doesn’t understand, (though I certainly didn’t attribute any great significance to them)
I also wonder how much of the ‘occult’ idea is people (especially religious-raised) fucking around with similiar things unaware of a mainstream framework to describe them and seizing upon nonsense in its absence as the Hidden Truth, kind of like how someone might down a bottle of vodka (don’t do this) because their parents or society tried to make them frightened of beer and “fool me once…”
How does this square away with the idea that humans before electric lighting slept in two parts. The so-called “Segmented Sleep” schedule? Go to sleep for ~4 hours, wake up in the middle of the night and do things (diary, watch the moon… procreate, etc) , then go to sleep for another 4 hours.
If this is the natural cycle of humans, the chemical pathways would need to have some sort of trigger to wake up when you’re half-way rested and be active for an hour or two, and then feel sleepy enough to fall back asleep.
How much credence is there to this pattern of sleep being the ‘default’ for humans? It’s obviously been done on wide scales. But is it driven by biology, or is it just another culturally driven sleep schedule? If natural – could sleeping disorders that cause you to stay awake, tossing and turning, be the screw up of a more delicate, complicated system that’s trying to make you semi-active for a few hours before falling back asleep?
It sounded really odd to me that the standard melatonin doses sold at drugstores is so much larger than the dose in which it is the most effective.
My first guess was that people purchase melatonin based on the intuition that higher doses are more effective so this incentivized drugstores to sell higher doses, and this process got a little carried away because of the (apparent) relative lack of bad side effects of large doses and the lack of regulation on it.
Googling a bit I found something about there being a “MIT patent” of dosages up to 1mg but I found conflicting reports about the patent being expired, and I also don’t know anything about patent law but something sounds funny about patenting a drug only up to a certain dosage. And in any case this doesn’t seem to tell the whole story since drugstores could have stopped say at 2mg.
Any more ideas about how the large drugstore doses came to be?
Do you know of any studies about melatonin for autistics? I have two autistic boys (ages 3 and 6) who won’t sleep at night without it. I’ve been giving them about 2.5mg just before bed for years. It seems to work, but I have no idea if these other study results generalize to autistics or not.
I’ve been a night owl since I was teenager, and I’m now approaching 30. I work in software so luckily I don’t have to come into work very early, but my natural inclination would be to sleep until noon every day, which is not really acceptable even in this industry. As such, I’ve been using melatonin for years to help get to sleep earlier. I still have trouble waking up as early as I’d like, and I’m still tired in the morning and throughout the day, but the melatonin does make it much easier for me to get to bed “on time.” The dose I take is 3-5mg, so perhaps that’s part of the reason I’m still tired during the day; I shall try taking a lower dose and seeing if it is still effective.
A local sleep specialist whom I saw a couple years back recommended taking it 3 hours before I went to bed. This doesn’t match the studies you linked, but I’ve found that timing to be pretty effective. Before seeing him, I was taking the melatonin immediately before going to sleep and I did not find it very effective.
I have found that my dreams are a lot more vivid when I take melatonin, or at least I’m more likely to remember them. Before I started taking melatonin, I almost never remembered my dreams. They can be pretty weird, but are’t dreams always weird?
For those who know, this is is obvious, but I walked in ignorance for decades:
There are cheap ($5 and up) and effective pill cutters that will easily cut any pill in half, and with some luck also let you keep going on to quarters etc. Check your local drugstore and amazon.com.
(This is to get your store bough melatonin pills closer to the 0.3 mg dosage, in case you’re to tired to make that mental leap right now)
Oh man, thanks for this Scott. I’ve been using low-dose melatonin for years to help me adjust my sleep schedule when it occasionally drifts to be really late. But I was always taking it around an hour before going to sleep, sometimes less. As you said, using the gun as a club.
Tonight I tried your suggestion and took it in the evening just after getting home from work, and now it’s 10:30 and I am beautifully drowsy and ready to drift off, whereas earlier this week I was only feeling like this around midnight. If this continues to work I should be able to get a lot better control over my circadian rhythms.
So thanks a lot for this. It means a lot that you’re able to distill this dense academic knowledge for a lay audience.
I keel over and sleep soundly around 9PM and get up at 4AM. For the record I think this is the best of all possible sleep cycles; nobody gets anything productive done after 9 anyway and getting 4 hours head-start on the world every day is great.
However, if you want a data point for your missing research, I’ll happily take melatonin in the morning for a couple weeks and report back in an open thread.
Have an N=1 study, which might be useful to someone. If you skip the rest of the post, probably the most generally useful point is this: you can get liquid melatonin off Amazon, and then you can easily adjust your dose to fit. Much easier to get 0.1-0.3mg that way than trying to cut a pill into ninths or worse.
I was on the short list of unfortunate sighted-with-non-24. *Was* being the operative word here. I am incredibly indebted to EY on two counts: once for convincing me, and then the people around me, that I had an actual medical disorder rather than just being undisciplined or lazy; and once for publishing that melatonin solution MetaMed recommended him, which with very minor modifications eventually cured – I’m going to use cured here, because it’s been two months and my schedule hasn’t slipped – my disorder.
My schedule was *very* extreme when I started – 27ish hours, 3-4 hours of shift every day – so taking melatonin at the same time every day was a non-starter. (Or rather, I tried it, several times, and got nowhere.) Plus, melatonin actually made my depression noticeably worse, which tended to have sufficiently deleterious effects on my spoon count that I couldn’t get myself to bed “on time” even relative to my schedule after a few days of it. I ended up working in smaller steps – I’d take melatonin around five hours before my target bedtime for a few days in a row, to shorten my sleep cycle by a smaller step (an hour until I was down to 25 hours, then half an hour, then skipping alternate days — I found I couldn’t accurately track and maintain steps smaller than half an hour, so I changed the frequency instead.) Then I’d go off the melatonin for a few days, taking it only as needed to maintain my shorter sleep cycle, for two-three weeks until my body got used to the new cycle.
(I was taking 0.1mg of melatonin, for the record. Like I mentioned above, I got these: https://www.amazon.com/Natrol-Melatonin-Liquid-Pack/ and took a tenth of the listed dose, which was very easy given the small pipette they provide.)
It took a solid five months, but I am happy to say that I am solidly done with that stage of my life. Posted here in the hopes it might help someone else.
After reading this article I have three follow-up questions:
1) Can I use melatonin when I wake up at 3 AM and can’t fall asleep again, or will this mess up my sleep cycles even more?
2) Is there an explanation (other than “something something circadian cycle”) why taking melatonin in the middle of the day (or first thing in the morning) helps to normalize the sleep cycle?
3) When I search for melatonin on amazon.de I get a lot of products with 5-HTP and L-tryptophan, which apparently are metabolized into serotonin and later melatonin. Is this the link between depression and sleeplessness?
I’m a bit surprised Scott didn’t link it, but for those who are interested in this topic, I would highly recommend Gwern’s deep dive into melatonin, which is excellent as always. Spoiler: he comes to the same conclusions as Scott.
Gwern reports that melatonin allows one to subtract an hour of needed sleep. Anyone have experience with this?
Also, does anyone know how much variation from person to person there is in the 8-hour of sleep rule? Should someone who sleeps less than this try to change it?
One kind of insomnia not mentioned in Scott’s taxonomy (and not entailed by it, as far as I can tell) is sleep maintenance insomnia. My wife has this. She falls asleep easily, but wakes up several times in the night. She is the featherweight champ of light sleepers. Sleep maintenance insomnia is a real struggle for her, and not something that melatonin seems to address (she has tried, under the supervision of a sleep doctor). Anyone have thoughts about how this fits into the story of circadian rhythms and melatonin?
Wondering how sneer club will spin this one as sinister: ‘Scott pushes
Melatonin on the Oppressed’, ‘Rationalist Wierdos OD Microdosing of Melatonin’
Less of this, please.
You should write more posts like this. It’s where you have the most expertise. Several of the sources you mentioned relying upon I had never heard of before.
1 – There is also allegedly a strong correlation between sleep disorders and ADHD, leading some to hypothesize causation. Certainly I seem to be having symptoms of both. Haven’t ever managed to fix the former reliably enough to find out whether it’d also solve the latter.
2 – Timed release: good or bad? How does it interact with dosage? I had previously guessed “good”, and my experience is that I needed about three of the 0.3mg pills for it to be effective, after which I bought 1mg pills instead. Maybe the lower dose would work better if it were instant-release?
Long time reader, first time commenter.
God I wish there were anything that could get me to wake up feeling refreshed. I’ve had sleep problems since age 5 and tried everything from melatonin and valerian to ambien but nothing works. To say nothing of meditation, diet change, hypnotherapy, exercising, fostering a sleep routine, etc. The only thing that ever worked for sleep was xanax – I woke up feeling engaged, alert, emotionally available, and focused. Found out the hard way that’s not a long-term solution. Any ideas what I can do?
In the vein of giving you a tip you may not have heard before, I find drinking soylent throughout the night (before sleep, if I ever wake up), works well for me. Others have noticed this too and theorize it’s the magnesium. So, if you haven’t already, you could try soylent or maybe just magnesium. Internet searches indicate magnesium glycinate might be best for sleep.
Two other things I’ve heard about – indica weed (probably obvious) and phenibut (addictive/rapid tolerance build-up, glowing sleep reports).
Thanks for the tip. Definitely tried phenibut before – but it leaves me feeling muddled the next day, unlike xanax (maybe a GABA A vs GABA B thing? No clue). Have not tried soylent though. Will try magnesium glycinate, that’s an interesting solution.
It sucks so much though, I always feel like a zombie. I’m so going to get fired one day.
Interesting. Good post Scott.
One thing I have noticed personally is that I tolerate 1mg/2mg(slow release) very well. I went up to 3mg and woke up at about 2am (~3 hours later) quite hypotensive (confirmed via sphygmo) which was pretty distressing. I haven’t met anyone else with that severe a side effect but it’s certainly one that’s possible.
I’d love to see a thread of people who are trying the recommendations. Suggested format:
Sleep issue: {advanced, delayed, non-24, [other]}
Number of days trialled: x
Dose in mg: y
Improved falling asleep?: {yes, no, somewhat, inconsistently, NA}
Improved staying asleep?: {yes, no, somewhat, inconsistently, NA}
Improved nightmares?: {yes, no, somewhat, inconsistently, NA} (only answer if you used to use melatonin but differently)
Notes: [free-form additions to contextualize results]
1. I’m one of the “Non-24-Hour-Sleep Disorder” people. My cycle is rightly about 26 hours, but when I have the scheduling flexibility to just live that way I normally go for 28 hours because it fits evenly into a 6 day week. I sleep beautifully when I am on that schedule. Too bad it’s not compatible with reasonable human living. When I want to approximate a 24 hour cycle, I use melatonin about 20 minutes before bed, which works.
2. I got the crazy dreams and early wake up when I first took melatonin. The problem for me turned out to be dose–I took like half the “serving size,” but as you know it was still like 10x too high of a dose. When I take doses more like .3mg, the crazy dreams and early wake up go away entirely. Maybe other people who have this issue are just taking too much for their system?
I think you’re right about this, but I would like to point out that the only pathway I know of this complicated comes from psychiatric drugs. Antipsychotics blocking D2 receptors which normally inhibits prolactin.