
[Disclaimer: Nothing here should be taken to endorse using illegal or dangerous substances. This was a quick informal survey and you should not make any important health decisions based on it. Talk to your doctor before trying anything.]
Nootropics are traditionally defined as substances that improve mental function. In practice they usually refer to psychoactive chemicals that are neither recreational drugs like cocaine and heroin, nor officially-endorsed psychiatric drugs like Prozac or Risperdal. Most are natural supplements, foreign medications available in US without prescription, or experimental compounds. They promise various benefits including clearer thinking, better concentration, improved mood, et cetera. You can read more about them here.
Although a few have been tested formally in small trials, many are known to work only based on anecdote and word of mouth. There are some online communities like r/nootropics where people get together, discuss them, and compare results. I’ve hung out there for a while, and two years ago, in order to satisfy my own curiosity about which of these were most worth looking into, I got 150 people to answer a short questionnaire about their experiences with different drugs.
Since then the field has changed and I wanted to get updated data. This year 850 (!) people agreed to fill out my questionnaire and rate various nootropics on a scale of 0 – 10 – thanks again to everyone who completed the survey.
Before the results themselves, a few comments.
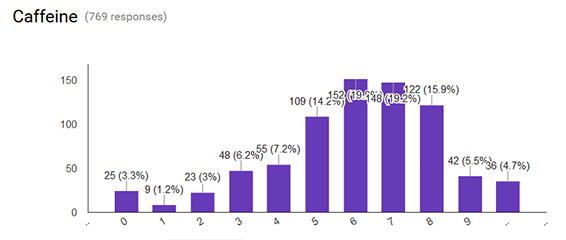
Last time around I complained about noisy results. This year the sample size was five times larger and the results were less noisy. Here’s an example: the ratings for caffeine form a beautiful bell curve:
Even better, even though this survey was 80% new people, when it asked the same questions as last year’s the results were quite similar – they correlated at r = 0.76, about what you’d get from making students take the same test twice. Whatever’s producing these effects is pretty stable.
A possible objection – since this survey didn’t have placebo control, might all the results be placebo? Yes. But one check on this is that the different nootropics controlled against one another. If we believe that picamilon (rated 3.7) is a placebo, this suggests that PRL-8-53 (rated 5.6) does 19 percentage points points better than placebo.
But might this be confounded by lack of blinding? Yes. That is, if companies have really hyped PRL-8-53, and it comes in special packaging, and it just generally looks cooler than picamilon, maybe that would give it a stronger placebo effect.
Against this hypothesis I can only plead big differences between superficially similar drugs. For example, rhodiola and ashwagandha are both about equally popular. They’re both usually sold by the same companies in the same packaging. They’re both classified as “adaptogens” by the people who classify these sorts of things. But ashwagandha outperforms rhodiola by 0.9 points, which in a paired-samples t-test is significant at the p = 0.03 level. While you can always find some kind of difference in advertising or word-of-mouth that could conceivably have caused a placebo effect, there are at least some reasons to think something’s going on here.
Without further ado, here’s what I found:
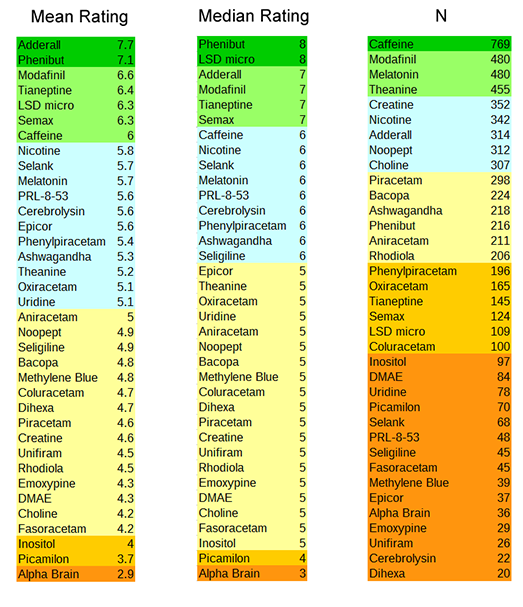

Some very predictable winners: Adderall is a prescription drug and probably doesn’t even qualify as a nootropic; I included it as a reference point, and it unsurprisingly did very well. LSD microdosing is the practice of taking LSD at one-tenth or less of the normal hallucinogenic dose; users say that it improves creativity and happiness without any of the typical craziness. Phenibut is a Russian anxiolytic drug of undenied effectiveness which is sort of notorious for building tolerance and addiction if used incorrectly. And modafinil is a prescription medication for sleep issues which makes users more awake and energetic. All of these are undeniably effective – but all are either addictive, illegal without prescription, or both.
I’m more interested by a second tier of winners, including tianeptine, Semax, and ashwagandha. Tianeptine is a French antidepressant available (legally? kind of a gray area) without prescription in the US; users say it both provides a quick fix for depression and makes them happier and more energetic in general. Semax is a Russian peptide supposed to improve mental clarity and general well-being. Ashwagandha might seem weird to include here since it’s all the way down at #15, but a lot of the ones above it had low sample size or were things like caffeine that everyone already knows about, and its high position surprised me. It’s an old Indian herb that’s supposed to treat anxiety.
The biggest loser here is Alpha Brain, a proprietary supplement sold by a flashy-looking company for $35 a bottle. Many people including myself have previously been skeptical that they can be doing much given how many random things they throw into one little pill. But it looks like AlphaBrain underperformed even the nootropics that I think of as likely placebo – things like choline and DMAE. It’s possible that survey respondents penalized the company for commercializing what is otherwise a pretty un-branded space, ranking it lower than they otherwise might have to avoid endorsing that kind of thing.
(I was surprised to see picamilon, a Russian modification of the important neurotransmitter GABA, doing so badly. I thought it was pretty well-respected in the community. As far as I can tell, this one is just genuinely bad.)
Finally, a note on addiction.
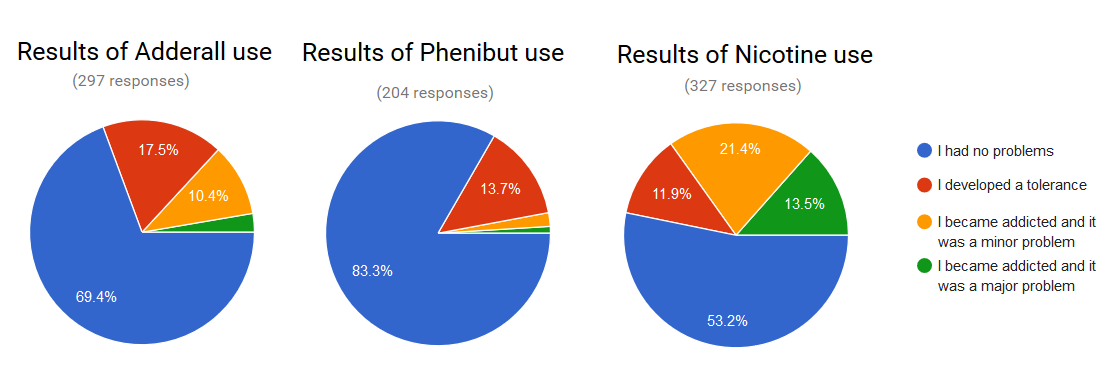
Adderall, phenibut, and nicotine have all raised concern about possible addictive potential. I wanted to learn a little bit about people’s experiences here, so I asked a few questions about how often people were taking things at what dose and whether they got addicted or not.
In retrospect, these were poorly phrased and didn’t get me the data I wanted. When people said they were taking Adderall every day and got addicted, I didn’t know whether they meant they became addicted because they were using it every day, or that they were using it every day because they were addicted. People gave some really weird answers here and I’m not sure how seriously I can take them. Moving on anyway:
A bit under 15% of users got addicted to Adderall. The conventional wisdom says “recreational users” are more likely to get addicted than people who take it for a psychiatric condition with a doctor’s prescription. There was no sign of this; people who took it legally and people who took it for ADHD were actually much more likely to get addicted than people who described themselves as illegal or recreational users. In retrospect this isn’t surprising; typical psychiatric use is every day; typical recreational use is once in a while.
Only 3% of users got addicted to phenibut. This came as a big surprise to me given the caution most people show about this substance. Both of the two people who reported major addictions were using it daily at doses > 2g. The four people who reported minor addictions were less consistent, and some people gave confusing answers like that they had never used it more than once a month but still considered themselves “addicted”. People were more likely to report tolerance with more frequent use; of those who used it monthly or less, only 6% developed tolerance; of those who used it several times per month, 13%; of those who used it several times per week, 18%; of those who used it daily, 36%.
Then there was nicotine. About 35% of users reported becoming addicted, but this was heavily dependent upon variety of nicotine. Among users who smoked normal tobacco cigarettes, 65% reported addiction. Among those who smoked e-cigarettes, only 25% reported addiction (and again, since there’s no time data, it’s possible these people switched to e-cigarettes because they were addicted and not vice versa). Among users of nicotine gum and lozenges, only 7% reported addiction, and only 1% reported major addiction. Although cigarettes are a known gigantic health/addiction risk, the nootropic community’s use of isolated nicotine as a stimulant seems from this survey (subject to the above caveat) to be comparatively but not completely safe.
I asked people to name their favorite nootropic not on the list. The three most popular answers were ALCAR, pramiracetam, and Ritalin. ALCAR and pramiracetam were on last year’s survey and ended up around the middle. Ritalin is no doubt very effective in much the same way Adderall is very effective – and equally illegal without a prescription.
People also gave their personal stacks and their comments; you can find them in the raw data (.xlsx, .csv) or the fixed-up data (.csv, notes). If you find anything else interesting in there, please post it in the comments here and I’ll add a link to it in this post.
EDIT: Jacobian adjusts for user bias
















Great stuff! I’ve been waiting for this with much anticipation; you have no idea how excited seeing that title made me. Quantitative data is sorely lacking in the nootropics community, but I think there’s a ton of potential there to make everyone’s lives better.
I find tianeptine’s opioid activity very suggestive and interesting, considering my experience (both personal and professional) with opioids and depression; but I haven’t actually looked at how significant it might be to its success and effects. I think endogenous opioid problems are under-considered as a candidate for the cause of various mental problems, though.
(For example, mirtazapine tends to do okay with otherwise treatment-resistant depression, and it messes around in that general area; less ambiguously, buprenorphine seems to work fantastically well for the same problem — and also for difficulty with motivation and concentration, IIRC — although it’s kinda hard to tell what’s addressing an underlying lack and what’s just partial-mu-agonist euphoria. But it definitely works!)
Mirtazapine has opiate activity? Darnit, how many years do I have to practice psychiatry for before I stop learning new things from random blog comments?
It’s weird! Mirtazapine, venlafaxine, and downstream modulation of opioid receptors — though, to be honest, I wonder how significant the effect can really be… but it certainly makes sense to me (but since I already convinced myself depression is often mediated in laege part by the opioid system, I’m kinda biased).
Unlike venlafaxine, it also appears to be a weak agonist of the kappa opioid receptors: https://www.ncbi.nlm.nih.gov/pubmed/22708686 … kind of like ketamine! Okay, now I’m reaching. But yeah, I’ve seen a decent amount of evidence that opioid activity is sometimes important in treating depression, particularly if severe or treatment-resistant, and I think it’s not really looked at too much (though I may be wrong there).
On the other hand, despite some studies claiming extra efficacy like the one above, mirtazapine didn’t do particularly well on your patient-rating-roundup, which I give a lot of credence to; I wonder if that might be due more to its immediately-perceptible and rather strong side effects (namely, hunger and drowsiness).
(Your commenters clearly form some kind of supercharged hive mind. Not me, though. We-I are only one tiny human-thing here.)
So is there something about Cerebrolysin that makes people really hyperbolic, or is that just an artifact?
Small N might account for it. But it did pique my interest. Another possibility is some kind of binary genetically mediated reaction to it.
(edit) – it also looks like the kind of thing that people might take in response to a major health problem (like a stroke), in which case the fact that it’s SUPER EFFECTIVE for some of those people might not be relevant to those not similarly affected. But I’m skeptical that the respondent pool has that many people with specific relevant conditions, I expect most of them are more or less the same pool of nootropic users that use the other various substances.
22 people used cerebrolysin. Of them 21 used caffeine. They rated it 1 point higher than the general population (1st,2nd,3rd quartile, mean). 18 used modafinil. They rated it the same as the population. 15 used adderall. Their distribution of opinion is more spread out: higher 3rd quartile and median, lower 1st quartile and mean.
N = 22. All you need is six people to rate it a 10 and then you’ve got the highest %10 in the whole sample. I’m guessing coincidence.
Not enough data to say. If you look at my graph (https://imgur.com/z3ubKdF) you could roughly say that Cerebrolysin’s mean rating could be anywhere as high as Tianeptine’s current mean rating or as low as Piracetam. So… it could be highly valuable or verging on possibly-entirely-useless. Cerebrolysin wasn’t on the 2014 survey either so can’t borrow any data from there. The next year’s survey probably won’t add much data either -at what looks like ~$100 for the Cerebrolysin/needles/swabs/etc (http://nootropic.eu/) the cost & injections deter a lot of people from trying it out and they instead go try some of the peptides like Semax.
Might be important to note that most of the respondents were male.
//All of these are undeniably effective – but all are either addictive, illegal without prescription, or both.//
Whyyyyy… :<
There’s a causative relation there.
Where can I find the survey? I don’t know what to make of the ratings because I don’t know what they *mean*. Seeing the actual question(s) asked might help.
https://docs.google.com/forms/d/1DFP4bSS00i_zQJ3nlw8KJxhUJjmrH9DA8cq0BsQciOc/viewform
This describes my experience, though I think I forgot to add a note when I took the survey. Since I started vaping I’ve been decreasing my nic level.
The nicotine one is one I’d love to see examined in more detail; e.g. what delivery methods do people use to get the nicotine into themselves (the tobacco cigarettes versus gum etc.), what exactly do people mean by “I had no problems”?
That could mean “I only smoke [tobacco cigarettes] now and again/I only smoke one or two cigarettes a day/I gave up with little to no trouble” or it could mean “I give up easily (but find I return to smoking after a while)/I don’t consider I have a problem (but ask my family/friends and it might be a different story)/I smoke regularly and every day, and I find I get nervy and irritable when I don’t smoke, but I don’t consider five cigarettes a day to be a large amount or a problem”.
I have a personal interest here; my father used to smoke but managed to give it up with no trouble, my mother smoked, tried giving cigarettes up, never succeeded in staying off them, smoked heavily for years and that’s how she got the lung cancer that killed her. So yeah, better information is better.
I smoked for a couple years, though never heavily; I peaked at an average of about three cigarettes a day, and more often I was doing one or two. Even that level led to mild but noticeable health effects: coughing, shortness of breath, endurance problems. So I decided to quit, and didn’t have much trouble or any physical withdrawal effects, although I had to deal with a few days of annoyingly intrusive I-want-a-cigarette cravings. (This is the opposite of how caffeine withdrawal works for me, incidentally.)
I’ve done the E-cig thing a couple of times, but never for long and it doesn’t excite me. It’s certainly an effective nootropic, but actual smoking is a much more enjoyable experience for some reason. Maybe it’s all the non-nicotine psychoactives in the stuff — I seem to recall there’s some kind of selective MAOI in it, for example. Or maybe it’s the fire thing.
Using WTA e-juice, it’s more enjoyable than simple nicotine e-juice, but still not quite as satisfying as an actual cigarette. Or perhaps more accurately, it’s not as satisfying as I remember cigarettes being, as having tried them a couple of times since then, they’re not as satisfying as they used to be.
Orphan, how is WTA vaping for sustained mental work?
I’d also like to see questions teasing out the timing there. How many of the addicted nicotine users are like me, a never-smoker? If you were already addicted to smoking, it’s not a surprise that your addictive habits might carry over; it’s more concerning if never-smokers using nicotine patches or gum or e-cigarettes also report high rates of addiction…
I downloaded the sanitized data (.xlsx), and when I try to open it, I get the error message “Excel cannot open this file. The file format or file extension is not valid.”
I have no problem opening rawdata.xlsx.
Not sure what to tell you. Works for me. Anyone else have this problem?
I have the same problem.
It’s a CFBF/CDF, not an XLSX.
Judging from the size and format, it probably contains the graphs. Did you intend that?
I’ve put it up as a csv now, see if that helps.
It works.
I uploaded the file to an online file conversion service, and it also got an error. How about providing a CSV version like you did with the raw data?
Still slightly irked that adrafinil wasn’t broken away from modafinil, since it’s legal and has similar effects.
Surprised that Selank didn’t do better. Ceretropic’s N-Acetyl-Selank formulation single-handedly eliminated most of my bad anxiety symptoms. Wonder if it’s just placebo (for the last two months) or it has a larger effect on me, or people aren’t using it for anxiety.
Selank is notable as the only one with a big difference across categories of people. Non-anxious or self-diagnosed anxious people rated it 5.something. People with officially diagnosed anxiety disorders rated it in the high 7s.
You should have asked about caffeine addiction. Its addictive properties are undeniable, and the withdrawal is *really* bad, and probably most American desk jockeys, to say nothing of many blue-collar types, are addicted.
I’m certainly addicted, but I make sure to keep my tolerance level low so I can get nootropic benefits by having an extra coffee or two. For comparison, I was never once addicted to nicotine, even when I smoked regularly. (I’ve considered taking it up again and vaping, but no one gets the aesthetics right.)
I’m not sure caffeine addiction symptoms are particularly obvious to most people using it. The thing with caffeine is daily consumption is so culturally normal that addiction isn’t obvious unless you try to quit, and the withdrawal while painful doesn’t (at least in my experience) come with cravings, those come later.
I quit caffeine once every year, before I go on holiday (don’t want to be forced to drink lousy hotel coffee). I just taper off over the course of 2-3 weeks, and that way the withdrawal isn’t painful at all.
Lousy hotel coffee is one of life’s great pleasures… in a totally different way from actual good coffee.
I think I’m one of the people for whom caffeine does little or nothing. If I take heavy doses of it (e.g. those energy drinks that are mainly all sugar and caffeine), and they need to be heavy, then it does elevate my heart rate.
But I don’t get the energy, wakefulness, stimulant effect of it. I never developed a coffee habit, I can start and stop drinking caffeinated drinks with no trouble, and I’ve never noticed any effect from “now with caffeine for extra jolt!” pills.
Chocolate is a whole different matter; I get very strong chocolate cravings at times, to the point where I need to get some goddamn form of chocolate into me or all hell will break loose 🙂
Yeah, I’ve never felt a craving for caffeine or noticed withdrawal symptoms, and I generally have at least one coffee, tea, or soda every day. But when I stop, it’s nothing unusual. Of course, the other explanation is that I’m bad at introspection in this regard.
I can drink a cup of coffee, tea, or soda right before bed and not have any trouble sleeping.
The only time I notice the effects is with a really high dose, like two caffeine pills. The drinks like coffee and tea, I drink for the taste.
From the information I’ve heard anecdotally, caffeine has a wide variance in how it affects people.
I seem to have a low tolerance so I notice strong differences in myself after drinking even one can of soda and do experience cravings (usually for soda rather than coffee).
I’ve given up caffeine cold turkey on three separate occasions and observed the withdrawal symptoms occur each time. It was the worst the first time I did it (pain, irritableness), noticeable but tolerable the second time (very weak pain, irritableness), and not very noticeable the third time. (I currently attribute this to decreased use each time.)
I don’t get cravings, but I do get withdrawal symptoms after a couple days — moderate to severe headache (sometimes bad enough to cause nausea, though not often since I was in college and drinking a pot of coffee a day), lethargy, motion and light sensitivity. This can cause problems, especially on weekends when I need to make my own coffee rather than grazing from the break room at work (or walk down the hill to Starbucks, but their coffee always tastes burnt to me).
On the other hand, tapering off to zero isn’t too hard if you don’t go cold turkey. I’ve done it a couple times, usually for practical reasons when I’m traveling. Afterwards, when I have my first cup of coffee for a couple weeks, it’s powerful — I feel jittery, highly productive, almost uncomfortably alert.
My usual level of diet coke or coke zero consumption, for years, was close to four liters a day. I could consume none for a week with no problem beyond thinking I would like a glass of it. So apparently caffeine isn’t addictive for me, and doesn’t have much effect.
A gallon of fluid a day is a huge amount to cut out. In those times that you did quit, what did you replace it with? Anything?
I wouldn’t call withdrawal *really* bad. I get a minor headache for a day or two, and feel tired if I continue on my caffeine levels of minimal sleep. If coming off of oxycodone from knee surgery was a 10, I wouldn’t even put caffeine at a 4 or 5.
Honestly, the headaches are as bad or worse as I build up tolerance to caffeine, which is usually what prompts me to give it up.
How do you feel about the cognitive performance aspect of withdrawal? I don’t usually get terribly bad headaches, but I notice my ability to think well drop drastically if I don’t have caffeine for a day. Maybe its the placebo effect or simple blame for my failures as a student, but that for me is the biggest reason why I feel I’m dependent on coffee.
I try to keep my caffeine habit in check by periodically resetting my tolerance. One time I tapered down too quickly. I had to go home sick. It was the worst head pain I’ve ever had.
Definitely have a healthy fear/respect of the power of caffeine addiction now.
The withdrawal is unpleasant but it doesn’t really qualify for really bad, particularly in the context of withdrawal.
I drink one to two pots of strong black coffee a day, plus a couple bags of high-caffeine tea and possibly a soda. Going from that to zero caffeine means having a headache for a day or two, but it’s not even enough to justify taking off work.
There’s a reason they don’t have rehab clinics for coffee users: if you have any reason at all to stop drinking it, you can easily do so.
I don’t currently take any nootropics, but I’m intrigued. Does anyone have any suggestions for reliable vendors for the non-controlled stuff like adrafinil, phenibut, and tianeptine?
r/nootropics has a list of reliable suppliers. The tl;dr is Nootropics Depot
I started taking tianeptine sulphate after reading about it in this blog, and I can’t tell if it’s doing anything at all. I’m taking it at a dose slightly higher (60mg/day) than what I found generally recommended online, and there’s tons of people who swear by this stuff.
Can someone expand on the specifics of what its effects are supposed to be?
It’s a mild euphoriant. It elevates mood. If you’re taking it for energy, and your primary cause of lacking energy is something other than dysphoria, I doubt it will help for energy. If you’re taking it for focus, and the primary drain on your focus is something other than intrusive anxiety, I doubt it will help for focus. It should boost anyone’s mood, though.
Before experimenting further with tianeptine, take a break. Tianeptine builds tolerance if you use too much of it. 60mg/day is high enough to eventually build a tolerance without being high enough to have blatantly obvious effects.
Then, try a higher dose. I’ve heard that the blatant effect threshold is 100mg. Don’t do that daily or often. 100mg of tianeptine is recreational. It builds tolerance quickly and may have long-term health risks.
Next, try low doses, and gradually increase them over a few weeks to see if at some point the effect seems to ‘kick in’. I don’t know if tianeptine is one of them, but I’ve heard that some nootropics have unintuitive dosing curves. I do know that tianeptine sulfate seems to have a subtly favorable effect on my mood at a dose one sixth of yours.
I’ve said “tianeptine” five times and “sulfate” once. I was only speaking specifically of tianeptine sulfate once. This is because, as far as I know, the difference between tianeptine sodium and tianeptine sulfate is that tianeptine sulfate has a longer half-life in the body, being therefore slower to set on and slower to fade. AFAIK, the two compounds are taken at the same doses for what are otherwise the same effects. If I’m wrong about the doses and effects of the two compounds being otherwise the same, adjust your estimates of how likely I am to be right about the rest of it accordingly.
If I’m right about the doses and effects being otherwise the same, faster onset may lead to clearer effects for experimentation, so you may wish to try tianeptine sodium and then switch back to tianeptine sulfate when you’re confident you understand how tianeptine affects you.
Pedantry: your last two tables are headed “percent” (both the in-table headings and the captions in the post here) but actually contain fractions.
This is probably a dumb question because I’m not a statistics person but how do you get a sample size of 769 for caffeine when you had 750 responders? Shouldn’t that be capped at 750?
(Fairly sure i’d tag this as “comments i’ll regret posting” if you could tag comments but think i’d regret not knowing more)
The fixed-up data .csv has 825 response rows. I assume 750 is just a rough number, counting maybe that some people didn’t fill out enough of the survey to be fully useful, etc.
Awww…no love from anyone else for plain old pseudoephedrine (a.k.a. sudafed)? Certainly, it is not nearly as good as adderall or even ephedrine (which used to be in all the popular diet supplements in the U.S. before the FDA cracked down on it), but for something that is legal, available down the block at your nearest grocery store, and dirt-cheap, I find it provides a nice little pick-me-up without the jitteriness of caffeine.
I honestly can’t remember if I’ve ever taken Sudafed; my sister, when she was taking something with pseudoephedrine in it for congestion or whatever, found it gave her the jitteriness and unpleasantly wired feeling along with rapid heart rate, so she didn’t like it.
Again, I imagine a lot of these things are down to idiosyncratic reactions: person A will find it great, person B will have bad side effects, and person C will find no difference.
For the record, ephedrine is still legally available in the US, although it can’t be marketed for diet purposes. Look for Bronkaid or Primatene at most pharmacies, particularly Walgreens.
Really? Awesome! Thanks for the info!
No problem. Be careful though; ephedrine is pretty powerful stuff.
Adderal XR is pure nerd in a pill, I’ve tried it before. I’m almost tempted to try and get some.
Question — has anyone here been diagnosed as ADHD, but had it missed earlier in life because of high IQ? I keep thinking I might be, from online self-tests, but I’m not sure what the benefits/costs would be to me of making it official.
Other than perhaps an Adderall or Ritalin prescription, which this chart makes a little tempting…
I wasn’t diagnosed as a child, I think partly because it still wasn’t being diagnosed as much as it is these days when I was a kid, but perhaps partly because I was mostly getting by in school with high intelligence compensating for minimal effort and poor focus. I did eventually get diagnosed in grad school (was seeing psych services partly for depression, but psych services at my school was pretty good, and had me tested for that as well on the basis of some of my issues). I also have at least one friend of similar age who was only diagnosed as an adult. Both of us benefit a lot from stimulants, so the prescription may be a good enough reason if you really have the condition.
Were their any downsides to being diagnosed?
Edit* Did I skip your last sentence or did you just edit it? Updating this to make more sense.
I edited it, and I didn’t experience any downsides to being diagnosed.
Thanks.
Yes – me.
I went through elementary school with horrible grades. The structure of high school let me get up onto the honor roll and then I went on to get an engineering degree and then work professionally.
At some point I started looking at my life and realized that something wasn’t quite right with me.
I went and saw a psychiatrist who determined that I was borderline for ADHD.
Given the circumstances, the easiest way to get a definitive diagnosis was to write me a script for modafinil. He said one of two things would happen:
1) I would have a significant reduction in symptoms, providing solid evidence of some ADHD-like condition.
2) I would be up on the roof of my house shooting at news helicopters, at which point I shouldn’t mention his name.
The first day I took it I cried. I was able to go outside and just *be* with the wind and the birds flying and be content. No more constant distraction by everything that I didn’t realize didn’t need to be there. It’s awesome.
Since then I’ve converted to duloxetine (off-label use) for primary management of ADHD (and other things) with 5mg Adderall tablets to handle remaining symptoms as-needed. My quality of life is drastically improved.
Surely not modafinil. methylphenidate?
Modafinil is a stimulant, but it is not approved for ADHD. Anecdotally, it doesn’t seem very good for ADHD. It would be good to get more data, but, for that very reason, it is totally inappropriate for diagnosis. (I think most people on amphetamine do not have ADHD and would be better off on modafinil.)
I’ll add that my wife did try Modafinil, on the prompting of a nootropics enthusiast, and she said it did absolutely nothing for her.
Well, I’d agree with the sentiment that adrafinil and modafinil should have been broken out from each other. I tried modafinil once and it worked pretty noticably. Adrafinil didn’t do anything for me.
That’s her, by the way, so I clearly mixed those up.
My wife was diagnosed as an adult. She did well in school growing up, was admitted to several Ivies but went to RPI instead since she was interested in engineering and they gave her a very generous scholarship. ADHD doesn’t have to mean you do poorly in school. How she did it I have no idea, though. The difference between when she’s taking Adderall (she’s a perfectly normal person) and when she’s not (can’t sit still for more then ten seconds and is constantly getting up and wandering away) is stark.
> Question — has anyone here been diagnosed as ADHD, but had it missed earlier in life because of high IQ? I keep thinking I might be, from online self-tests, but I’m not sure what the benefits/costs would be to me of making it official.
Yes.
I’ve struggled with depression/anxiety for my whole life, and once I stopped trying to treat depression and started trying to treat ADHD it got a lot better, very very quickly.
Turns out that sometimes “depression” is a totally legitimate reaction to poorly treated other problems
Pretty similar to my experience.
Yes, I has diagnosed at 28. It was never suspected due to high IQ and lack of hyperactivity. No downsides, though I keep it under wraps.
The only downside of a diagnosis I can think of is if you were planning on joining the military. In the US at least, they’ll allow you to join if you have the diagnosis, but only if you have not taken medication for it in the past year.
Actually, I guess if you plan to become a commercial pilot in the US, you can’t be on stimulant drugs, either. The diagnosis alone is not a disqualification.
I think of caffeine as a way of time-shifting alertness vs. sleepiness.
I am addicted to caffeine; I consume hundreds of milligrams a day in the form of coffee, mainly, and green tea and yerba mate a little. I choose coffee because I am consciously seeking its liver-protective effects.
But even having a tolerance / being addicted, what coffee does for me is enables me to choose when I will feel tired. It can’t give me more total hours of alertness, but it can help me rapidly complete the transition from still sleep to fully awake in the morning. And again, later in the day, it can stave off sleepiness until later.
So the point of caffeine for me is to choose *when* I will be alert, not to try to get more total hours of alertness (which it does not do), or cognitive improvement. I could do the same by napping, but caffeine is faster. Coffee naps are also a great tool to restore alertness, when I have the time.
Bromantane looks very interesting and appears to have been in use by enough people for a long enough time to establish a safety record, but there are theoretical reasons to be concerned about increased risk of Alzheimer’s disease. I’ve been unable to find any empirical data on whether or not these concerns are warranted. Does anyone have a read on this?
From a pragmatic perspective, I’m not sure it really matters how much any of the effects are due to placebo, as long as they’re real effects and not just a positive bias imposed on the evidence.
If we can make sure that placebos are actually effective interventions where there isn’t an obviously better alternative to use in their place, then there’s really no reason not to use placebos as a treatment.
One quick thing I noticed about the survey is that some respondents just gave a high rating to everything, so the drugs that these “nootropic-optimist” people were taking got inflated grades. To put a number on it, 499 of the 528 drug-to-drug correlations were positive and only 29 were negative. To put a better number on it, the standard deviation of the user’s average ratings is 1.62, and the SD of the drug’s average ratings is 0.82: most of the variance in user/drug ratings is driven by the user baseline and not the drug.
To adjust for that, I compared each rating to the user’s average over all the drugs they rated. Basically, I subtracted the row means from each row. Here are the adjusted results:
Nootropic Rating vs. User Average
Modafinil 1.329317892
Tianeptine 1.289107591
SemaxandNASemaxetc 0.894085597
LSD 0.810223255
Caffeine 0.678064245
Cerebrolysin 0.497841269
PRL853 0.465987613
SelankandNASelanketc 0.41024318
Melatonin 0.372214947
Epicorasimmunebooster 0.221123431
Phenylpiracetam 0.10914365
Ashwagandha -0.065035333
Seligiline -0.083027829
Uridine -0.102587165
Dihexa -0.148651715
Theanine -0.178589701
Oxiracetam -0.219684625
Aniracetam -0.297719383
MethyleneBlue -0.360068161
Bacopa -0.445575288
Coluracetam -0.456463627
Piracetam -0.49418767
Noopept -0.531590788
Unifiram -0.574670481
Creatine -0.673251745
Emoxypine -0.68213666
Rhodiola -0.691577188
Fasoracetam -0.760364641
DMAE -0.810338529
Choline -1.089267314
Inositol -1.140997313
Picamilon -1.52332507
AlphaBrainproprietaryblend -1.918130392
The results aren’t completely different, but they changed at the top: Modafinil and Tianeptine are the clear winners. This is because people who’ve used Modafinil are much more noo-skeptic in general: they give other drugs a 4.85 rating vs. a 5.51 average among Modafinil non-users.
They should use it as a marketing slogan: “Modafinil, the skeptic’s drug!”
Note: I didn’t participate in the survey and don’t personally take any nootropics besides caffeine because coffee is yummy.
Why did Adderall and phenibut disappear?
Also, how exactly did you do the adjustment? I was a little worried to try this because – for example, let’s say there was a large population of people who tried both tianeptine and AlphaBrain and nothing else. If AlphaBrain is in fact unusually bad, then this grouping would tend to make tianeptine look unusually good even if it was really just average.
I wonder if something like this happened for modafinil – I bet there are a lot of people who take modafinil and nothing else, and most other things are worse than modafinil.
Jacob probably omitted all the drugs you really cared about because their columns were headed with complicated titles like “Effectiveness of Adderall” rather than just the name of the drug.
Whoops, Adderall and Phenibut weren’t in the main range of columns so I forgot them, updated table below (Adderall is still the best).
My adjustment was simply subtracting the user’s average rating from all of his scores. The concern you mention is in fact a possibility, but it probably doesn’t have as much of an effect. I did a correlation matrix of indicators for trying a drug: the lowest correlation is -0.03 and the highest is 0.69. Basically, every nootropic makes you more likely to try every other nootropic.
There is one cluster of nootropics that are often taken together (high correlation for trying each drug inside the cluster) and don’t correlate much with any others: Fasoracetam, Unifiram, PRL853, Emoxypine and Dihexa. Even for that cluster, the effect isn’t large and my rankings are pretty close to the unadjusted rankings. In contrast, the effect of user-to-user variance is huge, and like I mentioned it’s bigger than the drug-to-drug variance.
Adderall 2.02
Phenibut 1.54
Modafinil 1.15
Tianeptine 1.10
Semaxa 0.75
LSD 0.62
Caffeine 0.50
Cerebrolysin 0.43
PRL853 0.35
Selanka 0.29
Melatonin 0.18
Epicoras 0.13
Phenylpiracetam -0.06
Seligiline -0.21
Uridine -0.22
Ashwagandha -0.22
Dihexa -0.23
Theanine -0.35
Oxiracetam -0.36
Methylene Blue -0.44
Aniracetam -0.46
Coluracetam -0.59
Bacopa -0.60
Piracetam -0.65
Unifiram -0.68
Noopept -0.70
Emoxypine -0.76
Rhodiola -0.85
Creatine -0.85
Fasoracetam -0.90
DMAE -0.96
Choline -1.24
Inositol -1.31
Picamilon -1.65
AlphaBrain -2.06
Now it doesn’t look too much different, but I think that this is a more precise measurement of objective rating.
That can be done better with a multilevel model, adding a random intercept for each user (based on my 2014 code). The results: https://i.imgur.com/z3ubKdF.png
library(reshape)library(blme)
library(lattice)
# previous: http://dl.dropboxusercontent.com/u/182368464/2014-ssc-nootropicssurvey.csv
nootropics <- read.csv("https://slatestarcodex.com/Stuff/fixed.csv")
nootropicsResponses <- subset(nootropics, select=c(Modafinil,Caffeine,Coluracetam,Phenylpiracetam,Theanine,Noopept,Oxiracetam,Aniracetam,Rhodiola,Creatine,Piracetam,Ashwagandha,Bacopa,Choline,DMAE,Fasoracetam,SemaxandNASemaxetc,SelankandNASelanketc,Inositol,Seligiline,AlphaBrainproprietaryblend,Cerebrolysin,Melatonin,Uridine,Tianeptine,MethyleneBlue,Unifiram,PRL853,Emoxypine,Picamilon,Dihexa,Epicorasimmunebooster,LSD,Adderall,Phenibut,Nicotine))
long <- reshape(nootropicsResponses, idvar = "Subject", v.names="Response", timevar="Nootropic", times=names(nootropicsResponses), varying=list(names(nootropicsResponses)), direction = "long")
summary(long)
blmr1 <- blmer(Response ~ (1|Subject) + (1|Nootropic), data=long); summary(blmr1)
rr <- ranef(blmr1, condVar=TRUE)
dotplot(rr)$Nootropic
Produces a similar ranking but uncertainty expressed. You can see how much broader a range Cerebrolysin covers, for example.
Thank you for doing this. Valuable service. I wish Scott would do this by default. Much easier to interpret.
Scott is interested in anxiety, so let’s estimate nootropics separately for anxious and non-anxious and see what happens:
nootropicsResponsesAnxiety <- subset(nootropics, select=c(Modafinil,Caffeine,Coluracetam,Phenylpiracetam,Theanine,Noopept,Oxiracetam,Aniracetam,Rhodiola,Creatine,Piracetam,Ashwagandha,Bacopa,Choline,DMAE,Fasoracetam,SemaxandNASemaxetc,SelankandNASelanketc,Inositol,Seligiline,AlphaBrainproprietaryblend,Cerebrolysin,Melatonin,Uridine,Tianeptine,MethyleneBlue,Unifiram,PRL853,Emoxypine,Picamilon,Dihexa,Epicorasimmunebooster,LSD,Adderall,Phenibut,Nicotine, MentalHealthAnxiety))
longAnxiety <- reshape(nootropicsResponses, idvar = "Subject", v.names="Response", timevar="Nootropic", times=names(nootropicsResponsesAnxiety)[1:36], varying=list(names(nootropicsResponsesAnxiety)[1:36]), direction = "long")
longAnxiety <- reshape(nootropicsResponsesAnxiety, idvar = "Subject", v.names="Response", timevar="Nootropic", times=names(nootropicsResponsesAnxiety)[1:36], varying=list(names(nootropicsResponsesAnxiety)[1:36]), direction = "long")
# dichotomize it to no problems or problems:
longAnxiety$MentalHealthAnxiety <- longAnxiety$MentalHealthAnxiety != 0
al <- blmer(Response ~ (1|Subject) + (1|Nootropic/MentalHealthAnxiety), data=long)
## What do the anxious find most helpful?
sort(ranef(al)$MentalHealthAnxiety[2,], decreasing=TRUE)
# (Intercept) NootropicPhenibut NootropicTianeptine NootropicModafinil NootropicLSD
# TRUE 3.091278122 -0.5105190709 -1.057200516 -1.138469415 -1.217272206
# NootropicCerebrolysin NootropicSemaxandNASemaxetc NootropicCaffeine
# TRUE -1.381575243 -1.756096591 -1.77087925
# NootropicSelankandNASelanketc NootropicMelatonin NootropicPRL853 NootropicNicotine
# TRUE -1.802979159 -1.878447062 -1.900276202 -1.909209198
# NootropicPhenylpiracetam NootropicEpicorasimmunebooster NootropicAshwagandha NootropicUridine
# TRUE -2.163747531 -2.390842171 -2.42676335 -2.465921564
# NootropicAniracetam NootropicTheanine NootropicOxiracetam NootropicColuracetam
# TRUE -2.530111173 -2.571222892 -2.590264411 -2.804064743
# NootropicNoopept NootropicPiracetam NootropicBacopa NootropicSeligiline NootropicCreatine
# TRUE -2.824889009 -2.831704912 -2.894511653 -2.961800907 -2.979285444
# NootropicMethyleneBlue NootropicDihexa NootropicDMAE NootropicRhodiola NootropicFasoracetam
# TRUE -3.088910432 -3.093002554 -3.250258882 -3.266642152 -3.379884865
# NootropicEmoxypine NootropicUnifiram NootropicCholine NootropicInositol NootropicPicamilon
# TRUE -3.407471261 -3.524940176 -3.577285412 -3.731613201 -4.247856452
# NootropicAlphaBrainproprietaryblend
# TRUE -4.292551616
dotplot(ranef(al, condVar=TRUE))$MentalHealthAnxiety
# https://i.imgur.com/GmjUmG8.png
## For which nootropics is difference between the anxious rating and non-anxious largest?
sort(ranef(al)$MentalHealthAnxiety[2,] - ranef(al)$MentalHealthAnxiety[1,], decreasing=TRUE)
# NootropicCerebrolysin NootropicSelankandNASelanketc NootropicAniracetam
# TRUE 2.698084031 1.127953895 0.9667527679
# NootropicAlphaBrainproprietaryblend NootropicPhenylpiracetam NootropicUridine
# TRUE 0.9309526632 0.8056889991 0.7814025454
# NootropicColuracetam NootropicLSD NootropicPiracetam NootropicDMAE NootropicPRL853
# TRUE 0.7804027708 0.7507048755 0.7113650908 0.6543638562 0.5925774774
# NootropicOxiracetam NootropicPhenibut NootropicNoopept NootropicCreatine NootropicAshwagandha
# TRUE 0.5615406515 0.5355206424 0.5092079112 0.5091827888 0.4908332287
# NootropicTianeptine NootropicBacopa NootropicInositol NootropicCholine NootropicMelatonin
# TRUE 0.4860944099 0.3748337733 0.3577989731 0.340854145 0.3242550006
# NootropicTheanine NootropicRhodiola NootropicNicotine NootropicFasoracetam (Intercept)
# TRUE 0.2636736807 0.1791294596 0.1655886185 0.1430377289 -0.02170039867
# NootropicEmoxypine NootropicEpicorasimmunebooster NootropicCaffeine NootropicModafinil
# TRUE -0.02276595555 -0.143210957 -0.1466009237 -0.2832420922
# NootropicSemaxandNASemaxetc NootropicMethyleneBlue NootropicPicamilon NootropicDihexa
# TRUE -0.3040346975 -0.3061321063 -0.4452781107 -0.5494996756
# NootropicSeligiline NootropicUnifiram
# TRUE -0.5852123712 -0.8846300255
Ranking in decreasing order: Phenibut Tianeptine Modafinil LSD Cerebrolysin SemaxandNASemaxetc Caffeine SelankandNASelanketc Melatonin PRL853 Nicotine Phenylpiracetam Epicorasimmunebooster Ashwagandha Uridine
Largest gain: Cerebrolysin SelankandNASelanketc Aniracetam AlphaBrainproprietaryblend Phenylpiracetam Uridine Coluracetam LSD Piracetam DMAE PRL853 Oxiracetam Phenibut Noopept Creatine
Largest decrease: Unifiram Seligiline Dihexa Picamilon MethyleneBlue SemaxandNASemaxetc Modafinil Caffeine Epicorasimmunebooster Emoxypine
So apparently stimulants do work on the anxious but they don’t like stimulants as much as the non-anxious, and really seem to have a thing for -racetams. I’m surprised phenibut is not the top gainer – Cerebrolysin and Selank must be quite the anxiolytics , it would seem, but that the anxious like AlphaBrain is questionable.
I think we can solve this using a fixed effects model, regressing score on both drug *and* respondent. Here is the relevant part of the output. For brevity I omitted the coefficients for the responders, which would teach us how generally positive or negative some (anonymous) person is.
The Adj. t-stat is for the difference between this drug and the average drug – hence why the ones in the middle are 0.
Drug Adj. Beta Adj. t-stat
Adderal 7.5 (2.9)
Modafinil 6.8 (6.34)
Phenibut 6.5 (4.15)
Caffeine 6.1 (4.33)
Tianeptine 6.1 (2.86)
LSD 5.9 (2.24)
Melatonin 5.8 (2.92)
Cerebrolysin 5.6 (0.8)
Nicotine 5.6 (2.04)
SemaxandNASemaxetc 5.6 (1.5)
SelankandNASelanketc 5.5 (0.96)
Seligiline 5.5 (0.87)
Uridine 5.2 (0.51)
Ashwagandha 5.1 (0.39)
Aniracetam 5.0 (0.15)
Phenylpiracetam 5.0 (0.15)
Bacopa 5.0 (0)
Coluracetam 4.9 (-0.18)
PRL853 4.8 (-0.25)
Oxiracetam 4.8 (-0.46)
Theanine 4.8 (-0.62)
Epicorasimmunebooster 4.8 (-0.32)
Fasoracetam 4.7 (-0.41)
Unifiram 4.7 (-0.41)
Creatine 4.5 (-1.71)
Dihexa 4.4 (-0.62)
Noopept 4.4 (-1.85)
Piracetam 4.4 (-1.87)
Emoxypine 4.3 (-0.89)
Rhodiola 4.3 (-2.09)
DMAE 4.2 (-1.65)
MethyleneBlue 4.0 (-1.53)
Choline 3.8 (-3.81)
Picamilon 3.5 (-2.99)
AlphaBrainproprietaryblend 3.4 (-2.48)
Inositol 2.8 (-5.03)
What do you think about the pros and cons of subtracting the user’s caffeine score, rather than the average score?
What about the problem of not just mean varying between users, but also the variance, the value of a point on the score? We probably don’t have enough data to estimate this. We could rescale scores by defining the caffeine-modafinil gap as the unit, but I’m not sure that’s a good idea.
All those things make sense, but even my coarse adjustment didn’t do much although it was also unlikely to introduce any bias. Looking at rating variance is going to be very noisy (you care about variance of variance when each user maybe rated only a couple of drugs) and I’m not sure it will help. Looking at caffeine-modafinil specifically is likely to introduce unneeded bias, for example from all the people genetically non-responsive to Modafinil.
But hey, the last thing I want to do is to discourage people from playing with data. Take some drugs and fire up the stats software, who knows what you’ll find?
What if some respondents are just more sensitive to substances in general? My roommate & I are opposites in this way (I react strongly to everything and have great relationships with lots of drugs, he reacts less to stuff). Supposedly it’s related to eye color?
It would be interesting to see citicoline and meldonium in the next iteration of this survey. In post-Soviet countries doctors prescribe them to people who experience prolonged fatigue. Meldonium is recommended to athletes to speed up the recovery after strenuous exercise. Based on the personal conversations I’ve had doctors generally consider these drugs effective. You can find online forum discussions by people who use them for mental performance enhancement but authoritative English-language information/feedback is scarce. Gwern hasn’t tested either of them.
I’ve never heard of meldonium. But notice that choline in general did poorly. If you click through the link to the last survey, you’ll see I differentiated by choline type – citicholine did a little better than some other forms, but still wasn’t too impressive.
Maria Sharapova just got “busted” for using meldonium (it was just made illegal by the WTA and she claims she didn’t know that).
My experience has made me ask if there are people who generally don’t respond to nootropics at all. I’ve tried Selank, Semax, and Aniracetam but have experienced no notable effects with any of them. My friends have reported strong effects from modafinil and Concerta (which I believe is a slow-release version of Ritalin?). OTOH, I didn’t experience any effects of modafinil or Concerta (I actually felt tired and took a nap after an hour of taking the modafinil).
Modafinil’s a bit odd for me. I never even slightly got the “wow, I feel so productive” effect, but it does make me less sleepy. Or rather, it makes me able to pull an all-nighter when I otherwise wouldn’t be able to at all.
On the other hand, I can take one and go right to sleep with no problems if I want (maybe spending an extra five-to-ten minutes awake). I just have less of an urge to get in the bed and fall asleep.
This has been my experience as well on about a dozen trials. It is actually fantastic for me as a stay at home dad. If the kids are up all night it keeps me reasonably alert during the day, while I can still grab a nap if they are both sleeping at the same time. In this sense it is pretty close to a wonder drug- the one caveat is that I seem to lose the ability to fall asleep at night easily if I take it after 2 pm or so.
Also took it once for a 7 hour night time drive- was prefect for that.
These things are pretty close to useless.
Drugs like Modafinil and Adderall , and caffeine/nicotine are all used by academics, fighter jet pilots, and pro gamers to *temporarily* improve performance. And its all temporary, with none of them recommended for long term continuous daily usage. Coffee is probably the only decently vetted one, and it stops working well with continuous usage.
For the rest? All these Aniracetam, Piracetam…I mainly see studies in very elderly patients with mild-moderate dementia. And usually one off ones, or just two studies. Those studies are all subject to this lovely effect in medicine. And the effects are always just very very minor, and usually subjective.
http://www.stat.cmu.edu/~ryantibs/journalclub/ioannidis.pdf
>Why Most Published Research Findings Are False”
If a drug besides a stimulant has worked in any significant manner to raise IQ or memory by any significant way without sides, the military would have already been using it by now.
Being a guina pig buying up all these blends of nootropic scams listening to other non double-blind subjective studies is just a terrible idea to spend your money.
All of these are so heavily out-done by good sleep, a decent diet, and regular exercise that its best to just assume its all a scam besides the stims. Well, unless its something like relaxing tea’s, but that’s a bit different.
I mean, you know something has a plausible chance of actually doing something, when there’s articles in the news (like there is for Adderall and modafinil) of Caltech students suddenly getting ADHD en masse….or something to that effect.
I hear this point about coffee a lot, and it frustrates me, because I think coffee has a clear benefit, which I tried to describe in my comment: it *time shifts* alertness.
I feel that with coffee I have exactly the same number of hours of peak alertness I would have without it. But without it, they would be not come at the times I want them to come.
So by drinking one cup around 8 AM, another at about noon, and a third about 2:30 or 3PM, about two hours after lunch, I keep the eight or nine most alert hours of the day all contiguous, from 8:30 AM until 5PM or so. I’m sure I’m more tired later in the evening, but that’s fine. And I need, I think, exactly as much sleep as I would have needed if I didn’t have my three cup coffee habit. But I’m not trying to reduce the amount of sleepiness I experience — I’m trying to choose which hours of the day I’ll be most awake.
Otherwise I would probably have peak awakeness around 10 AM until 1PM and gain from 3 until 8. That is not when I want to be most awake. Caffeine enables me to change the schedule of peak alertness hours. IT doesn’t add to the absolute number. Nor does it subtract.
This is a tremendously useful function. It’s why businesses give their employees free coffee. It’s why people drink coffee and tea on the job. It’s why tea time was invented.
Yes – there are non responders, that for whatever reasons, don’t respond much at all to nootropics.
There are also a lot of people within that group that take nootropics that really don’t make you “feel” anything. Which is the case for a lot of nootropics. They do however, allow your brain to process better in a variety of ways (working memory, verbal fluency, other). Those people are likely also not doing any deep cerebral work, where they’d notice a difference in the amount of numbers they can hold in their heads at once.
So.
If there is a future version of this study, I would recommend including separate side effect and effectiveness ratings for every drug. I was going to take the survey to report on modafinil, but I wasn’t sure whether to rate it a 0 or a 7-8. It’s definitely effective for me, but it has pretty bad side effects (headache or anxiety) at least 50% of the time I take it.
I used to think it was good to take vitamins, supplements, etc. because you could control what you’re getting and therefore know what caused what: if I take this vitamin B12 pill I know that’s pretty much all I’m getting, whereas if I eat some herb I’m getting a cocktail of all kinds of subtle things.
Now I am the opposite. I think our bodies have evolved to deal with the complex cocktails, especially the complex cocktails we’ve been consuming for a long time, like alcohol. Attempting to micromanage with nutritional isolates, I find, is ultimately not very helpful in the long run, to say nothing of being expensive.
So alcohol and caffeine are pretty much the only “drugs” I take, with rare exceptions (when I really need an antibiotic or whatever).
But why alcohol?
Not sure about onyomi, but I can speak as to why I consume alcohol:
1. It lowers inhibitions. Great when I’m not a perfect rationalist that can 100% “decide” to be gregarious, charming, and loose, and have it be instantly effective.
2. Social bonding.
3. By drinking myself, I encourage others with me to drink- which means group inhibitions decline, group cohesion goes up, trust increases, etc., etc.
4. It satisfies my “collector” impulse, and it’s fun to learn new cocktails and improve bartending skills.
5. I’ve experienced no problems with addiction.
To relax? Because it’s fun? I’m not claiming it’s a nootropic, just mentioning that I do use it. Some studies apparently show higher mortality among teatotallers than even heavy drinkers, though moderate drinking (as I engage in) is best. This may not actually be causative: could be teatotallers are former alcoholics with liver damage or something. But since stress is bad for you and moderate alcohol can be stress-relieving and enhance social bonding (which is good for you), it might just be that.
But even if it doesn’t make me live longer, it’s a good mood-manager sort of on the opposite end from caffeine: if I have trouble with energy to work during the day I drink more caffeine. If I have trouble relaxing at night I’ll have a glass of wine. Though I don’t use alcohol daily, whereas I do use caffeine daily (too much alcohol actually interferes with restful sleep even if it does make you feel sleepy, I find).
Also, if I’m experiencing a time of high stress I tend to drink less caffeine and more alcohol, and vice-versa, so the pair can help manage mood in that way as well.
Because it is… “delicious” isn’t quite the right word. Perhaps “sublime?”
Except gin, which is garbage squeezed from a pine cone.
So I’m supposed to say here that gin is much better in cocktails (and it is), but honestly I can drink a “smooth” gin like Gordon’s or something (which is good despite being cheap) neat.
In fact, I would rather have gin neat than drink your typical beer or wine. 😉
But my favorite gin cocktails are the Negroni and the Martinez. The Negroni is equal parts gin, Campari, and sweet vermouth. The Martinez is two parts gin to one part sweet vermouth, with a quarter part maraschino liqueur.
Gin is mostly what both my wife and I drink. I also sometimes go for tequila or whiskey, but she pretty much only drinks gin.
Your average well gin is pretty vile, all right, but at the high end it’s one of my favorite liquors. The key is to find a distillery that actually cares about what they’re infusing rather than just running a Christmas tree through a wood chipper and collecting the drippings.
This tends to be very regional. St. George makes some of the better ones in NorCal, and Aviation in PacNW.
Outrageous, gin over ice is some good drink, much superior to vodka, and cheap gin is much better than cheap wine relative to cost.
If I stay at a below-recreational dose (near 0.02 BAC), I get elevated mood, which leads to elevated productivity, for an hour or two without noticable impairments.
Disadvantages: Can be smelled, and builds tolerance if used frequently (i.e. also for recreational purposes).
My guess is that a lot of public speaking could be improved with a single small shot of hard liquor.
The Ballmer Peak?
My takeaway here is that modafinil is only a little better than caffeine. Which is nice, because that kills my temptation to try it and potentially screw up my brain chemistry. I’ll stick to tea.
I’m not sure I’d characterize closing almost half of the gap between “Meh, it’s pretty good” and “life-changing” as doing “only a little better”.
I’m not sure I’d characterize going from a 6.0 to a 6.6 mean rating as “closing almost half the gap between ‘meh it’s pretty good’ and ‘life-changing’.
Yeah, I was just looking at the relative ratings. The difference between 6 and 7 is pretty minor in my book.
As far as I know, there’s no danger of it “screwing up your brain chemistry”.
It’s just different from caffeine. The question I would ask is: do I want to have the ability to get by on very little sleep / pull all-nighters for a limited period of time? If that sounds appealing/necessary to you, then I would recommend it.
But if you’re anything like me, I don’t think you will get much out of it just by taking it every day in the morning. Maybe if you have trouble waking up.
If you want to try something different from and more powerful than caffeine, but with a longer history of interacting with the human brain, try the betel nut, assuming you can get your hands on it in America. I chewed them fairly often when living in Taiwan, which was always hilarious to Taiwanese, since they associate it with blue collar locals, i. e. the opposite of white foreigners.
But it is strongly stimulating in a way that, I find, provides more of the mental clarity aspect than caffeine.
Aren’t they highly carcinogenic? You probably shouldn’t leave that part out.
A quick Google shows a relative risk of 58.4 (!) for oral cancer in one population — which I’m pretty sure makes it 2-3 times as carcinogenic as tobacco chewing for that particular condition — and relative risks in the 1.2 – 1.5 range for a number of other conditions including cardiovascular disease. Not sure what that hashes out to in terms of absolute risk, but the cardiovascular risk alone would make me think twice.
I guess for me it’s self-limiting since I only use it when I’m in Taiwan, so I never really worried about it. But it does sound like it may not be a good option for regular use. But I would imagine occasional use when you need to finish a rush project or have a bad cold (it’s great for that because it numbs your sore throat, opens your breathing passages, and gives you energy), probably isn’t too risky. Some people definitely get addicted to it, but I never found any difficulty dropping it cold turkey.
@onyomi
Admit it, you were just trying to get the betel girl’s number, weren’t you?
I am very cautious about what I put in my brain. It already works very well for me, and the risks of any loss are a lot bigger than any expected gains for me.
Caffeine has been thoroughly vetted for ages in many cultures. I consider it entirely safe, for any amount that I would conceivably ingest. The only downsides (minor withdrawal headaches) are well-known and easily managed. And even there, I take my caffeine from tea rather than coffee, so my normal dose isn’t that high.
Modafinil may well be safe, but mostly it’s new enough that I’m not completely certain. Since I’m very loss-averse here, it seems better not to risk it.
I agree. I experimented a fair amount with chemically altering my brain states in earlier years to mostly bad results. Other than the basics, like caffeine, things that help seem only to help a little and/or for a little while; things that hurt can hurt for a long time. Not worth the cost/benefit to experiment, in my experience.
I don’t think I’m all that loss averse. I’m just not sure what I’d gain. Even the most enthusiastic reading of the results seems to indicate maybe I could sleep two or three hours less without feeling any ill effects. I don’t think adding three hours to the day would allow to accomplish anything I much feel like accomplishing that I can’t already do. There are other ways to gain three hours, too, such as not reading and commenting on blogs or social media.
Really? That sounds crazy to me.
If I could actually gain two to three hours per day with no ill effects, I would spend hundreds on modafinil. Not having enough time in the day to do all the things I want to do is the main problem I have.
Spending less time commenting on blogs would be cutting out something I find entertaining, so it’s not costless.
The problem is that modafinil, in my experience, doesn’t work that way. You can’t just cut out three hours of sleep every day. Or at least I can’t. Not without feeling very tired and miserable all the time, which isn’t worth it.
I only find it useful for transferring sleep, such as staying up for 48 hours now so that I can “crash” later. And since this is not extremely useful for me, I have yet to go through the ~40 pills I bought several months ago.
I would pay an incredibly amount of money to be able to have an extra 2-3 hours a day*! I would have to think hard before committing to a number but 25-50% of my post tax income seems reasonable to me.
Assuming I suffer no ill health and feel as mentally alert on average as I do now. (though I would definitely trade signifigant health for 3 hours a day! This would reduce the price I would pay).
I suppose I’ve already found a fair amount of time just by working from home, not having a television, and basically ordering every dinner rather than cooking. That’s quite a bit more than three hours out of an average American day. I’m just not sure what I’d even do if you gave me yet another three hours. Once I get to the point I can afford a daily maid, that’s like another half hour a day. When I finish my reserve commitment, which I no longer get much out of, that’s a few hours a week.
Hire a servant? Seems about right for the price range.
Also possible: Work less.
@ Anonymous:
I’m not saying that hiring a maid or working less might not be a reasonable decision, but it’s not the same.
For instance, if you consider your working hours to be be more pleasant than unpleasant, i.e. better than being unconscious, you ought to prefer eight hours of work plus three extra hours of leisure (gained at the expense of sleep) to five hours of work, even if the pills cost the same as you’d lose by working three fewer hours.
And it’s highly unlikely that a personal servant, especially of the kind that a normal person could afford, could possibly do enough to save you two to three hours a day of personal chores. They can’t take showers for you, and we have yet to perfect the technology of hiring someone to chew your food. 😉
@ Adam:
You don’t have a backlog of books to read, games to play, or other hobbies you wish you had more time to practice? You could learn how to play the piano or the guitar, take up gardening, learn to cook, You could have more time to spend with friends and family. Or just not have to rush as much to get ready in the morning and get things done.
Having 25-50% more waking hours is basically the same as living 25-50% longer, except better in that you get that time spread out throughout your life instead of tacked on to the end.
Not really, no. That’s probably part of the reason I have as much time as I do in the first place. I don’t really have hobbies. Don’t play games. Nearly everything I read is instructional in nature and basically part of job/continuing education. I used to swim and climb and would like to do those things again, but it’s waiting for surgeries and injuries to heal preventing me, not lack of time. Theoretically, I’d like to spend more time with my family, but they’re in California and I’m in Texas. I invite them out here and even offer to pay for the ticket fairly regularly and they don’t come (probably will when my dad retires in a couple years). I don’t really value in-person human contact all that much, but understand others do and some of those others are people I care about and would like to maintain good relations with. I don’t feel that requires a huge time commitment, though. Maybe once every year or two for a couple days.
@Vox
You could outsource your job to China!
@ Anonymous:
I heard about that guy. Very clever!
Juicers and blenders are rather like a technology that chews your food for you.
That’s where looking at data like this can really negatively fuss with an onlookers determination of it. Modafinil and caffeine are not even comparable. Modafinil is like lightening, whereas caffeine is like.. I don’t know.. a sea otter.
According to this survey, Caffeine appears to be the perfect nootropic drug. It’s 100% legal, cheap, only mildly addictive, and reasonably effective. There are other drugs with a lot more kick, but they have pretty strong medical downsides and are much harder to obtain.
Is this right, or am I missing something ?
Well, it’s certainly a pretty good one, which is probably why it’s so commonly used.
But all these drugs — the ones that aren’t placebo, anyway — are going to have different effects, and sometimes you want something that caffeine can’t offer. “Nootropic” is a pretty broad umbrella, it doesn’t describe a specific mechanism of action.
Melatonin, for instance, is like the opposite of caffeine.
It works, too. I don’t know if it makes me sleep better, but it allows me to “precommit” to going to bed on time by making me really drowsy.
If I say “I’m doing this now, but I’ll go to bed in 30 minutes”, I’ll say the same thing 30 minutes later. If I say “I’m doing this now, but I’ll take a melatonin pill”, then I really will go to bed in 30 minutes.
Have you tried a Schelling fence (or whatever this is called)? I’ve found declaring a certain time to be “time for bed” and a certain time to be “time to wake up” entirely sufficient to preclude 95% of sleep-procrastination.
I’m pretty terrible at getting to sleep on time – I tried a ‘Do less’ goal on Beeminder, with the ‘less’ being ‘minutes after midnight when I am not yet in bed with the lights out’ but that still didn’t help (by comparison, I’m pretty good at sticking to ‘do more’ goals, or at least am more likely to derail through forgetting to input data than through actually not doing the thing).
For getting up, I found the ‘countdown from 10’ technique pretty effective, but having learned this, I now feel the same flinch at starting the countdown as I used to feel at the prospect of just plain getting out of bed…
Theoretically, from reading plenty of nootropics groups, the point of much of this isn’t even supposed to be immediate cognitive enhancement, but the preservation of brain function as you age. Or even repair. It seems like half the people in any given group are there trying to reverse the negative impact of a prior drug addiction or brain injury. That isn’t impossible to study, but it’s not going to be an annual survey of users with no control group reporting their perception of how well it works.
The down side to caffeine is tolerance. To a first-order approximation, caffeine provides no net increase in performance, but allows you to trade a period of extra fatigue in the future for one of increased energy right now.
This can be very useful if you know about it and account for it. If you don’t, it’s possible to trade e.g. a month of increased energy to deal with your first really tough college class against a lifetime habit that isn’t doing you any good and a month of extra fatigue when you eventually go through withdrawal. Though I suppose it is possible to die without ever having paid back that loan.
Caffeine is one of the stimulants I generally limit myself to using once per calendar week.
If you like alcohol, coffee is doing you some good. It’s protecting your liver. The liver protective effects are exreme onc eyou drink three cups a day. There’s also a bunch of recent evidence that it’s protecting your brain from dementia in old age.
The neuroprotective effects are why I haven’t bothered to try tapering off long-term, but hepatoprotection is a nice bonus.
Also, though I agree that one is trading energy now for future tiredness/sleep/recovery with just about any stimulant, having that option does allow one to manage when one has energy: I am willing to trade being tireder at night, for example, for having more energy in the morning.
Same. Caffeine lets me do things I just can’t do without it, like stay up until 2 AM working on a project when I have to or be 100% alert for an 8:00 AM class without going to bed super early. The downsides are worth it, and not unmanageable.
Caffeine doesn’t make you more tired than you would have been without it.
The “crash” is just you going back to the same level of tiredness you’d be at if you had never taken it in the first place.
Also, the withdrawal effects don’t somehow build up over time. If you use caffeine daily for a year, that doesn’t mean you’re going to have a year of withdrawal effects.
If you use caffeine daily for a year, you’re only going to have a month or so of withdrawal effects. And yes, during that month you will be more tired than you would have been if you’d never touched the stuff.
But you only got a month or so of extra energy in the beginning. The other eleven months, you got the same level of energy (or lack thereof) that you would have had in the first point. That’s how tolerance works – your body’s setpoint adjusts to support the same long-term energy level as always, in spite of the steady dose of a stimulant. And with caffeine, that’s most of how withdrawal works, as you are stuck with the low setpoint and no caffeine for a month.
This is, to be sure, a great improvement over most stimulants which have actual addictive effects beyond tolerance, and which tend to demand more immediate payback at a >1:1 ratio.
The tolerance doesn’t just keep increasing to the point where it doesn’t work at all, though.
I have used caffeine daily or almost daily for almost my whole life. As I’ve said, I don’t feel like I get very much effect from just your standard Coke or cup of coffee. (I don’t experience much in the way of withdrawal symptoms, either.)
But if I take several caffeine pills because I really want to stay up all night, it works. And I could keep taking them and staying up longer. The limiting point is not the caffeine tolerance but the fact that, at some point, you go crazy from staying up too long.
And as many people have said in this thread, using caffeine every day allows them to be more alert during certain parts of the day, even if it doesn’t allow them to get by on less sleep overall.
It may be a bad idea to get too little sleep, but if you are, you’re probably going to be more functional on caffeine than not on caffeine.
Maybe if you drink an almost-lethal dose of caffeine every day, you would build up a tolerance so high that there’s no room to increase it. But who does that? In the average person’s caffeine use, there’s always room to get a bigger boost when you need it.
Nope, you’re completely right. The only “true” cognitive enhancers are methylphenidate (Ritalin) and amphetamines (like Adderall). Nothing else comes close, and even these have only modest effects.
You’re missing what actually is the case. If you’re making that determination, you’re probably doing so with great cause and reason! The data.
But this data does not say much about what’s really happening out there. Caffeine, is really not a nootropic in the same way that Oxiracetam is as an example.
The former will prevent you from feeling tired due to binding to adenosine receptors.
The latter will enhance glutamate signaling and positively modulate its receptors thereby improving neuronal metabolism, thereby enhancing things like the amount of digits you can hold in your head at once.
My prescription for perfect cognitive health:
1- Caffeine in moderate amounts
2- Nicotine rarely in e-cig/patch/lozenge form
3- Alcohol in moderate amounts
4- Aerobic exercise in large amounts
5- Good relationships with other humans
The most important is probably getting aerobic exercise to maintain the health of brain vasculature. Having good relationships to keep you cognitively on top of your game, and the drugs will give you some MINOR benefits. It’s hard to dissasociate cognitive benefits of alcohol and nicotine from the cognitive benefits of increased social interaction and better support structures. Nothing is worse for the brain than depression.
“The most important is probably getting aerobic exercise to maintain the health of brain vasculature.”
I don’t know if it’s true that exercise has only the one mechanism for improving mood/cognition, but, for me at least, the benefits are much better than any of the listed powders and pills. Obviously, it is more time consuming than taking a pill; and, obviously, the last g-ddamned thing I want to do at six AM is waddle around pointlessly on a treadmill. But! The results are hard to argue with, and the non-nootropic “side effects” are generally highly positive, and your doctor won’t look at you as some kind of obscurantist junkie when you tell her about it.
Some people suffer greatly from running. I think it has something to do with various levels of oxidant stress, and the pain related with working at such a high VO2-Max.
I can’t run because of this, so I swim.
Also just plain orthopedic injuries. I used to be a pretty accomplished runner, at least a state champ at the high school level. But my ankle is too jacked up now and I can’t run more ten feet without it giving out. I still love swimming, though (but need my rotator cuff to heal before I can do it again).
You know, it’s interesting: I’ve read various theories about how humans are natural-born distance runners–hunters who can’t beat most animals in outright speed, but who can follow for miles and miles, etc. and it’s true that some people can develop impressive endurance.
But, personally speaking, I sure as heck don’t feel like a natural-born runner. Every time I have tried to distance run with any regularity, even when I was younger, something has started to hurt. I’ve tried wearing those natural “vibram” shoes, running on earth instead of pavement, etc. Doesn’t matter. My joints just don’t seem to be able to take the repetitive stress.
I agree swimming is great for all the opposite reasons. Aquatic ape hypothesis?
The only outdoor athletic activity I’ve ever truly liked is skiing. And unfortunately, I don’t really get much opportunity for that one.
The ankle is years of repeated abuse, mostly from playing basketball and coming down bad, but the final straw was stepping in a hole at an Army school and refusing to come out of the field because I didn’t want to recycle and start the school over, so I just kept turning it over and over again. It never healed properly after that. Running itself was always pretty comfortable for me, just not now that my ankle doesn’t work.
Can confirm. Running usually takes more than it gives, at least for me.
I hate running too, mostly just because I find it incredibly boring. And obviously some people have limitations due to injuries, age, and other medical limitations, ask your doctor not the internet, etc. But I think the crucial distinction here is between being very sedentary and being somewhat active. It’s likely that some exercise regimens are better than others in terms of emotional and cognitive health, and maybe a similar survey could show some statistically meaningful differences. But – for me at least – the difference between being active in some way and not is at least as big as the difference between taking caffeine or tianeptine and not. It just requires motivation (which caffeine and tianeptine can help supply, tbh.)
And it should be noted as well that when you move your body around regularly you are using your body as mother nature “intended”, while when you treat it as a mostly vestigial organ for supporting your mouse finger you void the warranty. OTOH, when you ingest dodgy powders from the internet, maybe the downstream consequences are benign, but that’s not something I would necessarily feel confident in assuming. I’m a great fan of certain dodgy Internet powders, but I’d like it if the Fandom was a bit more vocal about this concern.
And it should be noted as well that when you move your body around regularly you are using your body as mother nature “intended”, while when you treat it as a mostly vestigial organ for supporting your mouse finger you void the warranty.
By the time you make it past 50, Mother Nature’s warranty period has been expired for a while.
You’re in Father Reason’s territory at that point.
“By the time you make it past 50, Mother Nature’s warranty period has been expired for a while.
You’re in Father Reason’s territory at that point.”
Except your cognitive peak is (very generously) around the age of 25, it’s just that by 50 you’re too senile to remember that. Let alone where I put my glasses WHICH I JUST LITERALLY HAD A MINUTE AGO.
This seems like solid grounding for a class action lawsuit.
I think Mother Nature intended for us to move, not to exercise– that is to move to accomplish some compelling purpose like getting food, protecting ourselves, or having fun.
We are not built for highly repetitive movement because we were told it’s a good idea or proof of virtue, and we were not built to push our limits unless there was an emergency.
Don’t Drone Me, Bro, have you checked on whether you pushed your glasses up on your forehead?
@ Nancy-
The gap between activeness and exercise is very grey. Walking a few miles carrying an animal carcass is “active” for one hominid and a workout for her descendant.
@ Nancy
I think a key difference is which is setting the pace — one’s own breath, or an internalized gym teacher.
Exercise has withdrawal effects as well. people who exercise often think that those who don’t exercise go around feeling as crappy as they do when they skip a day. That is a mistake people don’t make about caffeine.
This may sound weird, but it reminds of something that bothers me a little about good health habits: I find that, while you can improve your daily mood, energy level, health, etc. by doing things like exercise, meditation, eating right, etc., once you’re used to doing those things you feel even worse than you did before you start doing those things, at least for a little while, if you stop doing them. Sort of like being addicted to being healthy–mostly good, but still kind of an addiction, weirdly enough.
Like, recently, I’ve switched to a more vegan-ish diet and I feel better. Not 100% vegan or even vegetarian by any means, but just more fruits and vegetables and whole grains and less meat and oil and dairy.
Now, I’ve read some of these arguably orthorexic “raw vegans” or even just regular vegans saying “oh my god, I feel so awful if I eat dairy,” or even “I feel so awful now if I eat cooked food,” and I actually kind of believe them. They probably feel better not eating dairy or cooked food. But I’m not sure I want to know what that’s like, almost? Like, if I could feel better without cheese in my life, I kind of don’t want to be made painfully aware of that fact? I’m already kind of sad I know how much better I feel not eating gluten.
May sound silly, but we pretty much all have to make compromises somewhere: I’m sure I’d be healthier and happier if I could afford the time and money to get a massage every day. But I don’t want to know awful and tight I’d feel if I got used to a daily massage and then had to stop.
Veganism is fine, but steer clear of the “raw” bullshit just in case you were considering it (which fortunately you probably aren’t).
Cooking is to the human GI tract what clothes are to fur, what tools/weapons are to apelike strenght. All these things are “natural” to humans in the sense that we evolved to depend on them, losing our apelike physical attributes.
There is no serious argument in favor of raw eating. With most foods, cooking is necessary to make many of the nutrients digestible and absorbable (this is much more important than the alleged desctruction of nutrients by cooking), and unless one employs flawed cooking techniques, it is harmless.
I say all these things as a recovering raw vegan. My health improved a lot when I switched to cooked veganism.
The reason somebody may feel an improvement as he start eating raw is that it’s hard to intoxicate yourself when all you eat is fruit, vegetables, and sometimes nuts. However, I learned that, suprisingly, you can benefit from vegetables and less-than-perfectly-ripe fruit more if you cook them, and, more importantly, you can eat a wider variety of food, thus ensuring that you get enough calories and protein.
The chief reason someone may feel awful if he eats food different from his usual diet is that the digestive system adapts in the short term. It doesn’t mean that your current diet is superior or inferior. Extreme low carb eaters feel awful if they suddenly go back to eating carbs. But nobody will seriously argue that carbs are unhealthy.
I should have written “cooking is to the human GI tract what clothes are to human hairlessness and tools/weapons are to human inferior strenght.”
That way it’s logical, the way I first wrote it isn’t.
However, don’t be afraid of veganism itself. Personally, I tried lots and lots of diets; low fat well-cooked veganism works great for me.
And have you ever tried to quit oxygen? I can’t believe that stuff’s legal!
> 5- Good relationships with other humans
Where do I get a scrip for that?
Why is the response saying that someone is addicted while taking something once a month not at face value clearly saying they think they’ve become dependent on doing so?
How do you become “dependent” on taking something once a month?
Being “dependent” on it means you can’t function at a normal level without it in your system. It doesn’t stay in your system for a month.
I think it’s possible to be dependent on doing absolutely anything once per month. e.g. Seeing your children, exercising, playing devil may cry 3 on the ps2 for 27 minutes precisely, or burning a particular kind of red pencil, while singing nursery rhymes, and tap dancing, at 9:43PM. -Things can simply become something that someone focuses around and uses to unwind or otherwise “perform maintenance” on themselves. Something that they lean or are wrapped around as part of their current motivational, or other necessary, structure. e.g. I like to come home and sit down in a comfortable chair after a day’s work, which has direct objective value, but I also like to sometimes drink alcohol, which is less objective and direct. I can’t think of any particularly weird things that I currently like to do along these lines, but I’ve come across a lot of people with loads of these little rituals, and also some people for whom “everything must be in its place”, who will feel much better if some otherwise arbitrary thing is just how they like it, and potentially feel as bad as distraught if it isn’t. Imo most people+ have these kinds of little micro psychological anchors or rest points (or hyper points) or rituals or whatever.
Dependent also seems like a kind of low bar, like an addiction, but not to the level of that name because it can easily be broken through, so yeah between placebo, ritual, leaning on something, and whatever direct effect the drug is having (which might also potentially enable someone to carry out useful maintenance with lasting effects (e.g. meditation) during that duration), I don’t see how there wasn’t an obvious possible explanation for someone being dependent on taking something once a month. Like, look at hoarding as a behaviour, or anorexia, and surely it’s obvious that in a world with these things, among many many many, people can end up in states of mind that don’t have a logical purpose aesthetically aligned with the greater state of the universe. Obviously this explanation might not hold, but the point is why would those results be confusing, when “human minds are weird, and can attach or wrap around just about anything” is the obvious explanation. (not as in all human minds, but enough at least)
By the way, I would also like to see some opinions on Hydrafinil. It’s billed as Modafinil 2.0 but its chemical structure is actually really different and the response on r/nootropics seems to be mixed.
Next time can we add an optional field for IQ or SAT score or League of Legends ranking or whatever you feel the best intelligence proxy is?
Curious to know what improvements marginal people get vs average people.
I attend a health professions school in the Caribbean, whose students are mostly Americans and Canadians. Ritalin/Methylphenidate is very cheap and widely available here. Would love to see more survey data for it.
http://www.amazon.com/Encyclopedia-Enhancing-Foods-Nutritional-Substances/dp/0786441429
Somebody read this book? What you can tell about it?
Some of those work by increasing BDNF. I know for a fact that lion’s mane mushroom increases NGF. It improves my coordination when I take it. I’ve noticed it more than bacopa (which is also great). Tianepine and Semax didn’t work for me for some reason.
There’s also studies to support the NGF and lion’s mane link.
I like bacopa, mostly as anxiolytic or sleep aid. Can someone recommend a well trusted brand that has serious heavy metal testing in place?
r/nootropics did some third-party testing of bacopa back in April 2014. For bulk powder, the Nootropics Depot bacopa is a good choice, and what I use personally. If you want capsules (bacopa is not tasty!), Nootropics Depot carries them; if you want to buy from Amazon, use capsules that contain “bacognize”.
Thanks. I don’t deal with powders if I can avoid it (bad enough that whey and creatine are in powder form, but at least those taste decent).
I guess that means Swanson’s store brand then. Unlike last time I looked at, shipping to Europe seems not totally ridiculous anymore (9USD up to 2kg, instead of something like 30 for a single small bottle of caps)/
Excellent. Thanks for the results and the analysis. It might be useful to run Factor Analysis on the various ratings so that we can determine the major dimensions along which these nootropics vary. I’m really curious about it. I suspect that cholinergic activity would probably be one of the major factors, and dopaminergic activity would be another. But what else would we find? Probably something interesting.
For an example of a dimensional analysis that includes drugs of all other classes (psychedelics, dissociatives, etc.) see this study I conducted on the state-space of drug effects:
STATE-SPACE OF DRUG EFFECTS: RESULTS
Additional note: Picamilion sucks for one weird reason – it completely messes up my sleep schedule. I think this is a common problem.
An attempt at a factor analysis:
## rank each nootropic by level of missingness
sort(sapply(nootropicsResponses, function(y) sum(length(which(is.na(y))))))
## had to delete in order for factor analysis code to run:
## Fasoracetam Seligiline MethyleneBlue
## Epicorasimmunebooster AlphaBrainproprietaryblend Emoxypine
## Unifiram Cerebrolysin Dihexa
nootropicsResponsesFactor <- subset(nootropics, select=c(Modafinil,Caffeine,Coluracetam,Phenylpiracetam,Theanine,Noopept,Oxiracetam,Aniracetam,Rhodiola,Creatine,Piracetam,Ashwagandha,Bacopa,Choline,SemaxandNASemaxetc,Melatonin,Tianeptine,LSD,Adderall,Phenibut,Nicotine, Inositol, DMAE, Uridine, Picamilon, SelankandNASelanketc, PRL853))
library(psychology)
fa.parallel(nootropicsResponsesFactor)
# Parallel analysis suggests that the number of factors = 9 and the number of components = 6
# https://imgur.com/RaqZ9WW
## We strongly suspect there is a general factor of nootropics response from the multilevel models where random effects
## for users works so well. Unsurprisingly, `fa(nootropicsResponsesFactor, nfactors=9, missing=TRUE)` yields uninterpretable factors
## so we switch to the hierarchical factor analysis that 'psychology' provides:
omega(nootropicsResponsesFactor, nfactors=9)
# The estimated weights for the factor scores are probably incorrect. Try a different factor extraction method.
# The estimated weights for the factor scores are probably incorrect. Try a different factor extraction method.
# The estimated weights for the factor scores are probably incorrect. Try a different factor extraction method.
# Omega
# Call: omega(m = nootropicsResponsesFactor, nfactors = 9)
# Alpha: 0.91
# G.6: 1
# Omega Hierarchical: 0.61
# Omega H asymptotic: 0.63
# Omega Total 0.97
#
# Schmid Leiman Factor loadings greater than 0.2
# g F1* F2* F3* F4* F5* F6* F7* F8* F9* h2 u2 p2
# Modafinil 0.23 0.78 0.25 0.76 0.24 0.07
# Caffeine 0.27 0.76 0.77 0.23 0.10
# Coluracetam 0.48 0.73 0.86 0.14 0.27
# Phenylpiracetam 0.38 0.64 0.21 0.64 0.36 0.23
# Theanine 0.44 0.23 0.48 0.37 0.68 0.32 0.28
# Noopept 0.41 0.20 0.49 0.21 0.58 0.42 0.29
# Oxiracetam 0.43 0.44 0.44 0.22 0.75 0.25 0.25
# Aniracetam 0.44 0.30 0.49 -0.24 0.20 0.69 0.31 0.28
# Rhodiola 0.51 0.52 0.24 -0.23 0.67 0.33 0.38
# Creatine 0.51 0.38 0.26 0.27 0.59 0.41 0.44
# Piracetam 0.47 0.43 0.48 0.30 0.80 0.20 0.27
# Ashwagandha 0.50 0.56 -0.23 0.32 0.22 0.84 0.16 0.30
# Bacopa 0.46 0.59 0.61 0.39 0.35
# Choline 0.45 0.40 0.20 0.41 0.20 0.73 0.27 0.28
# SemaxandNASemaxetc 0.47 0.62 0.67 0.33 0.33
# Melatonin 0.31 0.79 0.78 0.22 0.13
# Tianeptine 0.43 0.64 0.20 0.67 0.33 0.28
# LSD 0.25 -0.23 0.70 0.30 0.74 0.26 0.08
# Adderall- -0.85 0.78 0.22 0.00
# Phenibut 0.32 0.76 0.75 0.25 0.14
# Nicotine 0.35 0.75 0.74 0.26 0.16
# Inositol 0.44 0.77 0.87 0.13 0.23
# DMAE 0.49 0.76 0.25 0.95 0.05 0.25
# Uridine 0.58 0.30 0.47 -0.23 0.81 0.19 0.41
# Picamilon 0.60 0.21 0.21 0.42 0.36 -0.38 0.90 0.10 0.40
# SelankandNASelanketc 0.57 0.28 0.30 0.47 -0.46 0.97 0.03 0.34
# PRL853 0.51 0.25 0.44 0.47 0.87 0.13 0.30
#
# With eigenvalues of:
# g F1* F2* F3* F4* F5* F6* F7* F8* F9*
# 5.2 2.5 2.1 1.6 1.6 1.6 1.5 1.6 1.4 1.2
#
# general/max 2.1 max/min = 1.96
# mean percent general = 0.25 with sd = 0.11 and cv of 0.44
# Explained Common Variance of the general factor = 0.26
#
# The degrees of freedom are 144 and the fit is 48.11
# The number of observations was 848 with Chi Square = 39985.02 with prob < 0
# The root mean square of the residuals is 0.05
# The df corrected root mean square of the residuals is 0.08
# RMSEA index = 0.577 and the 90 % confidence intervals are 0.566 NA
# BIC = 39014.04
#
# Compare this with the adequacy of just a general factor and no group factors
# The degrees of freedom for just the general factor are 324 and the fit is 53.98
# The number of observations was 848 with Chi Square = 45150.2 with prob < 0
# The root mean square of the residuals is 0.16
# The df corrected root mean square of the residuals is 0.17
#
# RMSEA index = 0.407 and the 90 % confidence intervals are 0.401 0.407
# BIC = 42965.51
#
# Measures of factor score adequacy
# g F1* F2* F3* F4*
# Correlation of scores with factors 254.25 244.41 162.81 22.25 419.23
# Multiple R square of scores with factors 64645.00 59733.97 26507.30 494.85 175752.76
# Minimum correlation of factor score estimates 129289.01 119466.94 53013.60 988.70 351504.51
# F5* F6* F7* F8* F9*
# Correlation of scores with factors 173.28 543.46 287.89 73.93 591.77
# Multiple R square of scores with factors 30026.39 295348.75 82883.34 5466.19 350193.48
# Minimum correlation of factor score estimates 60051.78 590696.51 165765.67 10931.38 700385.95
#
# Total, General and Subset omega for each subset
# g F1* F2* F3* F4* F5* F6* F7* F8* F9*
# Omega total for total scores and subscales 0.97 0.89 0.89 0.82 0.84 0.88 0.85 0.93 0.73 0.65
# Omega general for total scores and subscales 0.61 0.39 0.29 0.34 0.22 0.27 0.41 0.17 0.00 0.07
# Omega group for total scores and subscales 0.16 0.50 0.60 0.48 0.62 0.60 0.44 0.76 0.73 0.58
# https://i.imgur.com/XM7ufEC.png
What do these factors mean?
g is the general factor and works about as expected: those who rate one nootropic highly tend to rate others highly as well, and this explains ~0.26 of the total variance or ~R^2=50.1%, I think.
F1 is kinda a bit like anxiolytic/adaptogen, F2 is maybe stimulants (interesting to see LSD microdosing lumped in with noopept/aniracetam/oxiracetam – having difficulty sleeping after an LSD trip is commonly reported due to the stimulating effects), F7 looks like another stimulant cluster, F9 looks like it’s just for tea/coffee users, F3 I think must be a -racetam cluster (noopept/piracetam/choline/inositol/DMAE, no idea about theanine/Ashwagandha)…
But F4/5/6/8? I have no idea. F4 I would call a stimulant cluster except that along with the Semax/LSD/Nicotine loadings it also pulls in Picamilon & Selank, which I thought were supposed to be more anxiolytics! F5 might be more of a anxiolytic cluster but I don’t know enough about Uridine/PRL853 to know where those should go. And F8 is weird for mostly having negative loadings (-0.85 for Adderall! this is the only factor which includes Adderall too. huh?)
(You might think that retrying with `nfactors=2` might at least reproduce the usual stimulant vs anxiolytic split, but nope. The two non-g factors split up the stims about evenly: F1 gets Modafinil/Caffeine/Coluracetam/DMAE/Theanine/Noopept/Oxiracetam/Aniracetam/Rhodiola/Creatine/Ashwagandha/Bacopa/Choline while F2 gets Phenylpiracetam/SemaxandNASemaxetc/Melatonin/Tianeptine/LSD/Adderall-/Phenibut/Nicotine//Uridine/Picamilon/SelankandNASelanketc/PRL853. Very weird. Do we need to resort to deeper classifications like neurotransmitters? I’m not very expert on that.)
I took modafinil occasionally for a while (staying up to finish a project, long drives, etc.), and then there was a period of time where I took it with more frequency several times per week. I was working a job that was a terrible fit for me, and it helped me get through the day (increased single-minded focus, decreased anxiety thought spirals – a very strong positive effect on productivity, for me). Looking back on it, I see it as kind of a willpower splint. Almost as if I’d injured my willpower by working out of alignment with what I actually valued, like lifting a heavy weight with bad form and pulling a muscle.
I stopped taking modafinil when the company collapsed and I got laid off. I would prefer not to put myself in such an unnecessarily stressful position that I need that kind of — willpower exoskeleton again, on a regular basis. I could see myself using it again for some intense short-term project, if it was important enough. For now, guayusa tea is working really well for me — it’s a holly tree related to yerba mate and has caffeine and L-theanine in it. Helps with my alertness and focus, without contributing at all to anxiety (which coffee increases, for me).
My main reluctance around taking modafinil again is the emotional blunting effect I experienced. For some people, that might be a desired effect, but I think it allowed me to ignore really strong “YOU ARE MAKING YOURSELF MISERABLE!!!” signals. I’ve been trying to get better at listening to those internal signals (meditation, Focusing, Internal Family Systems), so I can make small corrections to what I’m doing before it gets so bad that some part of me has to yell and scream and act out to be heard.
Interesting. What you experienced on modafinil as “emotional blunting” I experience as “taking me to a calm, cerebral place where I like to be”. That is, I became aware that it was damping out minor mood swings but found the effect positive.
When I’m on modafinil I still love my wife and like our cat a lot, I’m just maybe less expressive about it. And one part of emotional range is not at all suppressed by modifinil – my sense of humor. I think I may be slightly more amusing and more easily amused when I’m on it.
Funny, I ‘m not a regular reader of slatestarcodex, and just found this today, as I am about 4 hours into my second phenibut trial. Two days ago I tried around 700 mg, with only the mildest ‘relaxing’ feeling, so mild it might be placebo, kind of underwhelming. This time, I tried 1000 mg 4 hrs ago , then 500 mg 2 hrs ago. So far, still not feeling much, although they say it can take as long as 6 or more hours for it to kick in..
A few things:
1. Adderall likely wins in popularity compared to the real smart drugs/nootropics (like Piracetam, Oxiracetam, Aniracetam) because it is far more known. And, most experienced nootropic users do not fuss with Adderall, but rather, the substances I mentioned (because Adderall is insane, and not a smart drug/nootropic whatsoever).
2. You’ve over stating the significance of the placebo effect. It’s not fancy packaging and marketing that trigger a person to like a product over another product, based on some perceived placebo effect. Rather, it’s how the substance effected them. Nootropics are not diet pills, they (the good ones) cross the blood brain barrier and effect neuronal/receptor site functionality quite definitively. And (no affiliation whatsoever), Alpha Brain is a subtle stack. It offers benefits to most people, that are noticeable enough, but they’ve made the stack (Onnit) a bit less potent over the years. Plus – a few of the ingredients dum down the effects of others (IE Theanine VS Alpha GPC).
Your assumption (because that’s all that it is, and it’s quite shallow) that a supplement like that won’t be effective because of “how many random things they threw into a pill” is about as accurate as your data actually saying something here. While I agree, they put a bit too many ingredients in that stack, each one of those ingredients are quite effective by themselves, and somewhat effective together. Huperzine A as an example.. well, just go buy some and dose 200MCG of it. When you end up trying to read the encyclopedia and understanding it all, I’ll be in the corner winking 😉
It seems obvious that you don’t take/have much experience taking nootropics. So, your opinion is limited to that. You’re on the outside looking in, which is fine. But readers should know that (readers, please know that).
I on the other hand, have taken nootropics for 6 years. I’ve NEVER had a “placebo” effect from smart drugs. You will either notice them or you won’t, based on a variety of things (their ability to cross the blood brain barrier, how you diet is, how much you slept last night, whether or not you have alcohol in your system and your liver is detoxing at the moment, neurotransmitter quantities, etc etc etc forever). Again – most experienced nootropics users will tell you the same thing.
While I can appreciate the time you put into this, you would actually learn more by taking nootropics yourself, and having a subset of really experienced nootropic users to ask questions.
So while, like someone mentioned in one of these other comments, quantitative data is lacking in the nootropics community, this is not the nootropics community. This is just one sector of data that you got from.. for all we know, unexperienced nootropic users. Or a mix of experienced and non experienced. Or people who aren’t hardcore nootropics users at all. Being a part of many nootropics communities on the web, I can tell you that a lot of those communities are filled with newbs. People just getting into them.
*note* – if anyone decides to look up who I am, you’d find that I own a commercial cognitive enhancement company, that sells a proprietary nootropic stack. But before that was ever a thought in my mind, I had 5 years of experience experimenting with nootropics/smart drugs at various capacities. It was in fact THAT that inspired me to build a company around them.
From the quality of this reply, I can well believe you have six years of taking brain-affecting chemicals behind you.
Funny, I’ve been taking nootropics for 7 years, and I’ve verified with randomized or blinded self-experiments I’ve OFTEN had a ‘placebo’ effect from smart drugs. (Most recently, LLLT.) You will either notice it or not, based on whether you bother to check.
While I can appreciate the time you put into this comment, you would actually learn more by running nootropics experiments yourself, and having a subset of really experienced psychologists to ask questions.
I tried rhodiola, having read that it’s the best thing ever, but it tastes awful. I found that I liked the taste (rather like ginseng) but got no effect from it whatsoever.
I know someone who tried provigal, and got 18 hours of sleep. Same thing happened when he tried it again.
Anyone else have tales of non-standard results?
Do you have any thoughts on 4-Hydroxy-4-methylpentanoic acid? It’s a drug which targets just the GHB receptor without hitting GABA, making it potentially have the antidepressant effects of alcohol/ghb without the side effects. Or maybe it does nothing at all. It’s hard to say, because there was one study of it done on rats which just said that it didn’t cause ataxia, and there appear to be no accounts whatsoever of actual humans taking it and reporting the results. Even its toxicity levels are up in the air. Unfortunate for something with so much potential.
This may be a good place for me to mention two related aspects of my modafinil experience that are a bit unusual.
The first is that I can take it legally – my GP is willing to prescribe it – for a reason unrelated to sleep disorders.
The second is the specific reason he’s prescribing it. A little-known off-label effect of modafinil is that it reduces spasticity in people with cerebral palsy – it is in fact the only drug or intervention of any kind that does this reliably.
That said, I admit that I view this as a pleasant side effect of what it’s really good for, which is helping me concentrate on creative work for long periods of time in which I would ordinarily need to sleep.
Also I owe some thanks to the rationalist community in general for having tested and (informally but effectively) certified a good offshore supplier – Sun Pharma – so that I can actually afford to take it.
My experience with occasional use of this drug has been extremely positive. I would go so far as to recommend it to other software engineers. Provided you can take it safely and legally, modafinil is a superb for putting you in a zone of optimal productivity. I won’t advocate daily use, as I have not done that out of a desire to avoid developing tolerance. But for occasional use when you want to be at peak performance and can block out a long stretch undistracted time, it’s brilliant.
Do you have any theories about why it works for both spasticity and narcolepsy? They don’t have any obvious relationship.
Nobody has any freaking clue why it reduces spasticity.
Then again, the mechanism of action for its anti-narcoleptic effect isn’t completely understood either. It’s partly a dopamine-reuptake inhibitor, but only a weak one; there are other things going on.
Modafinil is actually a rather interesting mystery, because most of the other drugs with similar wakefulness effects have nasty side effects and high addictive potential. Nobody expected to find such a benign drug in this rather seedy and dangerous neighborhood.
I see that you have included the age of the respondents in the survey. It would be interesting to see this displayed on a chart with age as an ordinate.
Here are the top five drugs. loess curves, with standard errors, and with scatterplot.
I wouldn’t draw any conclusions. The most plausible is that adderall declines with age. Outside of the 20s and 30s, it’s noise. The decline of theanine in the 20s and the rise in the 30s discourage me from believing either. The jump of modafinil from no better than caffeine in the early 20s to halfway to adderall in the late 20s is too fast for me to believe that it’s a biological effect. It’s probably change in the community. Maybe biological, but probably memetic.
Here is another graph that separates SSC readers from r/nootropics readers.
The two groups have different opinions on drugs, but SSC readers are older, so graphing by age is moving from reddit opinions to SSC opinions. I thought that the two weird results in the joint graphs, modafinil and theanine, might be due to that. But, actually, the modafinil weirdness was entirely due to r/nootropics and the theanine weirdness was due to SSC (thence to low N=78). Anyhow, the fact that these age effects are not replicated in the other population is pretty good evidence that they’re false.
Since I haven’t seen enough reiterations of this, let me just say very loudly: “DO NOT USE phenibut unless you really really know what you are doing”. In many users’ experience, it is a more addictive benzodiazepine (both operate on GABA receptors); with worse tolerance/withdrawal. If you know anything about the addictiveness of benzos, you know how scary that is. If not, do some research into the dangers of this drug class before taking it.
Being GABAergic doesn’t make a drug equivalent to benzos. Ethanol operates on the same receptor class. So does theanine.
(Wiki also suggests that phenibut operates mainly on a different part of the GABA system — a voltage-gated calcium channel, while most of the drugs I just mentioned operate on GABA A receptors, which are a ligand-gated chloride channel. But we’re getting a little outside my wheelhouse now.)
I’m not saying “it is equivalent because it operates on GABA”, I’m saying “it is more addictive because that is the experience of many users (and no surprise as it operates on GABA)”. The receptor similarity is additional evidence, not the main argument. Look at something like:
https://www.google.com/search?espv=2&biw=1162&bih=742&q=phenibut+site%3Awww.bluelight.org&oq=phenibut+site%3Awww.bluelight.org&gs_l=serp.3…9930.12144.0.12434.2.2.0.0.0.0.82.158.2.2.0….0…1.1.64.serp..0.0.0.C8mI8tb3YSI
And focus on the longer-term posts and not just the “woah I tried it this week and it feels so good!”. You’ll see a lot of bad experiences.
It’s definitely not as crazy as benzo’s.
OT:
I tried to buy a tall boy of Bud Lite. Bought a tall boy of Bud Ice by mistake. Now instead of drinking beer that tastes like water I’m drinking beer that tastes like shit. God is just.
I have to point out that all the strongly psychoactive ones somehow just happened to make it to the top. I mean phenibut may be great for anxiety but I have trouble believing it’s a genuine nootropic. The problem with these surveys is that people are usually terrible at evaluating their cognitive abilities. I suspect what’s happening here is that people are rating the substances which *make them feel the most different* as being superior to substances which they may not notice even if these substances are better. Retaining more information when learning isn’t necessarily going to be super noticeable but flooding your brain with dopamine is.
Being neurotic/anxious makes it difficult to concentrate on external things. I don’t know all the broscience behind phenibut, but I can assure you that the subjective experience for certain psychological makeups is very much this. And I can certainly see how people with different mental/emotional profiles wouldn’t get much out of it. I doubt there’s a such thing as a true “nootropic” that simply makes everyone smarter – maybe caffeine /amphetamine type things come close, though with a large number of caveats.
1 The middle way is best—no less than seven hours of sleep daily and no more than eight.
2 Going to bed every day at the same time and getting up every day at the same time is best. Let the body do it; throw away alarm clocks.
3 Due to human evolution an omnivorous, close to 100% organic diet is best. Shun fast food and junk food.
4 Shun all recreational, hallucinogenic, and psychedelic drugs—legal or illegal, including coffee, tobacco, and alcohol.
5 One hour of moderate exercise (fast walking, swimming, rope jumping, hiking) three to four times a week is best.
6 Look, listen, learn, laugh, live, love!
7 Love, not willpower, is the foundation of everything, including gratitude. 😀
“A day without laughter is a day wasted.” —Charlie Chaplin
“The fundamental obstacle to happiness is anxiety.” —Epicurus
1 The middle way is best—no less than seven hours of sleep daily and no more than eight.
My mileage varies considerably. Even on 8 hours, I feel noticeably sleep-deprived.
(Of course, since the average person needs 7-8 hours of sleep, the “middle way” will work for most people.)
What does evolution or omnivorousness have to do with whether or not one should eat vegetables grown with artificial fertilizers?
This is overconfident, low information blather.
Agreed. I feel like going through these point by point.
1) 7-8 hours of sleep.
Depends how old you are and on your family background, but this is good general advice.
2) Consistent bedtime/waking schedule, no alarm clocks.
I agree with this one, though alarm clocks are a useful safety net if you have kids and a job.
3) Organic omnivorous diet because evolution.
We evolved from single-celled organisms a bazillion years ago, and we are still evolving, so that’s not helpful. Instead, think about your family background. What did people eat in the part(s) of the world where most of your family is from going back 100-500 years? Meanwhile, “organic” is mostly a marketing ploy, though it’s probably a good idea to stay away from meat that’s been injected with weird stuff.
4) No drugs, no coffee, no alcohol.
Again, check with your family background. Humans have been using drugs for a long time, though what kind depends on where you’re from. Everything in moderation, though abstaining altogether is never a bad idea.
5) Moderate exercise–walk fast, swim, hike, or jump rope–3-4 times a week.
Good advice, but there’s a huge differential in strenuousness between those activities. It took me a whole summer swimming 5+ times a week to get to the point where I could swim for a solid 30 minutes, and I was otherwise in good shape. Meanwhile I could always walk fast for an hour even after a whole winter of sitting on my butt.
6) Look, listen, learn, laugh, live, love!
Yeah OK whatever
7 Love, not willpower, is the foundation of everything, including gratitude.
That doesn’t really mean anything either. Why do people bother saying stuff like this?
Charlie Chaplin is STILL one of the best physical comedians in any moving picture format…but he was a big fucking asshole. He’s better at making me laugh than telling me to.
“What did people eat in the part(s) of the world where most of your family is from going back 100-500 years?”
My impression is that a lot of people these days don’t have somewhere that most of their family is from. I suppose that they should experiment with food from the top two or three fractions of their heritage.
Excellent information and job well done (thanks for taking the time to put this together, as a vendor this information is invaluable to see what’s trending and what’s working well). Some are not surprising based on the last survey completed. Notable new ones (at the top no less) LSD microdosing, which is very trendy right now, I also don’t recall Phenibut on the previous list, but it’s certainly very popular. Not terribly surprising that Alpha Brain is on the bottom of the list.
Great job on the latest survey! Surprised LSD microdosing is below Tianeptine and on par with Semax. Interesting results, for sure.
Addiction is defined too vaguely for any useful conclusions.
For instance take the supposed result that users taking the drugs under a doctor’s care at the prescribed dosages are less likely to become addicted.
I take adderall in this fashion and would answer “not addicted” even though *everyone* who takes adderall in a daily fashion at any non-trivial dosage will go through withdrawal (huge amounts of sleep, depression etc..) if they stop taking the drug. When various factors meant no pharmacy came through one week it made for a really shitty week.
However, the mere fact that I have the medical establishment behind me supporting my continued usage (or controlled removal if it becomes a health issue) means I don’t face the problems that render dependence on a compound addiction. If I faced exactly the same physiological effects but had to depend on unreliable suppliers, the possibility of confiscation or drug testing etc… etc… that same physiological effect would amount to a problematic addiction.
You might contend that I am confusing addiction with problematic addiction but if so the ambiguity is inherent in our words. Consider someone who suffers from severe chronic pain of some kind. They are *MORE* dependent on high doses of opiods (or other pain relevier) than any recreational user. The recreational user may experience severe unpleasantness for weeks or even months (duration may be related to how the drugs affect the g-protein receptors with some agents suppressing regrowth more than others) but the chronic pain sufferer will immediately become incapacitated with agony for as long as they abstain. However, we would not deem that kind of “medical need” addiction anymore than we would deem a need for asthma meds or nitroglycerin addiction.
Addiction is a hopelessly loaded and confusing word to use in drawing any conclusions.
Have you ( or anyone else in the community ) seen any results or evidence of effectiveness for L-Alpha glycerylphosphorylcholine ( more commonly known as Alpha-GPC )? I personally use it and find myself believing it to be extremely effective, with notable difference in taking it + my dextroamphetamine ( generic Adderall ) or taking only my dextroamphetamine. That said, as I am a sample size of only one, I am high skeptical of my results and would love to see some supporting or contradicting evidence.
Alpha-GPC should be under Choline.
I find it has no effect on my normal state, but if I’m really tired after work it cuts out the “brain fog” some. Caffeine makes me feel awake again, but I still can’t think about anything even if I feel awake.
BTW, supposedly it eliminates the headache from modafinil.
I think the list is very useless. I have seen people battling benzo addiction with phenibut, liking nootropics for better vision or because they had a better performance at their waitress job. You know were this is going. People have different reasons to take nootropics, this should be factored in.
I know I’m very late to the game with this, but I’ve done a Bayesian analysis of the data that accounts for both discretization (respondents can give only one of 11 possible responses, although effectiveness is a continuum) and scale usage heterogeneity (some people spread their responses out more than others; some tend to give higher answers than others in general). The plot is here, and the writeup is here.