
[Epistemic status: Very weak – I’m still trying to figure all of this out. Some things in here will almost certainly be wrong. Please don’t let this overrule what government agencies or your common sense are telling you. For a more careful guide to the coronavirus and what to do about it, see here.]
Prepping
For a description of why you might want to prep, see Putanumonit: Seeing The Smoke. For a description of how to prep, see this article by Kelsey. For a really intense guide by a professional prepper, see here.
But there’s such a thing as being too intense. You probably won’t need to store water – the water kept running in Wuhan. You probably won’t need a generator – Wuhan has electricity. The most important thing seems to be food (and toiletries, and other necessities). If the epidemic gets bad, you’ll want food so you can avoid going out to coronavirus-filled supermarkets. And if you get the coronavirus and are feeling sick, you’ll want food at home so you don’t have to get too far out of bed.
What about Amazon? Getting fresh groceries delivered whenever you want seems like a pretty good alternative to stocking up on canned beans. You’d need faith that it won’t get so bad that Amazon’s logistics break down. I think that faith is mostly justified – The Chinese version of Amazon seems to still be making deliveries in Wuhan. And it’s hard to imagine anything – pandemic, nuclear war, demon apocalypse – getting between Jeff Bezos and his next billion dollars. Three cheers for capitalism!
Coronavirus can remain on objects for a few days, and Amazon warehouse workers may come into work with the condition, so if you’re using Amazon as part of a self-quarantine strategy, you should probably open packages away from your main living space, using gloves, and disinfect anything inside that doesn’t have its own packaging from the manufacturer.
How bad will it be?
From the Chinese numbers, people have estimated these death rates:
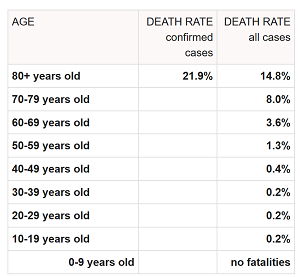
The good news is that it’s pretty unlikely to kill young people. The bad news is that even young people seem to have severe cases that can land them in the hospital. This comes from former FDA commissioner Scott Gottleib – the rate of hospitalizations for flu vs. COVID-19 by age group:
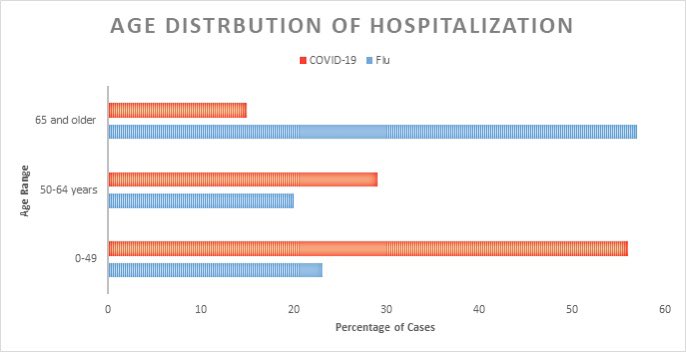
This page says that the Chinese population is 70% under 49, 20% 50-65, and 10% 65+. So the graph above implies that every demographic has approximately equal hospitalization rates, which other sources suggest are 15% to 20%.
This is a weird pattern – why are so many young people getting hospitalized if almost none of them die? Either the medical system is serving these people really well (ie they would die if they didn’t go the hospital, but everyone does make it to the hospital, and the hospital saves everyone who goes there), they are being hospitalized unnecessarily (ie they would live even if they didn’t go the hospital, but they do anyway), or it’s statistical shenanigans (eg most statistics are collected at the hospital, so it looks like everybody goes to the hospital).
Are these an overestimate? Maybe most cases never come to the government’s attention? There’s some evidence for this. In South Korea, coronavirus started spreading through a tightly knit cult, so the government had to test the whole cult, including the people with no symptoms. 70% of asymptomatic members tested positive for the virus, suggesting that many cases may not come to medical attention (although some of those people might have just been in the incubation period). So hopefully the 20% hospitalization rate will prove to be a worst case scenario, and the real number will be less.
[EDIT: several people are saying that in other countries the hospitalization rate is closer to 5%; let me know if any of you find a source for this]
Self-quarantine starting now vs. later?
Rough Fermi estimate: there are 10 reported cases in the Bay Area. Optimistic scenario, we’re only missing another 20. Median scenario, most haven’t been detected and there are really 100. Pessimistic scenario, 1000.
(in a draft, I used the term “worst-case scenario”, but it turns out some people can think of some really bad scenarios. Let’s stick with “pessimistic”.)
The number of infected people doubles every 2-7 days. Let’s say optimistically 7, median 3.5, pessimistically 2.
So over the next week, we can expect there to be 20 (optimistic), 300 (median), or 10,000 (pessimistic) new cases in the Bay Area.
The Bay Area has a population of 8 million. So we can expect that 1/400,000 (optimistic), 1/30,000 (median), or 1/800 (pessimistic) of the population will be infected in the next week.
Suppose you’re trying to decide whether to quarantine your 5-person household. Worst-case scenario you multiply the number by 5. But realistically your infection risk will be correlated – you’ll be in the same areas, hanging out with the same social circle. If the epidemic spreads solely among Chinese-American schoolchildren in San Mateo, and none of you are in that demographic, then you’re all safe. So for the median and optimistic scenarios, we’ll say risk varies with square root of the number of people in your house, and for the pessimistic we’ll keep it linear. So per house risk is 1/200,000 (optimistic), 1/15,000 (middle), or 1/160 (pessimistic).
So even in a pretty pessimistic scenario, Bay Arean households have a less than 1% chance of getting the virus this week (people from elsewhere will have to redo the math with their local numbers). Next week you can check how many cases there are (and how many hidden cases you suspect there to be) and reassess.
Ways this model might fail: there are more than 1000 cases in the Bay Area, you live with more than 5 people, some of the people you live with have an unusually high risk profile (are health workers? travel a lot?), unknown unknowns.
EDIT: Daniel Filan on Less Wrong has made a more complete risk assessment model.
What’s the endgame?
The theory is: you quarantine yourself for a few weeks or months while the epidemic is going on, eventually there aren’t enough virus-naive hosts to sustain transmission, and we’re all safe until the next time some moron in China eats a bat.
This theory might not be true. CDC director Robert Redfield says:
This virus is probably with us beyond this season, beyond this year, and I think eventually the virus will find a foothold and we will get community-based transmission…The containment phase is really to give us more time.
I don’t know exactly what this means, but it sounds like he’s saying it will become something like the cold, flu, or chicken pox – a virus that’s just ambient all the time, and you’re always at risk of getting it. You can’t outlast it because it doesn’t go away.
If that’s true, the goal of quarantine would change to outlasting the crisis. There will probably be a peak of the epidemic when hospitals are overcrowded and there are no spare ventilators and you really don’t want to need medical care. If you can get past that, and catch it a year or two from now, there will be spare doctors and nurses to care for you and spare ventilators to support you if you need it.
But if that’s true, maybe it would also be acceptable to catch it early and beat the rush. If you catch it literally today, you’re near-certain to get a hospital bed; if you catch it a month from now, who knows? This is another argument against premature quarantine, although not a strong one if you expect your quarantine to work.
(This part is especially speculative, even more than the rest of this post. Please don’t go out and try to catch the coronavirus on purpose.)
No, really, what’s the endgame?
Some sources argue that recovered patients can get reinfected with coronavirus, ie people don’t build immunity after surviving it once. This would really suck. I don’t know exactly how to model this – surely it wouldn’t mean a perma-epidemic all the time – but at the very least it would mean it was around permanently and even good quarantines wouldn’t be very valuable.
Microbiologist Florian Krammer (link) thinks these are probably false positives. Some other people have said they might be very elderly or sick people with abnormally poor immune responses. Let’s hope.
Home health care
Some people in the rationalist community have put together a document with some useful suggestions. Among them:
– Most coronavirus infections will be generally mild and probably treated at home. Make sure your home has oral rehydration solutions like Gatorade or Pedialyte available to deal with dehydration from vomiting, diarrhea, or other causes, and Tylenol available to help with fever.
– If you think you’ll fret a lot about whether you need to go the hospital, get a pulse oximeter ($20 on Amazon). Readings consistently below 90-94% are pretty bad and mean you should seek immediate treatment.
– Everything that makes you feel better and healthier in general helps your immune system too, so get good sleep, eat healthy, and take Vitamin D if you’re deficient.
– The best way to avoid infection is still to wash your hands frequently and avoid touching your face. Less good but cooler ways to avoid infection include putting copper tape over everything in your house (copper kills viruses on touch). For best results, use a combination of copper, iron, and silver tape to be protected from coronavirus, fae, and werewolves simultaneously.
Don’t visit Grandma
Seen on Tumblr: the coronavirus death rate is 0.2% for people in their 30s and 15% for people in their 80s. The vast majority of our concern should be for our elderly and for what happens to the 2020 election after we lose every presidential candidate except Pete Buttigieg.
You might want to call your elderly parents and grandparents and ask them to store enough food and water to stay in the house for a long time. You might want to talk to them about how bad things would have to get before they should stop visiting large gatherings, and how bad things would have to get before they stop leaving the house. You might want to explain to them how to use Amazon if they don’t already know how to do it, or coordinate with them so you can Amazon them things if they need it later on. You might want to make sure they have enough of their prescription meds stored up in case going to the doctor suddenly becomes harder. You might want to talk about whether they should come stay with you assuming you aren’t more exposed to the outside world than they are; if you have kids who go to school every day, your elderly relatives might be better off at their retirement home.
But have these conversations by phone! Don’t visit them! The last thing we need is everyone suddenly going and visiting the elderly much more often than usual!
(Grandma, if you’re reading this, the reason I haven’t called you about this yet is that Dad is investigating options and he will be contacting you soon).
Also, although the original post was titled “Don’t visit Grandma”, technically it’s Grandpa you should be most concerned about – elderly men seem to have twice the death rate of elderly women. [EDIT: Michael Keenan points out this might just be because elderly men in China smoke a lot and have bad lungs]
The view from China
A Chinese-speaker on the subreddit sums up what they’ve gleaned from Chinese social media. For example:
People are talking less about Wuhan and more about the rest of the world in recent days. The worst of the overload in Wuhan is over, and the quarantine in the rest of the country is keeping spread more or less manageable. People are talking more about the usual scandals and fandom stuff. Meanwhile, people are horrified at, say, Japan’s mismanagement of its earlier cases. I’ve seen the attitude “we sacrificed Wuhan to slow the spread and you guys are just wasting your window of opportunity?” And comments that maybe the CCP isn’t that incompetent in comparison after all.
The framing of sacrificing Wuhan to save the rest of the world is pretty poignant, and partly true; they did buy a lot of time. And cruachanmor describes the ways the Chinese quarantine can basically be called a success:
The fact is that the Chinese efforts at containment do seem to have worked – cases have been dropping consistently now for nearly a couple of weeks. Back in the first week of February the Chinese were diagnosing between 3,000 and 4,000 cases a day (and that was lab diagnosis only) on an alarmingly upward trend, yesterday there were just 415 (lab+clinical), all but 17 in Hubei, with 600 or so suspected (which follows a similar pattern). That’s really quite remarkable – and despite the common internet belief that China is lying through it’s teeth that’s unlikely because more open societies like Singapore and Thailand have followed similar patterns. If there were a more widespread infection then this wouldn’t be the pattern. Indeed at this point the stats would suggest there’s now significantly less people in China with an active infection than there was two weeks ago – this is not “dubious efficacy and inherent harms of China’s historically unprecedented crackdown.” – well that is unless the only thing you care about is the amount of product coming out of Chinese factories.
Whilst the virus may now be in more countries, epidemiologicaly there’s little difference between spreading around the world and spreading in China – which does after all contain 20% of the world population.
Of course that’s not to say we won’t see a pandemic, but The Atlantic is way off on this. In the UK for instance a 40% infection rate with a 2% death rate would be half a million dead. If any democratic government threw up it’s hands and took the ‘fuck it, we’ll let it burn through’ approach suggested by the Atlantic whilst at the same time China does manage to contain it then said elected government is not going to be elected long.
No country that has to respond to the concerns of its citizens (and that includes China where the CCP needs to retain legitimacy) is going to let this go. Even Iran, as there’s a lot of pent up discontent by the younger generation there who are not going to look kindly on their government after a major epidemic.
The story I’m hearing from most smart people is that China has done amazing work and mostly halted their epidemic. This is very impressive, but it’s unclear what it will achieve long-term; they’ve basically turned off their whole country, and they’re going to have to turn it on again sometime. Once that happens, the coronavirus can just pick up where it left off, either from a few people in Wuhan who they missed, or from foreign travelers. I guess they’re gambling they can put out every fire as soon as it starts using the logistical capacity they built for Wuhan, and maybe they’re even right. Nobody’s too optimistic that democratic countries can follow their lead, though.
No problem so bad overregulation can’t make it worse
So far the government has bungled its coronavirus response pretty egregiously.
Most hospitals have the equipment in house to detect coronavirus. But the FDA banned them from using it. They said all coronavirus tests needed FDA approval, and refused to approve anything except the official test made by the CDC.
Unfortunately, the official CDC test was defective. The test itself worked, but one component in the test kit was broken. Most hospitals had their own supply of this component and could have substituted it in, but the way the FDA approved the CDC test banned them from doing this.
The CDC tried as hard as it could to fix their broken tests quickly, but they weren’t able to do it fast enough to satisfy demand. In order to ration the scarce tests, they mandated that hospitals only test people who had recently been to China, or been in close contact with someone who had.
This was a disaster. For example, here’s a story from a person who traveled to Japan, where the coronavirus is active. He came back to the US, started developing symptoms, and went to a hospital. The hospital said since he hadn’t been to China, they couldn’t test him, and sent him home (he voluntarily quarantined after discharge, so thanks).
But even worse, the policy ruled out by fiat ever being able to detect when the epidemic spread to the US. So in mid-February, when a patient with no history of travel to China came to a hospital in California with coronavirus symptoms, the doctors had to ask the CDC for special permission to test. The CDC dithered for four days before granting the permission, during which nobody put any work into containing the disease. Finally the test came back positive – after some health workers had already been infected.
There were many points where this could have been avoided. A better CDC could have made tests that worked from the beginning, or ramped up production of working tests faster, or come up with smarter criteria for rationing tests. But it would have been even better to have a system where things don’t have to go perfectly, and where a few mistakes don’t choke up the entire response to an epidemic for weeks. If we hadn’t let our culture reach the point where governments ban things by default and review at leisure, and where individual iniative is frowned upon in favor of waiting for official permission to do the right thing, we could have recovered from all of these mistakes. Hospitals would have used their existing tests which they already have more than enough of, doctors would have had permission to test suspicious cases at their discretion, and we would have had a chance to catch infections early before they could spread. If the government didn’t already regulate adrenaline, buspirone, insulin, and genetic testing to the point of near-unavailability, maybe people would have thought it was weirder, or raised more of a fuss, when they started doing it for coronavirus tests.
If you don’t trust me, trust former FDA director Scott Gottleib, who explains the situation here in an unusually candid communication from an ex-government official talking about his former agency. His Twitter feed is a great source of information in general.
And here’s a more careful analysis of some of the laws around diagnostic testing and how they contributed to the current crisis. And by more careful, I mean it ends with “Bottom line: the FDA is going to kill us all”.
The efficient market hypothesis is the real victim
I know a bunch of people who sold or shorted stocks when the virus started hitting China hard, based on the assumption that a pandemic sounded bad for business and business hadn’t priced this in yet. Jacob of Putanumonit and Wei Dai on Less Wrong both mention doing this and making healthy amounts of money. Good work on their part – though given the recent market crash, trying to replicate their success now seems suspiciously like a buy high, sell low strategy.
Masks and respirators
People are coming down really hard against face masks for coronavirus. Wirecutter: You Don’t Need A Face Mask For Coronavirus> Marketwatch: US Health Officials Say Americans Shouldn’t Wear Face Masks To Prevent Coronavirus – Here Are Three Other Reasons Not To Wear One. Fastcompany: Five Reasons Not To Wear A Surgical Mask To Stop Coronavirus (number five is “Just don’t.”) The CDC and Department of Health and Human Services have both officially recommended against mask-wearing.
Some of the reasons given are idiotic: the virus is not common in the US yet, so you are wrong to worry. This reminds me of all the people saying that AIs are not currently superintelligent, so any discussion that AIs might become superintelligent is just fearmongering. Who are these people? How are they still alive? How do they avoid driving off cliffs? They’re heading towards the cliff face, and their passengers scream at them: “YOU’RE DRIVING TOWARDS A CLIFF!”. And they calmly respond with “We are not falling off the cliff yet, we’re on perfectly level ground, there’s no reason to panic.”
Other reasons are superficially better, but collapse under scrutiny. Masks, the articles say, only help people who are sick avoid transmitting the disease, so healthy people don’t need to wear them. But the coronavirus can be asymptomatic for weeks, so if you want contagious people to wear them, part of your target demographic will think they’re healthy. Also, if you become sick, you don’t want to have to go out to the store to buy a mask or wait for it to arrive from Amazon, you want to have it immediately.
Other reasons make more sense. Standard-issue surgical masks may not help much, especially if you aren’t trained in their use. The coronavirus isn’t airborne; wearing a mask while walking outside is unnecessary – it’s when you’re kissing your spouse or chatting around the water cooler or touching a doorknob that you really want to worry. Any mask weak enough to stay comfortable while wearing for long periods, or even weak enough to talk through, is probably too weak to work. There’s a good NYT article about some of these issues here. If people with masks risk compensate even a few percent, that’s enough to make them a net negative.
And other reasons are really truly excellent: if random people buy up all the masks, there won’t be enough left for health care workers or the very sick. I agree this one is a good point.
But the thing is, I already own a P100 respirator. I bought it during fire season last year, aka the-air-is-unbreathable season. Living in California is full of excitement, and after a couple of years you end up prepared for lots of stuff. And the other day, I wore it on the BART – a densely-packed subway full of people who are constantly breathing in your face. And my friends told me – haven’t you heard that the government says masks don’t work?
An N, P, or R rated respirator, worn properly, in specific high risk situations, can be an appropriate part of a safety strategy. I think an accurate treatment of the topic would admit this, while also stressing the reasons most masks might not appropriate for most people in most situations. The statements and articles I’ve read don’t seem up to this level of subtlety. Instead, they seem focused on getting people to do what they consider the right thing (not hoard masks and panic) at the cost of oversimplifying the situation, sometimes up to the point of mistruth.
Their goal is understandable, and maybe this kind of simple messaging is the right choice during a pandemic. But the thing is, I doubt any government preparedness czar called up the major media companies and started their pitch with “I’m going to ask you to make an unprecedented sacrifice today”. I doubt there were hours of soul-searching in newrooms and government PR departments as people considered whether to take this step. I think this happened instantly and seamlessly because it’s what everybody has been doing all the time for years.
So no, don’t use masks or respirators unless you know what you’re doing and are sure it isn’t inconveniencing anyone else. But also, try to pay attention to the forces shaping your informational environment.
(update: South Korea is going full speed in the other direction and making it a top priority to give everybody masks. See the Reddit thread about it here. I hope someone compares results once this is all over).
Zinc
There are a couple of compounds that probably help a little against the common cold. Some cold viruses are coronaviruses, and lots of respiratory infections share common mechanisms. Could these be helpful against coronavirus too?
For example, most studies suggest that zinc probably shortens the duration of cold symptoms by 25 – 50%. The studies didn’t really look at severity, but plausibly it affects that too. It’s unclear exactly how it works, but some people think it inhibits viral replication. It also might be involved in immune system function, and there’s some growing evidence that adequate zinc levels prevent pneumonia.
None of this evidence is great. And even if it were, there’s no guarantee it would transfer to coronavirus. Taking zinc to help coronavirus is a really long shot.
Still, it’s weird how explicitly anti-zinc a lot of sources are. Consumer Reports gives 6 reasons (why are these things always six?) that you shouldn’t use zinc for a cold – number one is because, although it will shorten the cold, it won’t prevent it entirely. That’s some galaxy-brain-level reasoning there. Wall Street Journal just warns people that zinc is not known to prevent coronavirus and so you should wash your hands instead, and the Telegraph warns about zinc in the context of scam coronavirus cures we should watch out for.
Again, I understand the impetus. Maybe people are morons, and if you say there’s a chance zinc might be helpful, they’ll go out, down a whole bottle of zinc pills, and then fly to Wuhan and gorge on batburgers because they think they’re invincible. Then when they get it anyway they’ll blame it on you. And there are so many scammers selling so many dumb supplements that it feels irresponsible to do anything which might aid or abet them. There’s no good way of saying “maybe there’s a 10%-20% chance, with lots of Knightian uncertainty, that zinc could make your coronavirus case a little less severe, but zinc pills are cheap and safe, so you might want to try it as long as you stick to safe levels”.
But again, I can’t help feeling like my information environment is being optimized to prevent stupid people from panicking, and not to help me make good decisions. I would love if the average news site I went to had an interview with an immunologist who gave their honest probability estimate for whether zinc would be helpful or not. In the real world, all we can do is make dumb guesses on our own.
Edit: knzhou has better information on this, including a microbiologist’s opinion.
Metaculus is optimistic
Metaculus is a prediction engine run by some cool people at UC Santa Cruz. It crowdsources predictions made in different ways, then studies various algorithms for aggregating them together. Unlike PredictIt, which is almost useless for anything outside the presidential primaries and Trump’s tweeting habits, Metaculus is doing a great job covering the coronavirus epidemic and the questions that are important to me (sometimes too good – I wasn’t expecting them to tell me how likely is is that the Effective Altruism Global conference next month gets cancelled).
As of me writing this they’re estimating that coronavirus kills 140,000 people worldwide in 2020 (25th percentile estimate is 33,000, 75th percentile estimate is 1,100,000). This confuses me – the flu kills a few hundred thouasnd people yearly, so the site seems to think COVID-19 will be less bad than an average flu season. Maybe they expect that people will demand higher standards of evidence in attributing a death to the coronavirus than people have making wild guesses about how many people die of the flu? Or maybe they predict a very high chance it stays contained?
Updates
The best source for continuing information about the progress of the epidemic is the Johns Hopkins coronavirus dashboard. And feel free to use the comments here to share any other information or questions you might have.
















Chloroquine treats SARS-coronavirus in newborn mice and in-vitro. It may be effective in humans for Coronavirus-2 as well.
For more reading:
“Chloroquine is a potent inhibitor of SARS coronavirus infection and spread”: https://virologyj.biomedcentral.com/articles/10.1186/1743-422X-2-69
“Antiviral Activity of Chloroquine against Human Coronavirus OC43 Infection in Newborn Mice”: https://aac.asm.org/content/53/8/3416
“The Management of Coronavirus Infections with Particular Reference to SARS”: https://academic.oup.com/jac/article/62/3/437/734735https://academic.oup.com/jac/article/62/3/437/734735
China might come out looking pretty good in the eyes of its population, which is the main thing the leadership cares about. Report depressed numbers now and only start reporting the real numbers when the whole world is reporting large numbers of cases, at which time the real numbers will look small.
If we have outbreaks in Korea, Japan, Italy, the US, how likely is it India, Indonesia, Nigeria, Brazil have escaped contamination?
Also estimates are hundreds of cases in Bejing before word got out. My bet is this is was a goner from the start. At best China manages to have the lowest infection rate of all countries… which could be perceived as a huge win… even at the cost of a worldwide recession.
That depends on the durability of Coronavirus to heat. Most such viruses are very weak to heat, which is why “Cold and flu season” is a thing.
For example, Thailand’s anti-coronavirus response has been garbage, but since it’s Thailand, they’re not experiencing the kind of rate increase China did.
Possible, though the high rate of infection in Iran (or even South Korea) leaves a lot of questions about India, at the very least.
The average daily high temperature in Qom and Daegu in February are 14 °C and 8 °C respectively.
In Qom in February, the mean temperature is apparently 7.1 °C. Iran’s on a plateau so I would imagine it can get fairly cool in the winter.
The myth of ‘dodgy Chinese stats’ was started by the folks who have annually predicted the collapse of China’s economy. They had to say something to cover their embarrassment, after all.
China has been gathering and analyzing stats for at least 2200 years and the Chinese people are both smart and highly numerate. They notice stuff like that and complain loudly if the see it.
There is not, to my knowledge, a single PRC stat that has proven false or misleading and specialists who make their living studying them, like Carsten Holz at HKU, say that they are, by far, the most reliable source of information about what’s going on in China.
“Running with Scissors” episode title on the remnant with jonah goldberg had a good china expert from AEI breaking down how the chinese lie about basically all their macroeconomic growth statistics. Would recommend listening if you want to get a full picture.
In terms of specific errors, I would point you to the unbelievably low correlation between what China claims is its electricity usage and its measures of output (number of factories, economic growth numbers, etc which are all inflated and smoothed out over time)
Ah, Jonah Goldberg. A titan of impartiality towards antagonist nations.
I feel like this isn’t a particularly great response to another person presenting information. Obviously he believes the information is credible, and just sneering about it isn’t a great way to facillitate discussion, so the intent seems to be shutting down conversation or starting an argument.
If at time t you have n confirmed cases, then even by the most conservative models you have at least 3n nonsymptomatic/undetected cases. Combined income with the fact that health care capacity limited the number of possible detections, the conclusion is that the trend of the number of Wuhan cases doesn’t make sense.
It’s the same for the estimated hundreds of Beijing cases. Measures weren’t very strict in Bejing initially.
There’s a reason they are reporting detected cases. Likely they are also doing random sampling to determine the effectiveness of the taken measures in reducing the spread. They are not reporting the estimated actual number of cases and I think that’s not accidental.
I hate to keep harping on this, but from my point of view, we’re driving down a nice paved stretch of freeway, and the backseat-drivers are screaming, “LOOK OUT A DRAGON !” I look around and see no dragons, so I calmly shrug and say, “Dragons don’t exist, you know. Also, I don’t see anything resembling one anywhere”. And the answer is, “I saw a cactus, which means we’re in the desert, which means that there are lizards, who will INEVITABLY GROW INTO DRAGONS !!!”. So… I’m just gonna keep driving for now.
I’m definitely amused to observe the behavior on SSC on this topic.
It reminds me of Facebook, just better written.
I’d describe it as the result of a loss of faith in public institutions to deal with a crisis.
Whereas I’ve never had that particular faith, so this is just another thing, no different from any of the other things.
I agree, that is a hilariously bad analogy and weak-manning this point is probably a mistake.
Yeah, weakmanning for a joke is something that only works when your reader not only agrees with your viewpoint but considers it obviously true. Otherwise it comes across as shouting from Mount Stupid. I don’t know how much regular readers swallow the LW dogma, but it’s pretty offputting to a general audience.
@Bugmaster
I’m with you on that. And it’s also generally my take on conversations to do with the extinction of all life on earth as a result of a temperature rise of another zero point five of a degree Celsius. I confess to some straw-manning here, but less than a sane person might think. If the conversation is with someone from extinction rebellion, your analogy really is how it goes.
I agree with you, of course. Global warming won’t end all life on Earth; it won’t even end all human life, and it won’t end human civilization… and it won’t even plunge us into Mad Max times. It will cause a massive economic depression, starvation, social unrest, some degree of technological decline, and further (likely, irreversible) erosion of Western political powers (such as Europe and the USA); plus mass extinction of some marine species. However, all of these effects are relatively mild from the long-term astronomical point of view. If you’re worried about survival of humanity, you can stop worrying (*). On the other hand, if you’re worried about continued human prosperity and advancement, then it might be a good idea to look for solutions now, rather than later.
(*) Well, I mean, you can keep worrying, just not for this specific reason.
I get where some of these come from (though I’m dubious about the starvation thing, but there are two I’m genuinely confused about.
I’m not saying that social unrest can’t lead to loss of technology (it has happened, at least locally), but it seems very unlikely to me given that technological progress is usually rapid in the modern age and we have good information storage/transmission. Unless you’re talking about technology like cars being abandoned, which would be more of a consequence of panicked reaction than of global warming per se.
I’m also not sure where this one comes from. Climate refugees? Europe, the US, and especially Canada are sufficiently far north to benefit compared to the world average in terms of geopolitics. I expect relative US power is likely to continue to decline, but for reasons unrelated to global warming.
Tacit knowledge is a thing, and it is not a thing we are actually good at transmitting to other people except by shared hands-on work. There are things we used to do fifty years ago (e.g. building moon rockets) that we have great difficulty doing now, because even though we still have all the blueprints and other records, we spent a generation not doing that and all the people who used to know how we actually did that are dead.
A sufficiently great catastrophe, and I’m skeptical that global warming would qualify but it conceivably could, might result in our spending a generation or more not doing things far more consequential that building moon rockets, and so not being able to do those things even though we still have all the libraries.
“Building moon rockets” was a highly specialized field that stopped being useful once the government lost interest in beating the Soviets there. Our inability to go there today seems more like a willpower / resource problem than a step backwards in technological ability.
Tribal knowledge loss is a real thing, but NASA had to start from scratch in the 60s too. We’d be starting from a better spot today if we really wanted to go to the moon rather than provide jobs for the most congressional districts.
And anyway we’re pretty good at building smaller rockets and satellites (because that technology stayed useful enough to justify maintaining the skills to do so).
So what is the equivalent technology to “moon rockets” that we’d lose for a long time if a severe economic / climate crisis forced us to shut them down? (Legitimately hard, complex things that require a lot of earned and perishable institutional knowledge but are basically “luxury goods”)
Nuclear plants maybe? Microchip manufacture? Big diesel engines? Some of the 367,000 parts in a Boeing 737, or some of the tools required to make those parts?
Willpower is the cause, actual loss of technological ability is the effect.
If we spend a generation not running chip fabs because the necessary global supply chains are horribly mangled and repurposing legacy chips from e.g. gaming consoles is good enough to meet our immediate local needs, then we’re going to lose the ability to fab chips. And when it comes back, it will come back at the 8086 level, not the Core i9 level.
We’ll learn faster the second time around, I expect.
@Bugmaster
One of us might be missing some irony, and if it’s me, it wouldn’t be the first time.
The starvation thing has a number of problems. During the period that temperatures have risen about one degree, crop yields have increased about 400%. The amount of food available per capita has also increased and (appropriately enough, given this post) there is indeed an epidemic occurring – of obesity. In short, global warming correlates with not-starvation. Do you have a prediction for when this is going to change?
There isn’t even a cactus in the vicinity – only a 200 year old desiccated remnant of something vaguely cactus-like, and you are crying out “Smaug, Smaug, Smaug!”
I didn’t mean global mass starvation (sorry if it came off that way), but rather local phenomena such as the Dust Bowl, the Irish Potato Famine (*), etc. As water becomes more scarce and weather patterns change, some geographical regions will see a greatly diminished food-growing capacity. Again, not a world-ending threat, but a very unpleasant phenomenon.
(*) Yes, I’m aware that it was caused by a fungus, I’m talking strictly in terms of scope.
There are plenty of places that no longer grow any of their own food – they seem to be victims of the obesity epidemic like everywhere else. Food is such a globalized commodity, I think it would take a global food shortage for hunger, let alone starvation to increase rather than continue to decrease.
Obviously I’m pretty sanguine about climate change impacts (tho’ I’m aware that negative surprises are more likely than positive ones) My interest here is in making the connection with a wildly different topic where someone – in this case yourself – is familiar with the experience of hearing from people who have imagined a disastrous future that seems wildly improbable given any trends we have actually measured.
Many people claim that the impacts of extreme weather events will increase. However, in the period of time that temperatures have risen their one degree, extreme weather impacts – by which I mean, specifically, deaths – have fallen by two orders of magnitude! So while newspaper headlines are encouraging dragon-imagining, cactuses have pretty much died out. And from the topic of AI risk, I felt you’d see the similarity..
As weather patterns change, some areas will see benefits and some losses. Is there any reason to expect water in general to become more scarce? Higher global temperatures should mean more evaporation from the ocean, hence more water vapor in the atmosphere — that’s one of the positive feedbacks, water vapor being a greenhouse gas, that pushes climate sensitivity above one.
Further, one of the effects of CO2 fertilization is to reduce water needs for plants, since they can get the carbon they need with less air going through the leaves. Combine that with the sharp increase in yield, about 30% for C3 plants with a doubling of CO2 concentration, and I would expect the average effect to be a substantial increase in food supplies.
@DavidFriedman
I don’t think it is just that more water evaporates from the oceans – warmer air holds more moisture, afaik 7% per degree Celsius. Hence, a warmer world is a wetter one (and why Antarctica is the driest continent)
(some details)
The potato disease outbreak was not limited to Ireland, it was a problem more or less throughout the European countries where the potato had been brought. Yes, the famine was worse in Ireland than in many places, but the scope of the problem should include the forced mass emigration, the spread of typhus and other infections through the ravaged land and other consequences.
Nowadays, about a third of “food and foodstuffs” rots away, which is a big problem. If the rotting gets faster, it will be a disaster (and in warmer and more humid climate it will get faster). I am not a specialist, and I would like to see a good review on how this changed or didn’t change in the last fifty years or so.
Also, if the atmosphere contains more vapour, doesn’t it make transpiration harder for the plant, and infection – easier for a parasite?
@Rm
When you say that a third of food being wasted is a ‘big problem’, do you have something to compare it with? I’m aware that it is a common meme for green-leaning newspapers, but you never hear how much wastage there was in the past. Before refrigeration, freezing, canning etc I think you’ll find that food wastage was far worse.
I’d guess that the figure of a third, if true, is the lowest in the whole history of the planet. It is also primarily explained by the fact that in developed countries food has become so ridiculously cheap that most people simply can’t be bothered to make sure they consume every last scrap of the food they buy.
@ Anteros
It was what our phytopathology course started with, although of course our lecturer is more of an algologist and could have read a newspaper.
From a book summarizing weather records over about a thousand years based on chronicles, it looks like in comparatively recent time wastage (in Russia and likely Europe) had to be 1) more variable due to climate and fewer kinds of crops, 2) worse on average due to less developed storage technologies. On the other hand, what this means remains less clear. Has storage sensu lato plateaued, and how stable it is? And how necessary is overproduction?
But aside from that, I am more interested in other questions like how the balance of heterotrophy to autotrophy will look after the saprophytes’ and parasites’ ranges change. Humanity is just one thing, after all.
@Anteros: I don’t know how accurate those food wastage statistics are, but the problem with wasted food isn’t that we waste more than our ancestors [1], but rather that food production consumes a lot of resources and has a high ecological impact. Reducing food wastage is generally a desirable goal, because it reduces negative externalities without reducing our standard of living (unless taken to extremes, of course).
[1] I’m sure there are some who raise the argument that “we’re less virtuous than people of ye olden times, because we waste so much food”, but that shouldn’t detract from the argument above.
@Adrian
Fair point. I agree that reducing food wastage is a desirable goal, including for the ecological reasons you mention. I’m not optimistic, however, that much change is possible. From farm to consumer all the relevant actors (where they are private entities) are already doing every thing they can to reduce their resource use. But mostly this translates to ‘costs’. And from their point of view there is an optimum amount of food wastage – obscene as that may seem to the environmentally conscious. Increased expenditure on refrigeration could reduce spoilage, but increase overall costs.
To reduce food wastage by consumers what option are available? Publicity campaigns? Infomercials that stress how food beyond ‘best before’ dates are still edible?
Unfortunately, as we become ever richer, and food expenditure falls as a proportion of income, the pressures to avoid wasting food will probably decrease, not increase.
@Anteros: Reducing food subsidies?
I think this is key. People used to patch clothes. Now they throw them away. It’s just not worth the effort when clothes are so cheap.
why would global warming cause ‘erosion of Western political powers (such as Europe and the USA)’? Canada, Sweden, Germany and Poland will all see milder temperatures, longer growing seasons, etc. Why would that lead to erosion of political powers? The US case is a little more complex– bad for Florida and Louisiana, good for the midwest and especially Alaska and the upper midwest, eg Nebraska, North and South Dakota, etc, difficult to call for the southwest– say 50% chance it gets wetter, and maybe a big win, 50% chance it doesn’t get wetter and remains basically desert… Hard to see how any of that is going to lead to erosion of political powers. Unless mass hysteria leads to tearing down fossil fuel power plants and replacing them with wind and solar power. Germany has definitely shot herself in the foot on that one.
I think the point I’m making is different from the one you’re arguing against.
It’s possible that AI will never happen and all concerns about it are stupid, and it could still be true that “we are not in the crisis yet, so we do not need to prepare” is a bad response to “we should prepare for a future crisis”. If you think the crisis will never happen, just say so!
AI is obviously happening right now, and it’s a good thing, because I’m tired of driving my own car to work (I want the car to do it for me). However, there have been no viable indicators that the Singularity would (or even could) ever happen. This is why I compared people who fear it to people who fear dragons due to seeing cacti and inferring lizards who grow into dragons.
I’m not going to say “the [Singularity] crisis will never happen”, because “never” is a long time. There could be some weird inter-Universal quantum fluctuation that sets it off tomorrow (or we could get vacuum collapse, or even aliens or demons from Phobos). However, one problem I see with the UFAI safety community is that they seem to be unable to even conceive of the scenario where “AI FOOM” isn’t a foregone conclusion. Every objection someone raises to their efforts is dismissed by saying, “well, given that the Singularity is inevitable, you’re basically just saying that we don’t need to worry about it in the near future, and that’s dangerously short-sighted”.
By analogy, I used to get the same response from Christians when I’d talk to them about Hell. They’d say, “well, given that God obviously exists and will obviously send you to Hell for sinning, you’re just arguing that Hell isn’t that big of a deal, and that’s dangerously short-sighted”. But no, the existence of God is not obvious to me; quite the opposite !
And my experience is similar when talking about climate change – it doesn’t matter that hunger has decreased, extreme weather impacts plummeted, crop yields increased etc etc – the litany states that climate doom is inevitable because…… dragons everywhere!
At least you know what I’m talking about even if climate dragons to you are real where all the other ones are obviously Illusory!
I think that’s understandable, but at least somewhat unfair. I’m not talking about anything even remotely approaching a climate-based extinction event — just a prolonged economic depression, with all the associated negative consequences. This is a much easier claim to defend than extinction of all life on Earth, or conversion of the Solar System into computronium. For one thing, we’ve definitely seen depressions happen before, so we know they can happen.
Fair enough. I suppose your original contention of a climate induced ‘massive economic depression’ sounds somewhat dragon-esque to me, but I agree it is – to me – more plausible than AI catastrophising.
My view is that “the singularity” is already happening and has been for the last 100 years.
It just occurred to me that when it comes to AI risk, it’s a lot like the climate change debate here, except I’m on the other side! Obviously I think AI is a thing (you’d have to be willfully obtuse to argue otherwise) and that it will continue to improve and continue to cause problems.
I just think that the AI risk scenarios this community loves to talk about are based on science fiction and unjustified by any observed or plausibly extrapolated trends. Sort of like the people who think that climate change will literally lead to human extinction, rather than just make things marginally more unpleasant.
An utterly terrible analogy, because we aren’t saying “cactuses, therefore lizards”, we have directly observed lizards, and we aren’t saying “lizards grow into dragons”, we are saying lizards reproduce until their numbers are such as to be a problem. There’s all sorts of things you could plausibly say (there are few lizards, they are far away, they cannot survive the high summer desert temperatures) but you are not, for some reason, saying them.
Is this a good characterization of AI safety? That already-existing AI will proliferate and we’ll be flooded with AlphaGos and GPT-2s? Because that’s extremely silly. My understanding was that AI safety people are concerned with a future super-AI that is to human intelligence as human intelligence is to ape intelligence. (In which case the analogy holds. We don’t even have lizards, i.e. dumb general AIs, and they may not even be possible because your brain is not a computer. We only have cactuses, i.e. specialized tools that can outperform humans on one or two tasks when put through rigorous and specially designed training.)
That article argues against a claim which is much narrower than your claim: That the human brain can be modelled in the terms of a classical computer with a von-Neumann-style architecture (i.e., a persistent memory, a volatile memory, and a processor which retrieves and stores data from/to them). Specifically, that information is perfectly stored in neurons in the same way that bits are stored in transistors and capacitors.
I haven’t seen such a claim in the last, what, 20 years? So I’m not sure why someone would deem it necessary to write such a long-winded article against it. And, uh, yeah, the brain does store information, but in a compressed and very lossy way, where information can get lost or even altered over time (see the “draw a dollar bill from memory” experiment in the article). And yeah, the brain does process information, just not in the deterministic, repeatable, simple-to-describe way a processor executes a program.
More importantly, the article doesn’t contain a single argument why an AI should be impossible or even unlikely. Just that it probably won’t look like the classic, symbolic AI of ye olden times. Which, again, basically nobody argues for anymore.
My view is that superhuman AI is not only possible, but probably inevitable. But the progression of AI will be a slow process and we probably won’t even recognize “GAI” once we’ve achieved it.
The AI risk scenarios people like to talk about here are more like “random guy summons a demon in their basement one day and fails to say the magic words that stop it from taking over the world.”
The article isn’t arguing against AI — that angle is my addition. It’s arguing that thinking of biological brains as belonging to the same category as computers is wrong. I agree, and a corollary is that thinking of computers as comparable to biological brains is wrong. I see this fallacy all over the place when talking about AI.
Computers are capable of a lot, including things humans can’t do. They’re getting better at solving certain problems because humans are getting better at framing particular problems in computer-solvable terms (or at least computer-approximable terms). But there is no reason to believe that they’re capable of everything a human can do, because they’re a different kind of object. There’s no reason to believe that a paperclip maximizer could convince a human to let it out of the box. There’s no reason to believe that an AI could build another, better AI. There’s no reason to believe that a general AI — that is, an AI with the ability to learn new skills across domains — could exist at all. We don’t even have weak versions of these. The only things we know of that can do these tasks are actual brains. But we may not be able to build a brain out of metal. And if we switch to building meat brains, we may suddenly sacrifice all of the properties of AI that would make it existentially dangerous.
For the record, I believe that
1) GAI is definitely possible but very hard,
2) superhuman AI (as in “more intelligent than the most intelligent humans”) is probably possible,
3) superhuman AI (as in “God-like powers”, as propagated by Yudkowsky et al.) is probably impossible,
4) hard takeoff from AI to superhuman AI within days or even minutes is not just improbable, but laughably implausible, as in “the earth below my feet will split open and swallow me whole” implausible.
That said,
Conversely, there’s no reason to believe they’re not in principle capable of doing anything a human can do (in terms of thinking and communicating digitally – I’m not talking about manipulation of the physical world).
See, and that’s where I think the reasoning shown in the article is misleading. Brains and computers are built very differently, and trying to understand brains in terms of computers doesn’t work (and vice versa), but they both communicate with the outside world, and they process and store information (albeit in very different ways).
Time for a car analogy! In general, cars can do everything horses can do, only better. They can pull things and carry people, but they’re stronger and faster. Sure, they can’t shit on the streets, but we don’t care about that. They can’t live off grass, which can be a disadvantage, but is not relevant to question of which can pull the heavier carriages.
My point is: Yes, computers are built very differently from brains, but that doesn’t necessarily mean that they can’t perform the same tasks as brains.
So, I’m not saying GAI is definitely impossible. I’m just saying it’s not definitely possible. Super-GAI might follow from GAI (depending on the details of how GAI is achieved — it may be that general intelligence is something only achievable through biological means, and that humans are near the limit of biological intelligence) but GAI does not follow from our current understanding of AI or current achievements in it. I’m mainly arguing against the view I typically see from AI safety people that GAI is inevitable.
We only have cactuses. Lizards might exist, but we haven’t seen them yet, so asserting that they must exist is wrong.
Maybe the lizards represent things getting checked onto the list “AI can now do this better than a human” and getting enough lizards like that can be a kind of problem, possibly even a FOOM problem for certain values of this.
I guess I have three reactions to this.
1) Most of the AI safety arguments I have seen are more of the form “Assuming a super-intelligent AI exists, it could do XYZ. Nope, you can’t do anything about it because it’ll outsmart you. We assumed it was super-intelligent, remember?”
2) People are really keen to put things on that list even when they don’t belong. I’m sure some people credit GPT-2 with human-level+ writing, against all evidence.
3) I guess I don’t see the problem. Certainly there’s a danger with humans misusing these specialized tools, that’s even the case today. But I don’t view that as an existential threat nor do I put it in the same category as danger from AI. Clearly the danger here is humans.
Is there any legitimate study comparing COVID-19 with the flu ? I found this article, but I’m not sure how authoritative it is:
https://www.livescience.com/new-coronavirus-compare-with-flu.html
The reason I ask is because it’s starting to look like COVID-19 will become a permanent feature in our environment, just like the flu virus. At the same time, the flu virus has been with us for a long time by now. After a few epidemics that killed a bunch of people — and which could not happen today, AFAIK, due to our generally increased level of medical technology — the flu had pretty much become an unfortunate yet minor annoyance. It can still be deadly to the elderly or the immunocompromised, which really sucks… but… most disesases are deadly to the immunocompromised. And yes, even minor annoyances can kill, and we should work as hard as we can to eliminate as many of them as possible, as part of our overall strategy to prevent death. However, today the flu is not a reason to panic.
If I heard that the flu season was starting, I’d take some precautions, but I wouldn’t head for my bunker in the hills and stay up all night with my trusty shotgun. Is the coronavirus going to be basically the same, or should I start welding riot blades to my car ?
It’ll be like the flu, except with a .2% death rate. Also all the old people will live on reserves
I think you mean 2%, not .2%. Convid is 20 times deadlier than the flu.
.2% for younger demographics, while old people have a much higher rate than 2% according to the chart here
It also seems to spread at least somewhat more easily than the Flu.
According to WHO report, Covid-19 has 3.4% of confirmed cases of death which makes it more deadly than the flue.
I think the problem is that even if the disease itself is similar to the flu, our ability to treat and prevent the flu is much greater than our ability to treat and prevent coronavirus right now. In the long run, maybe we will think of “coronavirus season” the same way we think of flu season. But it could easily have a nastier effect this first time around.
I wouldn’t recommend panicking though. Those nasty effects are more likely to look like businesses/schools closing temporarily and markets suffering than bodies in the street.
Based on Google Trends, there’s already a ‘coronavirus season’. If you restrict the dates to before the current crisis, the axis doesn’t get skewed and you can see coronavirus typically ramps up in early November, but then tapers off mid-March.
Give it two weeks and everyone will be talking about how COVID-19 was overhyped. Then when November hits they’ll be too invested in talking about the recent election to care about the newly-endemic cold virus making the rounds.
“The flu virus”, isn’t a thing. Influenza is caused by a family of viruses, individual members of which come and go. Hence the need for a new vaccination every year, even though the old vaccine provided several years of immunity to the specific (and now very rare) viruses it targeted.
If the flu analogy is correct, and it is at least plausible, then COVID-19 has come and will go and next year we’ll be dealing with a different coronavirus. Just like last year, and probably caring about as little as we did last year because coronaviruses are usually pretty mild.
I don’t think there is yet enough data to make a comparison with a lot of confidence.
You may be right in terms of the virology. I don’t know.
However, the government isn’t ordering the mass shutting down of towns and cities in response to the flu. That in itself is a big worry. Suppose for a moment the coronavirus is completely benign – the restrictions on movement, restrictions on gatherings and likely economic dislocation are extremely worrying need much more preparation than I normally do every winter. I’m making sure I have a good supply of certain goods, not because I’m worried that I’ll die if I go outside, but because I’m worried that I won’t be allowed to go outside, or that the supermarket shelves will be empty if I do.
That’s a pretty big assumption.
I was referring to things like the Spanish Flu epidemic; the outbreak of Cholera; and the Black Death. These were all terrible diseases that killed millions of people, and IMO none of them could kill millions of people today, even if we had no treatments that specifically targeted them. AFAIK even AIDS had been reduced from a guaranteed death sentence to a moderately survivable malady.
Obviously, some new and terrifying disease could appear tomorrow; but, to match the historic death toll of e.g. Cholera, it would have to be significantly more virulent and lethal (assuming that our civilization maintains its current level of technology, of course). This makes the appearance of such diseases (barring deliberate bioengineering by malicious actors) increasingly unlikely (and no, I don’t think COVID-19 counts), though obviously not impossible.
There are all sorts of moving parts to this sort of thing. Let’s look at cholera – there are, in fact, millions of cases annually even now, but the mortality rate is as you say much lower than it would have been historically. How much of that is due to better medical technology specifically, vs. having a basically-sound model of disease propagation rather than ‘I dunno, must be miasma’, vs. sanitation technology like sewage treatment chemicals, vs. sanitation infrastructure like ‘not putting cesspits literally in the basement of your building right next to the well’? Hard to say, and harder to say what happens if there’s a major war or natural disaster or [catastrophe here] which disrupts some or all of that.
You are correct, but I was actually including all those factors (such as “basically-sound model of disease propagation”) into “medical technology”.
I do agree that an additional disaster or catastrophe could greatly exacerbate the spread and lethality of disease; however, I was merely considering the scenario where a new disease arises without any other complicating factors. Obviously, if some new disease arises after some post-apocalyptic nuclear holocaust scenario, things would be very different.
Cholera specifically is a funny case, because it will kill you pretty reliably if untreated, but a very simple treatment regimen cuts the mortality enormously. (The regimen being basically “Drink water. No, more water. Keep drinking water. Drink even more than that. Also, add some sugar and salt to it.”) This isn’t specific to the cholera germ at all; it’s basically just a general-purpose “don’t die of diarrhea” recipe.
Much of our health care is similar supportive stuff, which is widely applicable and has advanced enormously over the past hundred years.
@Dedicating Ruckus – exactly. Cholera is really interesting precisely because it’s less about fancy high-tech medical devices and more about knowing what to do and having the infrastructural capacity to a) do it when needed, and b) keep it from being needed so often as it used to be.
AIDS is an unusually difficult disease, and fortunately COVID 19 doesn’t target the immune system. I have no idea how long it would take to find decent remedies for AIDS if it had first appeared recently.
Scott who are the people who made the table showing death rates? How much shoild we trust those numbers iyo?
I’m also curious if they account for the number of cases that are “silent”. If a significant portion of infected show little/no symptoms, we might be undercounting the number of infected and thus inflating the death rate.
The same is probably true for regular flu, though.
I’ve seen some people quote much lower numbers, but ~0.1% seems to be the standard estimate for seasonal flu mortality. The CDC gives an estimate for seasonal flu mortality in the US on the order of 0.1%, and they seem to make a genuine effort to estimate the true number of cases, rather than just counting diagnoses. There are other reasons to worry that the usual flu comparisons understate how much worse covid-19 might be, but afaict this isn’t one.
For that to be the reason of the trend, the number of undetected cases should be much much higher among old people than among young people, and I can’t think of a reason why it would be.
I can: old people often have all kinds of health issues going on, minor sypmtoms might be overlooked whereas a young person is usually healthy so the contrast is obvious.
I think you have this backwards, but I want to be sure we understand each other – assuming that subclinical cases are significantly more common among the young and otherwise healthy than among the old/immunocompromised (almost certainly true) and that clinical diagnosis is required for identification (true in this case, I believe), why don’t you think that leads to inflated overall mortality estimates?
This is somewhat true for the seasonal flu, but less so because I think those figures are derived from estimated prevalence, not clinical diagnosis counts.
[emphasis added]
It would, but I can’t see why it would lead to more inflated estimates for the elderly than for the young.
I don’t think anybody was saying it would? The points are that the most severe cases are over-represented in official figures, and separately-but-relatedly that the most severe cases are going to be mostly the elderly and/or immunocompromised.
They don’t account for silent cases, but nor do they account for the lag between diagnosis and death. Death takes 2-8 weeks from symptom onset, according to the WHO, whereas by early February lab-confirmed diagnosis was taking about 3 days from onset in non-Wuhan China, about 5 days in Wuhan.
(They also don’t account for the possibility that the death toll is significantly underreported, due in part to early Chinese deaths being attributed simply to ‘pneumonia’.)
If you look at deaths now ÷ cases as of n days ago, where n is an estimate of the average time from diagnosis to death, you get a much higher rate. Likewise if you look at deaths ÷ (deaths + recoveries) — despite the fact that the WHO figures indicate that death takes longer than recovery, skewing this figure downward as well.
Link: https://www.worldometers.info/coronavirus/coronavirus-age-sex-demographics/
I hope I have phrased this non-politically enough – my question is quite narrow:
In UtopiaStan, two factions struggle for control of government. Faction A, which has a competent propaganda machine, is observed to say, “Faction B wants millions of you to die from coronavirus!”
Given that observation, there are multiple plausible causes for it:
1) Faction A just wants to score quick points off faction B, and their action says nothing about their predictions.
2) Faction A actually believes millions may die, and is laying the groundwork for putting blame on faction B.
3) ….
My question: Given what we know about competent propaganda (plus whatever we may guess about politics in UtopiaStan – please do NOT publish your thoughts here), does this one action indicate anything useful about the likelihood that faction A actually expects millions to die? If so, would that tell us anything useful about the actual likelihood of millions dying?
Just on general principles, the answer to “does this one action indicate X” is “no”, regardless of X. You can’t draw meaningful conclusions from one data point.
It’s sad how thoroughly politicized the issue has been. In the beginning it was the left telling us that “it’s just the flu”, in order to criticize the travel ban policy. Currently it’s the right telling us that “it’s just the flu”, in order to defend Trump’s handling of the CDC response. I rarely see pundit opinion flip so seamlessly and so quickly. I have no doubt that if the Trump administration immediately acted extremely aggressively, and we were past this epidemic in two months, the narrative would flip right back — it would then be the left telling us that “it was just the flu”, and any measures taken against it were probably fascist or whatever.
The point is, in our system, literally any result can be politicized. Any policy can be framed as too strong, or too weak, or even both at once by a sufficiently disingenuous pundit. Knowing that one of the two factions is unhappy with a particular result is completely useless knowledge, because this would be true for any result. Ignore this noise and focus on what the actual scientists say.
Here’s an idea. Maybe the “competent propaganda machine” isn’t a propaganda machine at all. Maybe it’s a collection of independently-motivated companies that profit from attention rather than truth, and pandemic narratives get lots and lots of attention. Maybe there’s no conspiracy at all, just capitalism at work.
Here’s another idea. Maybe coronavirus would be of no real concern if handled competently, and people are used to infectious diseases being handled competently. And maybe newly available information has made it worryingly clear that coronavirus is not being handled competently, causing people to update their priors about the threat it poses.
One last idea. Maybe not everything splits cleanly along partisan lines. An issue like coronavirus very likely doesn’t. Maybe “Faction A believes X” and “Faction B believes Y” are meaningless statements on such issues because individual faction members have differing opinions. So that would make your question meaningless as well. (Or if there is an answer, it’s “no and no”.)
This is perhaps focusing on the wrong thing in response to a helpful post about a serious matter, but there’s a typo. Metaculus was founded by people at UC Santa Cruz, there is no University of Santa Cruz.
Square root is way too strong an adjustment for this correlation.
Simple intuitive reasoning: suppose you learn that one person in a household of 5 people has gotten coronavirus. And then you find out that another person in the same household also got coronavirus that same week, not from their housemate. Surprised? I find that pretty surprising, when background rates are 1/800 or less. Surprising as in less than a 10% chance.
But if there’s less than a 10% chance of multiple cases (given one case), that means that the linear estimate is pretty close. In the most extreme plausible adjustment, maybe the 5-person house is effectively a 4.5 person house in terms of how the risk accumulates. That’s much closer to 5 than it is to sqrt(5)=2.23.
Here’s an even more extreme example of correlation. Let’s say that someone shows up at work sick, and now everyone who works at their office each has a 10% chance of getting sick. Let’s say that the 5 housemates all work in the same office, and their entire likelihood of getting sick comes from this scenario. In that case there is a 41% chance that at least 1 of them gets sick (1-.9^5), as opposed to the 50% chance that they’d get if it was linear (5 x 10%). So the 5 person household is effectively a 4.1 person household.
Real correlations are much weaker than that, and so would be such a trivial adjustment from the linear estimate that they’re not worth trying to adjust for.
I’m also skeptical of the square root adjustment. I think the clearest way to think about it is to imagine the entire area is 4 person households – the optimistic scenario says there’s a per-person risk of 1/400k and a per-household risk of 1/200k. That means the average household that has a person getting sick has 2 getting sick, which is bizarre & IMO not believable unless the 20 people getting sick is including within-household transmissions. If the updates come from doubling times I think that would include intra-household transmission, so the 20 “new” cases is really more like 10 new households with 1 person sick & 10 households that already have an infection getting another one. That model feels believable, but suggests that the adjustment isn’t a square root, it’s more like a constant divide by 2 (essentially that you get sick if anyone in your household got sick last time step OR someone in your household becomes sick this time step).
Out-of-household risk of transmission should be basically linear as long as the virus is “sparse” in your demographic. Maybe an adjustment makes sense if you think your household is especially insular (e.g. work in close proximity, commute together, etc), but for something like the most stereotypical american family (2 working parents, 2 non-twins in school) I’d expect the single specific people that the household has contact with outside the home to be diverse enough (individuals, not demographics) that the risk for out-of-household transmission is almost independent.
With “Chinese-American school children in San Mateo” as an example, I estimate there’s ~1.7k of those (100k population, ~8% chinese, ~21% <18 yrs old, per wikipedia). In the optimistic scenario there's 20 sick and the next increment is another 20 getting sick. That's still only about ~3% of demographic is sick – positing the "Chinese-American school children in San Mateo" effect being strong enough sibling exposures imply they both likely get sick if one does contradicts the total demographic only having 3% infection rate. If P(getting sick from outside the household | housemate getting sick) is high because of the demographic, it should be high for everyone in that demographic, meaning the demographic has to be much smaller than “Chinese-American school children in San Mateo”, like “people who work at a 40 person company and eat all their meals together”.
> elderly men seem to have twice the death rate of elderly women
The New York Times has an article about that. One factor is that about half of Chinese men smoke, while only about 2% of Chinese women smoke, so that explains a portion of the virus’s gendered impact. Other factors are that apparently women have stronger immune responses in general, and that Chinese men have higher rates of diabetes and high blood pressure too.
I would imagine the “stronger immune responses in general” is doing most of the work. Having elderly men hit harder is not at all unusual among respiratory diseases.
China has a 4.6 year gender gap in life expectancy, so the average elderly Chinese man is closer to death than the average Chinese woman.
@Aapje
Makes it clear just how much work genetic processes are doing in modern life expectancy if Chinese men absolutely wrecking their bodies compared to women only translates into 4.6 years.
A quick search suggests that the life expectancy loss of smoking is about 10 years. 10/2 = 5, which is close to 4.6.
This is surprisingly “clean”.
I mean a single factor explains almost all of the differences between two populations who should different in multiple ways. (Men usualy also drink more, get more into fights, get more into trafic accidents etc.)
I’m somewhat doubtful whether that 10 year figure is true. But smoking might explain a substantial part of the difference.
Zinc is an interesting and kind of frustrating issue. As you saw, studies generally support the use of zinc for the common cold — and while the evidence isn’t perfect, it’s substantially better than any other purported cold cure.
Here’s what an actual, well-cited pathologist who has worked on coronaviruses has to say:
Personally, zinc has worked fantastically for me. I used to get a cold every other month, and over the course of several years tried tens of random supplements and read hundreds of studies. Now I only use zinc, and I get much fewer colds.
Why doesn’t everybody use zinc lozenges? A variety of factors:
– Most products you find in the pharmacy are marked as “homeopathic”, which sets off people’s antiscientific alarm bells. This is misleading. Homeopaths think the strength of a medicine rises by how many times it’s been diluted, with 30X and higher being the gold standard, but these supplements are prominently marked as “1X” diluted, i.e. basically not diluted at all! Zinc lozenges are about as homeopathic as a standard multivitamin is; the label is only there because it lets them dodge some FDA regulations.
– Ionic zinc (the active ingredient) tastes terrible. It basically removes your senses of taste and smell for a few hours, and leaves a metallic residue on your tongue. Popular brands try to fix this by adding binding agents that lessen the amount of ionic zinc produced, which makes them useless.
– The mechanism of action requires the ionic zinc to be coating the cells it’s acting on. This means that zinc pills don’t work at all, resulting in lots of people wasting their money. I assume this also means that zinc lozenges don’t help for lower respiratory infections (which COVID-19 is), which fits with my anecdotal experience.
– Zinc can have permanent long-term consequences. The FDA warned against zinc nasal sprays for removing some people’s senses of smell. After three years of using zinc lozenges every winter, I feel like my sense of taste has gotten permanently worse, but I can’t know for sure.
In other words, you’re exactly right about why there are so many anti-zinc articles: people have determined that pushing against zinc is the right call on a societal level. Promoting it means increasing societal trust for homeopathy and lowering societal trust in FDA guidelines. But that doesn’t mean that zinc doesn’t work.
I also use Zinc lozenges in the form of zinc acetate when I feel the first symptoms of a cold. For me it works well and while everything tastes bad after using them I do not have the feeling that my sense of taste is deteriorating. But I use them only for one or two days when I feel some symptoms, which is probably only the case 4 to 6 times per winter.
I wonder whether everyone who welds galvanised steel for a living will end up being fine (apart from all the flu-like symptoms of zinc poisoning).
Zinc is known to be toxic to neurons, particularly upon direct exposure, which is why the nasal sprays were so bad (you basically have exposed nerve endings poking out of your cribiform plate). If you’re taking zinc, I’d recommend considering some form of damage to nerves directly exposed to it as a “cost of doing business”; your call on whether that’s an acceptable cost.
A cold every other month is a pretty high frequency. I wonder if over time you became immune to so many strains of cold viruses that what looks like the effectiveness or zinc is more a function of immunity from exposure?
I have found the amount and severity of colds has fallen a lot now I am in my fifties. I have heard this from other people as well. Maybe it is lack of small kids around, maybe I finally developed immunity, or my suspicion is that my immune system is less effective, I believe a lot of cold misery is about the cold virus hijacking your immune system to spread itself via sneezing. If you’re immune system is weaker then it cannot so easily fire it into overdrive. Same with hay fever which has also gone away.
It’s not because you have a weakened immune system, it’s because you’ve built up a lifetime’s worth of antibodies to the numerous cold bugs out there. (I can imagine a hypochondriac seizing on the idea that *not* getting sick means having a weak immune system.)
I absolutely agree that zinc works fantastically against colds, with the caveat that according to a podcast I listened to, only one brand on the market (as of 2016) seemed like it would be expected to work. But that brand does wonders for me. No experience on whether it works for COVID, and I don’t personally know enough to speculate.
The brand in question is “Life Extension Enhanced Zinc Lozenges”. Life Extension does at least one other brand, too, so be careful. I’ve previously written up a LW post with more detail and buying links: https://www.greaterwrong.com/posts/un2fgBad4uqqwm9sH/is-this-info-on-zinc-lozenges-accurate
Might I ask what brand you take? I would expect the Cold-Eeze lozenges recommended above to be ineffective for the reason you cite (adding binding agents that improve the taste but make it ineffective).
(Aside, I misclicked and accidentally reported your comment. Sorry for the false report, Scott.)
I use exactly the same product. I heard that that this form of zinc usage helps against all rhino viruses, so the common cold. This works well for me butI don’t know if any coronaviruses will be affected.
Yeah, I currently use the same. When I was in the UK I used the “Elite Zinc Defence” lozenges from Healthspan.
Thanks! Assuming you mean these things, I don’t see anything in the ingredients list that sounds like they should be ineffective.
I guess either they’re newer than 2016 (oldest review is from two years ago) or the podcast host didn’t find them. (Or maybe they don’t/didn’t ship to the US, or probably a bunch of other explanations.)
They’re also cheaper, so when I run out of my current stocks I might give them a try.
Oh, now that I’ve written this comment, I now think the dose is lower than ideal. “34mg zinc acetate, delivering 10mg active ionic zinc” – but you want 18mg ionic zinc per lozenge. Maybe it’s sufficient to just have many of them.
> I must add, however, that using zinc lozenges as directed by the manufacturer is no guarantee against being infected by the virus, even if it inhibits the viral replication in the nasopharynx.
Do you know what this would mean in terms of outcomes? E.g. something like “helps with some symptoms, but not others”; or “slows progression of the disease but doesn’t particularly change severity”?
How high are the risks of nerve damage from zine? Are we talking about permanent nerve damage?
A year or two ago, I asked a pharmacist whom I know socially about zinc lozenges. His reply was, “Do you play the lottery? How do you know you’re not going to be one of the few guys who never tastes anything again for the rest of his life? Is that really worth having your cold be over with sooner?”
So… homeopathic zinc pills make homeopathic use of homeopathy, where the homeopathy is diluted down to the point where it doesn’t exist? No wonder they’re so effective!
Homeopathic homeopathy!
A doctor I saw seemed to correctly diagnose that I had a (mild) ‘plant’ allergy that’s seemed to have been managed very effectively with generic OTC drugs. Unfortunately, or so I’ve thought until I read your comment, they also gave me a homeopathic ‘drug’. It never occurred to me until now to have checked whether it was a homeopathically homeopathic drug!
Yup!
More specifically, “1X” in homeopathy means a dilution by a factor of 10. (So 30X is dilution by 10^30, which safely leaves no molecules of the medicine at all.) But that’s precisely what you want — it makes no sense to have a lozenge that’s literally just a block of pure zinc.
Similarly, some cold medicines are marketed as “2X” homeopathic, which means the active ingredient is at most 1% of the mass, which is again what you want anyway.
Another ‘homeopathic’ remedy that has actual functional levels of an active ingredient is Hyland’s Teething Gel. Granted, exposing your infants to highly dilute solutions of tropane alkaloids is a little dodgy, but I will say that it seems to work.
Honestly, at this point I’m seriously considering just making my own zinc acetate supply.
Stick some galvanised nails in a cocktail shaker and make a $spirit sour.
Gargle it and you get both zinc citrate and ethanol to kill virii.
I think the point of the article linked above by @philh is that any kind of zinc salt other than acetate or gluconate is unlikely to be effective, and acetic acid is far easier to source than gluconic acid.
Disclaimer: If zinc works for you, by all means, stick with it (ceteris paribus). Also, of course, given somewhat conflicting evidence of its effectiveness, it’s probably worth it to keep experimenting with it.
That said, focusing time and effort on things like zinc seems like a TWUD to me–time wasted on useless details.
a) The overwhelming likelihood is that if you get a cold, you’ll feel bad for a little while and then it will go away in time.
b) Take some NSAIDs and/or pseudoephedrine so you can feel good while you’re getting better.
c) Spend less time thinking about zinc and prevention. There’s probably a pretty good-sized nocebo effect if you constantly catastrophize about “maybe I’m getting sick/hope I’m not.”
Uh, sorry, the government pseudobanned pseudoephederine too.
Take it anyway; a “pseudoban” isn’t actually a ban.
If I have to provide ID and put my name in a little book which waives my Fourth Amendment rights for an indeterminate period of time to get the stuff, it’s as good as a ban. Especially since my house is packed with “drug paraphenalia” such as torches, digital scales, and plastic funnels, which they can get me on when they don’t find any meth.
It’s actually not too hard to make sudafed from reagents that are widely available across the US. (Hai, Hakkenshit 2011)
Lambert:
If I’m worried enough about getting raided by overzealous drug warriors to avoid buying sudafed, I suspect cooking up sudafed in my kitchen isn’t a strategy to lower that risk….
@Albatross: You seem to have skipped the step where you read the abstract Lambert linked to. You really want to go back and do that. Trust me.
There’s not really any need to carry out that synthesis; one of the precursors is a fine decongestant all on its own.
But you need to watch out for the side effects, such as “the urge to be successful in business or finance.”
Arggh! Should have followed the link!
Here’s a trial where zinc acetate did not help: https://bmjopen.bmj.com/content/10/1/e031662
I believe the lozenges they used make this mistake:
> Popular brands try to fix this by adding binding agents that lessen the amount of ionic zinc produced, which makes them useless.
It says they use orange flavours, and this suggests that may be octyl acetate. From my link above, anything ending “-ate” or “-ic acid” (other than stearate or apparently stearic acid) is bad news.
They also violate “dissolve in mouth 20-30 minutes” and probably[1] “18mg zinc per lozenge”. Granted, I don’t remember the podcast I used as a source being clear on why those were necessary; couldn’t you just take more lozenges to compensate? Plausibly, “high zinc levels for a short time” could be less effective than “moderate levels for a long time” in the relevant tissues, but that’s mostly a guess. But in any case, it looks like they didn’t in fact take enough lozenges to compensate for the dose; table 4 compares their trial to 8 others and shows they have the lowest dose and the least effect. (That table only includes positive-effect trials, so it doesn’t by itself show the effect is real; but I think it does show a plausible reason why, stipulating that the effect is real, this study may have been unable to find it.)
[1] I’m not 100% on that one. The brand I have says 18.75mg “zinc (as zinc acetate)”, and these were 13mg “elemental zinc”. It may be that what you need is 18mg zinc acetate to provide (what I think would be) around 6mg elemental zinc, in which case 13mg elemental would be more than enough. But my read, especially given table 4, is that you need 18mg elemental zinc, and my brand provides that through (what I think would be) around 56mg of zinc acetate. Listening to the podcast again my provide clarification.
Yes. This is undeniable.
People who say that China completely fakes its numbers don’t get how exponential growth works. It’s very easy to fake daily numbers, but it’s impossible to fake a trend. Infection numbers were going up by about 25% per day before late Jan/early Feb, then started plateauing.
Can the numbers in China be off by a factor of 2? Yes, of course, it’d be impossible to tell.
Can the daily growth numbers be consistently off by 25 percentage points for over a month? No, that’s impossible. Over time, the difference between the true numbers and the real ones would become several orders of magnitude (25% per day over 30 days = 800x; over 60 days = 652,230x).
We do have some “measurement devices” that are independent of the CCP. They are noisy and cannot tell the difference between 300 (the reported number in Shanghai) or 600 cases, but if there were 240,000 cases in Shanghai (800 x 300, circa 1% of the population; and trending up), “we” would know about it.
Exactly! I’ve been trying to make this point in various places for a month and continually being called a CCP shill for it (despite being an American citizen — turns out it’s transmitted genetically). The WHO visited China to verify the numbers and is of course in complete agreement with us, but all social media mentions of the WHO denounce them as… CCP shills!
I am perfectly confident that when the dust settles, none of the currently wrong people will have changed their minds. Nationalistic instincts go in, incorrect statements come out, no processing occurs in between.
I think this is borderline possible, but only in the direction that’s good; i.e. the disease is less infectious than thought because the reported numbers started off orders of magnitude lower than the real ones, but are now basically right. Imagine the spread started earlier than reported and the initial case numbers were deflated. Then over the course of a month the reported numbers (which started out low too low) catch up to the real numbers. It’s much easier to think/pretend 800 cases are actually 40 than 400k cases are actually 80k and there’s even perfectly ordinary and innocuous reasons to suspect that would happen (e.g. at the beginning only the worst 1% of cases are identified and now it’s more like 20%).
Thanks for writing this. I also live in the bay area, and I’ve done my own analysis outside of the rationalsphere, and came to mostly the same conclusions, so its good to have independent verification.
By the way, if you have a Samsung Galaxy phone, it has a built in pulse oximeter. Could be useful in a pinch.
I’m incredibly sad over the senseless deaths that will come in the next few weeks to months. Why did Western world ignore China and not learn from their mistakes? Why didn’t we start preparing sooner? Why aren’t we starting strict quarantine protocols?
I think there are pros and cons to the Chinese approach to the problem. On the one hand, putting the entire country on lockdown and throwing people in jail at the first sign of a cough is, indeed, a very effective way to stop the spread of disease. On the other hand, I worry about living in a country where the government is fully empowered to lock down the country and throw me in jail at the slightest provocation. There are tradeoffs involved, and I think it’s worth our time to look at the whole picture before committing to a course of action.
It’s always been that way.
The CDC’s handling of the test kits is not a commercial for the idea that our competent government agencies will exercise these powers in sensible and effective ways.
> On the other hand, I worry about living in a country where the government is fully empowered to lock down the country and throw me in jail at the slightest provocation. There
I think this is a strawman. What I meant here is that we could learn from China’s strengths (distributing masks, shutting down schools/offices quickly) and their mistakes (locking people and silencing them).
Sorry, I misinterpreted “their” in “their mistakes” to refer to the Western nations. I thought you were saying, “the Western nations chose to avoid the kind of draconian measures that were implemented in China; this was a mistake” — but it looks like you were not saying that, so I apologize for inadvertently strawmanning you.
living in a country where the government is fully empowered to lock down the country and throw me in jail at the slightest provocation?
Erm, their unarmed cops have better things to do that throw people in jail. Their incarceration rate is one-fourth ours and their rules about police behavior are much stricter than ours.
> ‘we’re all safe until the next time some moron in China eats a bat.
>and then fly to Wuhan and gorge on batburgers because they think they’re invincible.
Heads up, I know people take Scott’s word as gospel (I love his writing, too) but this isn’t confirmed – it’s just one of the many hypothesis out there.
>> ‘The efficient market hypothesis is the real victim’
Two people make a tiny bit of money on a temporary crash, and people really start updating as if that’s something they haven’t seen before? This should literally be almost no evidence for anything if you’ve looked at the market before – neither for or against EMH.
The evidence that it’s Zoonotic is pretty damned good.
The chances that it’s from bats is pretty high since the closest genetic match is a bat virus.
Inducing zoonotic transmission is a known method for making a pathogen more virulent.
That being said, cross species transmission is rare enough that you’re way better off rolling around in a pile of bats than getting coughed on by one infected human.
Other coronaviruses have come from bats by way of an intermediate host. In this case, the culprit is currently believed to be pangolins, since there is a very similar pangolin coronavirus. There’s also a pretty plausible method of transmission, since pangolins are commonly poached and consumed.
Glad that there is still good news in such a troubled time.
Three people (myself included). And while I only made about $3000 it seems like other people made more. (I closed my position too early, before the full extent of the crash – if I had waited a few more days I could have made $20000.)
Agreed, the EMH works for long terms trends, not short term. If those same people sold everytime there were early signs of a pandemic of similar scope, they would likely lose money. They just made the right short term bet.
I’m hoping that was a joke on Scott’s part. The EMH does not exclude the possibility of a few people on occasion getting lucky with positive returns from market timing.
Given that Eliezer was making very serious tweets that other people were taking seriously, the default assumption should be that it isn’t a joke.
The blow to the EMH is that bond yields started falling in earnest in mid January and gold started a bounce off the bottom sometime in Jan as well. Two major markets started flashing red 5 weeks before the equity markets caught on.
I thought the EMH bit was weird too, especially Eliezer’s tweet* (unless he was joking?). If your uncle Harry has a hunch that AAPL is going up because he really loves his new iPhone, and then AAPL stock goes up, that means…absolutely nothing. By this definition, tens of millions of people ‘beat’ the market every single day.
The distinction is having some edge that allows you to beat the market consistently over time (or at least make one enormous, spectacular Soros-style trade).
Most edges (exploitable anomalies) disappear as soon as they become publicised, which is the wildest thing about the EMH: rather than punching holes in it, every valid criticism of the theory makes it even stronger.
Edges that still work include ‘hedge funds which employ armies of drones to survey Walmart parking lots’, ‘being golfing buddies with the chairman of Big Company X’, etc. These are valid ways to beat the market, because they involve information asymmetries, and are included in the strong form of the EMH.
The argument here is that there’s an edge along the lines of ‘non-domain experts can use rationality skills to make better predictions than the biggest and most accurate prediction machine ever invented’.
It’s neat that Jacob and Wei Dai made money, but I think it’s dangerous to encourage this line of thinking. Honestly, this is one of the rare times when ‘if you’re so smart, why aren’t you rich?’ really does apply. There are legions of really, really smart people who a) live and breathe as professional investors, and b) have genuine information asymmetries to exploit, and they still don’t do all that well.
(If rationalists start their own hedge fund and become fabulously rich, I would love to be wrong!)
*jarring because EY’s writings on the EMH are v. insightful and well-explained.
No, this is just a tautological definition of the EMH, if I found a way to beat the market’s returns and no one else ever did, I would eventually accrue enough wealth that my action in the market would close the edge of and you would get to say ‘see, the EMH is true, baconbits9 no longer beats the market… eventually’.
The EMH says nothing about the edge being publicized, even for the weak EMH, only that the information used to create the method has to be publicly available for the weak EMH, and available for someone for the strong EMH.
No, that’s not my ‘definition’ of the EMH – I agree with you! We know it’s possible to beat the market; there’s a history of anomalies and maybe even some that still work or are yet to be discovered.
To rephrase my statement more carefully: “rather than punching holes in it, every valid criticism of the theory makes it even [more difficult to beat the market].”
In the old days you could run simple algorithms like Munger and Buffett-style value investing; now you have to do increasingly crazy things like send an army of drones out to survey Walmart parking lots.
The point I was making is that claiming to be able to beat the market is an extraordinary claim that requires extraordinary evidence: say, becoming fabulously rich, or making consistently high returns over many years or decades. Making one good trade, or even a handful of trades, just doesn’t mean anything in particular.
More broadly: there are many cognitive biases that nudge us towards thinking we’re special enough to beat the market, and rationalists are probably even more susceptible to them.
(I, too, think I’m special, and have allocated some play money for trying to beat the market! I am fully aware that this is silly, and that if I succeed, my ‘cunning strategies’ will almost certainly boil down to random good fortune.)
> More broadly: there are many cognitive biases that nudge us towards thinking we’re special enough to beat the market, and rationalists are probably even more susceptible to them.
See also: Scott’s implicit shilling of cryptocurrencies when asking “why didn’t rationalists get rich off the crypto boom?” Which is a bit like asking “why didn’t rationalists get rich off lotto tickets in Vegas last weekend”
The real evidence against (the strong form of) the EMH is stuff like the TWTRQ fiasco.
Of course, while markets aren’t literally perfect, they’re efficient enough that no ordinary person can reasonably expect to make much money on average, which is about the same thing for practical purposes.
The average person can’t beat the market because if they could they are by definition not average or all market returns will increase to that level. The EMH does not say ‘average people can’t beat the market’ which is bland and carries no information. The EMH is specifically about how new information spreads through markets, not about if average people can all somehow have above average returns.
On prepping in areas where there is likely to be nontrivial number of undiagnosed cases already – which is, many European cities, since people returning from northern Italy are being tested positive left and right, so we have to work under an, um, discardable, assumption that Italian outbreak is way more widespread than diagnosed numbers suggest:
I am not sure whether it is a good idea if everyone goes to the supermarkets (or chain stores or whatever are those called in the US), in order to buy up monthly supply, before proper social distancing etiquette is established.
Stores will get overcrowded. Or more overcrowded than usual.
Another South Korean cult?
Most of the death rates that people quote are nonsense, because they are calculated by dividing deaths by total cases, ignoring the fact that (according to the WHO) death takes 2-8 weeks from symptom onset, whereas diagnosis is much quicker than that. Hopefully there are more than enough undiagnosed mild cases to offset this (though I don’t know how confident we can be of that yet, given that deaths in China have probably also been underreported), and hopefully the rest of the world will have much better outcomes than Wuhan. But a lot of people are treating the current deaths ÷ cases figure as a ceiling, and revising it down based on the reasons for optimism, when they should be starting with a much higher figure before doing that.
+1 Just wanted to comment with the same. I still believe the uncertainty around “current deaths ÷ cases” is _mostly_ downward, but this is an important point.
FWIW, based on Wikipedia numbers as of right now, deaths_so_far/(deaths_so_far + recoveries_so_far) is 6% in mainland China and 19% elsewhere, though that most likely underestimate the ultimate fatality rates in places where the epidemic hasn’t peaked yet.
I think that’s backwards–it takes longer to recover than to die from the disease, so as long as cases are increasing, the death rate should be artificially high, not artificially low. And also confounded by the fact that so many mild cases are undetected, where as we have (not great, but better than this) decent measurements of overall flu prevalence.
That’s what I thought too, but the WHO report says otherwise. From page 14:
They classify about 80% of cases as ‘mild to moderate’, so these numbers almost certainly imply a shorter average time to recovery than to death.
Can’t seem to edit, but I just want to note some ambiguity: does the 2 week median include all the cases they elsewhere describe as ‘mild to moderate’, or are they deliberately leaving ‘moderate’ cases out of these recovery figures for some reason? (‘Moderate’ seems to mean relatively mild pneumonia, whereas ‘mild’ seems to mean non-pneumonia.)
Immediately before giving the 80% figure (on page 12), they say “Most people infected with COVID-19 virus have mild disease and recover.” So even if moderate cases are missing from the time-to-recovery numbers, they’re probably not numerous enough to matter too much in this context.
Secondly, 3-6 weeks looks like a range, but the grammar of that sentence makes it a median — do they mean that? If so, should we interpret 2-8 weeks as another ‘median’, even though it doesn’t seem to be presented as such?
Again, however this should be resolved, I can’t really see it affecting our question too much. But I want to be careful not to make unstated assumptions.
I meant overestimate not underestimate, sorry
I don’t think so. At the time, nobody knew (except maybe a few health professionals) whether the epidemic would be contained, like SARS and MERS were, or not. Some people bet on it spreading and others bet on it not spreading. One successful or unsuccessful bet is not a basis for disproving the efficient market hypothesis.
Did all the people out the market get back in before today’s rise? If not they could be missing out forever on a five or six percent of their investment. Also the idea that one good call disproves the efficient market theory is crazy. Every day people correctly choose the winners in horse races, doesn’t mean tomorrow they won’t lose. Investment is a game of averages not single events.
Thanks for this genuninely helpful public service announcement. Not that I wish it longer, but would it make sense to address Vitamin C? That also seems to be making the rounds. The below is taken from an email forwarded to me:
From Lynne McTaggart, author and health lecturer (read to end):
Last weekend, we held our Get Well Health Expo at Olympia. Thousands came to meet the many dozens of pioneering doctors and therapists of all varieties that we had carefully selected to offer alternative solutions proven to work.
Of nearly 50 brilliant talks and demonstrations, two delivered by Dr. Damien Downing, a pioneer in ecological medicine and president of the British Society of Allergy and Environmental Medicine, and Dr. Thomas Levy, a cardiologist and one of the world’s experts on vitamin C, offered the same message: there is a simple solution to the coronavirus, which has gripped the world in fear.
Dr Downing was one of a team of orthomolecular doctors (who offer therapeutic nutrition based on biochemical individuality) to put together an effective plan of attack for the coronavirus.
He and the others released a statement in late January by the Orthomolecular Medicine News Service to say that the coronavirus pandemic ‘can be dramatically slowed, or stopped with the immediate widespread use of high doses of vitamin C.’
This is nothing new. A raft of studies carried out in the 40s and 50s showed that very high dose vitamin C, particularly given intravenously, could stop the deadliest of infections, including polio.
Dr. Frederick Klenner was one of the pioneering doctors in the 1940s who successfully cured many viral diseases, from flu and hepatitis, to viral pneumonia and even polio using very high doses of vitamin C, anywhere from 30,000 – 200,000 mg, given as divided dosages throughout the day with no ill effects.
More recently, a 1999 study of 700 students with cold and flu symptoms compared one group, which just received the usual cold and flu drugs, against another, which received hourly doses of 1 g of vitamin C. The researchers discovered that symptoms decreased by 85 percent in the group treated with vitamin C. As the researchers concluded: ‘Vitamin C in mega doses administered before or after the appearance of cold and flu symptoms relieved and prevented the symptoms in the test population compared with the control group.’
Alan Smith is a recent case showing the power of this simple and inexpensive supplement.
In July 2009, Smith’s life hung in precarious balance. A farmer in New Zealand, Smith had come down with a severe form of swine flu and was deteriorating rapidly. Doctors at Tauranga Hospital induced a coma, then transferred him to Auckland Hospital, where he was put on specialized life-support equipment.
X-rays showed that his lungs were completely clouded with fluid – among the worst his doctors had ever seen. They then discovered that Smith also had hairy-cell leukaemia, but he still had a chance at survival if he could recover any lung function at all. However, in his present condition, the Auckland doctors told his wife Sonia that he was not likely to survive and recommended turning off his life-support.
Smith’s brother-in-law, however, refused to accept this death sentence and insisted that he be given intravenous (iv) vitamin C. To humor the family, the skeptical doctors agreed to administer 25 g/day of vitamin C for several days. By the end of the second day, however, new X-rays showed large air pockets in Smith’s lungs. His lung function had so dramatically improved that he was able to come off the life-support system.
Nevertheless, the doctors refused to acknowledge vitamin C as the source of the improvement and so stopped the IV drip, after which Smith rapidly deteriorated. But, at his family’s insistence, the doctors eventually gave Smith a far lower dose- 1 g of vitamin C twice a day; he began to improve, albeit much more slowly.
After a move to another hospital, he regained consciousness and his vitamin C regimen was stopped permanently.
Sonia Smith then decided to give her husband a new form of vitamin C, touted as being as powerful as IV dosing, called liposomal vitamin C. Smith’s recovery was dramatic.
Although doctors believed he would need three months of hospitalization for rehabilitation, he walked out of the hospital after two weeks. By the time he was released, he also had no signs of leukaemia.
Dr Downing and other physicians from the International Society for Orthomolecular Medicine urged preventive supplementation to ‘prevent or minimize symptoms for future viral infection,’ including the coronavirus.
These include:
Vitamin C: 3000 mg daily, in divided dosages
Vitamin D3: 2000 IUs daily (Start with 5000 IU/day for two weeks, then reduce to 2000 IU
Magnesium: 400 mg daily (in citrate, malate, chelate, or chloride form)
Zinc: 20 mg daily
Selenium: 100 mcg (micrograms) daily
As vitamin C champion Dr. Robert Cathcart once noted, ‘I have not seen any flu yet that was not cured or markedly ameliorated by massive doses of vitamin C.’
So stop panicking about the so-called pandemic and start this simple prevention program.
Vitamin C megadosaging is not supported by science.
I knew the grandfather of Vitamin C megadosing, Linus Pauling, who told me why it is officially considered ineffectual. One of the ugliest scientific stories ever told.
The reason is quite simple: studies have repeatedly failed to find it to have any positive effect. The vitamin C pushers claim success, but replications fail.
Is the punchline that he was wrong in an ugly way, or that the truth was suppressed over his version in an ugly way?
So, tell us.
>Alan Smith is a recent case…
n=1
“Orthomolecular doctors” are not actual doctors. The entire thing is an altmed scam.
technically Damien Downing is a qualified medical doctor, qualified in 1972. He’s just super into a lot of quacky stuff.
https://www.gmc-uk.org/doctors/1559976
Damien Downing also an “electrosenesitivity” believer and sells “chelation therapy” to treat autism.
There is no crisis so grave that someone won’t find a way to make a quick buck from it.
Shocking to me as a GIS educated person, why do the official COVID-19 media have such dreadfully bad GIS maps?
Just look at the map on the Johns Hopkins coronavirus dashboard. Zoom to east asia:
Why is the dot over Hubei the same size as the one over Korea? 67.000 cases are not the same as 5.000 cases. Neither are 935 in Jianxi.
If you are going to use graphical representation, why not choose a format that graphically represents the actual numbers?
And that is the central information site world-wide.
Problems like that abound: Look at the animation DER SPIEGEL puts in all its COVID-19 articles, e.g. https://www.spiegel.de/politik/ausland/coronavirus-fordert-bislang-mehr-als-1600-todesopfer-in-china-a-ae76de96-f5c3-40f4-858a-3e7a6238675a#.
The dot for the number of deaths is the same size as the dot for number of infected in Hubei?
Did everyone die? No, but let’s represent “3 %” as “100 %”, to make it easier to understand for people who do not like numbers.
My (strong) impression was that the maximum size of the dot is constrained to that associated with around 1500 cases.
Not exactly a fan of this for couple of reasons:
1. The Johns Hopkins coronavirus dashboard you linked too, far as I can tell, although this reads live data, it was built in late January, and the way it displays data is not exactly reflective of the way people are tracking the outbreak right now. It also is red on a black background, and has large alraming fonts. Might I suggest the WHO’s situation dashboard instead?
2. This post feels, and I’m sorry I don’t have a better word for it, selfish? Look, most of what you’ve written about here reads like a “beat the market be smarter than the masses mentality” which, well, is right but also, COVID-19 is a community problem, not a personal one. Yes, prepping increases your chances of survival, but that is true of virtually every disaster, prepping will help you survive anything, but we aren’t going to turn billions of people into preppers ovenight. Our solutions for improving outcomes should focus on community engagement, not secretly hoarding canned goods and N95 masks.
3. There is a lot of misinformation out there, and as you metioned there is plenty of misinformation about misinformation, ideally, if the rationalist community is as it porports to be, this is a community uniquely prepared to help sort and disseminate reliable, useful information, not back of the envelope calculations about the current state of the virus in the bay area. Yes, this isn’t as exciting, because the best information comes from government agencies and is technically avaliable, and no one is likely to rediscover the wheel, but things are getting nuts when it comes to misinformation, plenty of it btw floating about in the rationalist community. Let’s focus on how to help the community, as the most effective way to fight COVID-19 seems to be “follow the standard containment protocol being esposed by your local government” and maybe as a secondary objective make sure that the information that those orgs are putting out is actually correct.
On your 2: first, “community engagement” is nice and all, but it’s vague to the point of nonactionable, probably something you can’t do on your own, and most people ought to be limiting nonessential “engagement”. Prepping you can do effectively for yourself.
Second, prepping isn’t selfish. Unless you’re hoarding so much you are preventing lots of other people from having supplies, prep is good for the community. You get your supplies now, before lines are too strained, and don’t have to participate in the panic later (if it ever comes). Most importantly, successful preppers are self sufficient. So they won’t be using up scarce emergency resources, those resources can be focused on people who couldn’t prepare, and most importantly the prepped won’t be going out looking for supplies and becoming a vector themselves.
Many people prepping now means increasing demand now. I would be interested to see numbers how fast supply can be ramped up in order to meet this increased demand. If it happens slowly, substantial prepping might indeed prevent lots of other people from having supplies later on.
Also increasing demand means rising prices which would hit poorer countries.
Community engagement is not at all vague and none-specific, just diffrent from the immediatly obvious tasks of posting and replying to blog posts and reddit threads.
– Read and stay up to date about reliable informations sources regarding the outbreak. Yes this includes the boring ones, how many people in your community are scientificly literate enough, and have enough of a ressitence to “boring” scientific papers to correctly digest them. As a “rationalist” you should have the tools to do exactly this, to digest the information and pass it on to the concerned people around you who don’t have the tools to do so.
– Keep up to date with the status of the outbreak where you live. The situation changes quickly, and local news tends to report suspected cases, rarely correcting later for how many of those suspected were actually infected. This sometimes gives the impression that the outbreak is much worse where you live.
– Talk to the people around you about the outbreak and strive to correct missinformation, and discourage panic and speculation. People have a tendancy for paranoid rumination, be CBT about it, encourage people to find more efficiant thoughts about the crisis. IE regularly checking local health agencies for infortmation, if they are scientificly literate, point them to more direct sources of infromation, encourage personal hygine typical viral season.
– Encourage people not to distribute misinformation in channels you are a part of. Your uncle reposts a chain-forwarded whatsapp message to your family’s whatsapp group? Tell them to stop, explain to them if you have the time / courage (damn it can get tiring to argue with uncles).
– Encourage humane thinking about infected individuals, remember how sometimes even hospitals treat aids patients like they aren’t just infectious but instead radioactive? Those are medically trained profesionals, and they still lose sight of themselves sometimes. Your aunt Dorothy doesn’t understand why not all suspected cases of infection are hermetically sealed, try to explain to her about how these are people, and that there are concrete steps that can be taken to reduce infection without violating human rights, that are virtually as effective (especially if you live in a country only a limited outbreak / imported cases only).
– If you know about your country’s containment strategy, explain it to people. These steps are often invisible. Understand how the current global containment strategy works, follow its failures and be ready to discuss them and explain them rationally, things that haven’t worked haven’t worked for concrete reasons, not because the outbreak is an amorphous super force of destruction.
– The current strategy is dynamic. It will change, some recommendations will become more severe, some lesss. To people that aren’t following very closely this will appear fllippant, be ready to disscuss how if the strategy was static, it would fail as soon as something went wrong, changes aren’t arbitrary.
– Be ready to put statistics that appear terryfing in context. Encourage calm preperadness, but prepare people that there is a real possibility for sevre disruptions to civil life in the case of a local outbreak. Explain that even in China, these disturbances have been temporary / are expected to be.
– Suggest setting up channels to distribute this sort of information in your workplace, if they don’t already have one, forward matirials to your HR department from your local governing body that relate to workplaces.
As for prepping, it can be argued that prepping ahead of time can be great for raising your own chances of survival, but in the middle of a crisis? At best all your prepping work (and online disscussions focused on the best ways to prep for the outbreak) will take your time and attention away from helping and strengthening your community, at worst your last minute bulk orders of essetials will divert resources away from the proffesionals that need them to deal with the crisis.
I’ve seen posts by people explaining how to get their hands on drugs that are supposed to help treat the virus (which btw, is a supposition not yet a scientific fact), how to order them in bulk, and how to massage the truth to get the sellers to prioritize sending them to you. This doesn’t just hurt demand for the drug incase it formalizes into a first line treatment of the virus, but reduces stocks for people being treated with it for the desiase it is actually proven to help fight.
This seems like a false dichotomy. You don’t have to choose between preparing yourself and your household versus keeping up on the news and educating others. Yes, these things take time, but most of us have enough spare leisure that we can do both.
It really rubs me the wrong way to see people attempting to protect themselves decried as “selfish.” First, because there’s nothing unethical about Scott’s suggestions (you speculate some people might be doing unethical things, but that’s another topic), and second, because in this as in every situation I can only control what I do. Giving up on what is within your power to focus on trying to control other people’s actions, which are not in your power, is wrongheaded.
Not control but help. There are originizational steps you can take to ready your community.
Just as prepping is not equivelent to selfishly hoarding, being involved in your community is not equivelent to forcing your opinion on others.
Now this is far more anecdotal than anything else, but I have personally seen far more evangelical guides to prepping on rationalist forums, then steps to help make sure your community is better prepared for a local outbreak.
@TJ Michael But everything you’re talking about relies on convincing others. You can’t control whether others accept or believe info you give them. I’m not saying you shouldn’t try, but focus first on what is in your control.
@caryatis obviously I can’t control what others think, I’m not psychic.
But I can try and correct people when they spread misinformation, and suggest diffrent ideas about what they can do. Isn’t that what spreading ideas is all about? I’m saying if you can do that, do that. If you don’t want to do that, don’t. Sure I think I might have an opinion about what you end up doing, but you can’t exactly expect me not to anymore than I can expect to be able to force you to think what I want.
I can’t imagine that there are many people in the rationalist (or rat-adjacent) communities that need encouraged to argue with people who are wrong. We’re heavily selected for people who answer when duty calls.
(or if so many people are prepping at the same time that they end up infecting each other in the supermarket)
@TJ Michael
Note that both the Johns Hopkins and WHO dashboard’s are lagging by at least 6 hours when it comes to the latest information we get. If it lags for a relatively well-managed country like The Netherlands, it probably lags a lot more for other countries.
Actually think that it’s a good thing it lags, this isn’t a zombie epidimic, real time is really only useful for healthcare proffesionals where you live.
I’m assuming part of the reason it’s lagging is to reduce the occurence of noise from false alarms.
They actually did subtract one case today. A small kid was faking it to not have to go to school (not really).
John Hopkins updated to new obsolete data now, BTW, while the WHO has a double obsolete figure, still.
I like the Worldometer page for coronavirus.
You currently have three groups of people:
1. Those doing nothing at all.
2. Those acting to help themselves.
3. Those acting to help others.
Group 1 is the large majority of the population, group 2. is smaller, group 3. is even smaller. I don’t get focusing ire on group 2. as if they are worse than group 1. But if your goal is just virtue-signaling you’ll have a receptive audience in group 1., who want to validate their decision not to do anything.
What?
Look, man, this outbreak is scary stuff, it’s real anxiety inducing for people.
I know that I’m the rumminate and obssess over things type, and it’s part of the reason I end up on these sorts of sites. I also know that if you’re that sort of rumminating-obssesing type I am, you end up sometimes with these optimization traps, looking for the best way to prepare for the outbreak.
Sometimes it feels like a superpower, but also other times, there’s a tendency to look inward towards that group, and echo around this optimization seeking pattern, untill slowly the data inside that group is just built up so much from the optimization disscussion, that there’s no oxygen left for anything else.
Lately whenever I’ve looked at these spaces, I’ve seen the COVID-19 disscussion dominated by the prepping angle. And look, it’s healthy to do some level of preperation for any disaster, but infection is a community issue, you can isolate yourself completly from that community and hyper optimize your own survival strategy, you could, and maybe you could even do that without hurting others, but also maybe use that superpower to help others, to talk to the people around you and help them optimize their own strategy, help your community strengthen its response to the outbreak. Infections are a heard thing, and although intellecually I know I often feel my heard is online, when it comes to viral infection, it’s the people physically around me that matter most.
Now, granted, this is me projecting, this is me using those empathic parts of my brain to try to understand why others are hyper-focusing on prepping when the rational part of me doesn’t see the value in doing so to such a degree, and so it’s projecting my own patterns of rummination and obbsession to fill that hole.
Now you could argue that’s self serving, some twisted need for me to correct others as over-compensation for the fact that before I found balance with my own rumminations and obbsessive tendancies I really blew it, and I really had to hit rock bottom to get out, so now I try to win that time back by helping others, even if I have to invent the congruence between myself and these internet people to make that happen.
Now, that’s the self critical angle I use when I try to examine why I’m doing this, I don’t really see “virtue signaling” as being part of it.
It’s a contagious disease. Helping oneself, to reduce one’s chance of illness, is helping others. Masks to reduce one’s spread of it is helping others. Prepping so one can quarantine oneself is helping others. Meanwhile it’s not clear what “community engagement” is or how it would help. I’m guessing you mean, like, getting information out there to warn others to do these things? That would indeed help… but it’s exactly what this post is doing! So what are you complaining about? That the post doesn’t say “also you should tell this to other people too”?
Btw do you have a site that tracks cases with any greater precision than country? The site you linked seems to be useless for e.g. tracking its geographic spread within the US…
I am afraid that you are mistaken, setting aside innocuous measures like washing hands. Buying up scarce medical supplies makes them harder to access for others. Loading up on nonperishable food is also questionable as it encourages runs on the stores where there might be transmision of a disease due to overcrowding.
Its far better to run on stores now while few(er) people have the virus than wait until many people have it.
Sure, but no runs would be even better.
If there are no runs then companies that make products have no incentive to increase production. Runs and price spikes are what allow you to know there are shortages and a need of increasing supply.
There’s a circularity here. I feel like from a practical perspective that you are asking people to co-operate with defectors. If I don’t buy nonperishable food and then others do so, I may go without food if others clear the shelves. Yes, that very thinking is what causes the process, but I’d really be taking a big gamble to count on others to co-operate without any way to coordinate that co-operation.
It’s a coordination problem that can’t be solved by asking people to co-operate. You’d have to actually enforce it by rationing shopping runs, so that each person can only take a certain amount. Even then, that assumes there is enough for everyone if we portion it out evenly. If the necessary period of quarantine is for months, then there might not be enough available stock in stores to evenly divide that. In that case, without the actual material assurance, it really is everyone for himself.
I think that you are mistaken, at least in a mild situation like that (risk that things will go so bad that food supply will be interrupted is imho low and many of those who will go sick will hopefully be able to get food from deliveries by their friends, family, etc.). There was or is a mild shopping run here (Prague), but many people did not participate. I bought only a package of tissues and more tea than usual. Meme that shoppers are panicking and shouldn’t do that appears to be partially successful, although the store where I was buying normal things was more overcrowded than usual and coughing people did not adhere to any social distancing etiquette, which was uncomfortable.
Masks, on the other hand, are mostly gone from pharmacies for weeks and some enterprising individuals got to selling them on the secondary market for a hefty premium (note: I did not see anyone actually wearing a mask so far).
And one online retailer had impose rationing, since few people were trying to buy huge quantities of food, emptying its storage facilities.
I go to the grocery store about once a week anyway. (I don’t think this is unusual?) If I selfishly decide to “prep” for coronavirus by buying, say, more dried beans than I otherwise would on my next trip, I have a hard time seeing how that increases the risk of disease transmission compared to just doing my normal shopping.
Yeah, I am not in a position to judge anyone, I did that too. I am concerned by people trying to buy months worth supply of nonperishable food at once, since if everyone would do that, more cases of infected people are all but guaranteed, at least here.
Is anyone encouraging people to buy months worth of food at once? The Kelsey Piper article Scott linked talks about preparing for “a few weeks,” and encourages people to “slowly start to stock up.” Even the “really intense guide by a professional prepper” says your goal is to “stock up slowly by grabbing extra each time you go out,” and lists the most important goal as having “two weeks” worth of food (though admittedly he says 90 days is even better).
There are almost no reasons for not having 10-15 days worth of food in your house anyway. That is like 10 boxes of pasta an a jar of oil per person, or a 10lb bag of rice + oil. Obviously you don’t want just rice and oil, but it costs very little and takes up little space to have that on hand.
This is what we’ve done too and what I’ve seen public health officials recommending. It’s perfectly fine to gradually build up some shelf-stable supplies and to make sure you’ve got enough Tylenol etc in the house.
People who have the funds to lay in some goods can also give money to community agencies so they’ll have some funds to help people who don’t have money to lay in extra supplies.
There’s no “perfect” way to do this. There’s just taking reasonable precautions and helping your community take reasonable precautions for people who may be more vulnerable than you.
Wish I did, didn’t even notice that, I live outside the US so I’m just used to not having higher resolution geographic data.
Actually followed up with a pretty big reply about this for someone who had a similiar note.
Ah, oh well.
Actually reading this, I still don’t think the complaint makes sense? This is for several reasons.
The first is largely what I already said above. Basically your “community engagement” is essentially, tell people things. OK. Tell them what? What’s the payload? Scott is in fact just one more person getting information out there.
But, OK, you don’t want Scott to just tell people things, you want Scott to tell other people that they should be telling people things. But like… does this need to be said? The new coronavirus is the talk fricking everywhere as I can see. You don’t need to tell people to share what they know, everyone’s constantly doing it.
Towards the end of your post you suggest that there’s a tradeoff here, that time spent prepping takes away from discussion. You say:
But… no… discussion is constant. It just keeps fricking going. Talking is a free action, as they say. Maybe not if you’re writing whole long blog posts or doing lots of serious investigation of primary sources. But most of the time, there’s not any significant tradeoff here.
Looking again at the bit I quoted, it takes us back to the original issue — what’s the payload? Strenghtening the community how? By spreading information, apparently. And like, presumably that means actionable information. Actionable information like… on how to prepare? Like, it’s not clear to me what the community being “strong” is supposed to mean in this context — the context of resisting the new coronavirus — if not, y’know, actually being prepared for it!
But, OK. Part of what’s going on here seems to be that you seem to have a very different model of people’s living situations than I do. Now obviously all this is going to vary heavily — but that’s part of my point, it is going to vary heavily and you can’t just assume your picture applies.
Basically, when you say, “the community”, I say, “what community”?
Now I’ve a lived a lot in big co-ops houses in Ann Arbor. So if I were living there, I guess that would be “the community”. Right now I live in the Solarium in New York, basically the hub of the local LW meetup group, so I guess that whole group is the community, although I can assure you they’re already discussing this stuff endlessly on their mailing list, I don’t think I need to add anything.
But who was “the community” when I was living in an apartment by myself in Madison where I knew hardly anyone and barely saw the few I did? Other than the internet, since that apparently doesn’t count, even though for lots of people, the people they know on the internet are much more their community than anyone they know IRL?
Like, you seem to have some assumption that the people you’re talkingto live in something that can be reasonably called a “community” — and not an online one! I… don’t see that as being the case. Lots of people just live, y’know, alone, or with a few roommates, or with a nuclear family; and they may have friends over fairly often but they don’t have regular scheduled meetups or anything.
But, OK, maybe, even if there’s no big co-op house or regularly scheduled meetups, these groups of friends are still “the community”. But this brings us to another problem — you not only have a pretty specific idea that people live in these communities, but of what the other people in these communities are like. Because you actually do have a suggestion for the payload — why it’s supposed to exclude advice on how to prepare I don’t know, but I guess I already covered that above, so let’s move on — but it’s targeted towards a fairly specific sort of person.
I mean, as I already said, I live in the Solarium; “the community” is the local LW meetup group. Now when I lived in the co-ops in Ann Arbor — basically living with a bunch of random undergrads for the most part (though no uncles there) — yeah, maybe there’d be something to the picture you paint. (Although there, it’s likely an emergency house meeting would be called to discuss the situation, which brings me back to the point above about this not being some separate thing that needs doing. Also probably the food stewards would be prepping on behalf of the house although that then raises question of the budget but I guess the house might have to approve that anyway and uhhhhh I think I’m going off topic.) But when people choose who they hang around with, they’re largely going to hang around with people like themselves, not the paranoid, panicky, and essentialist people you depict. I mean, you use the example of aunts and uncles. Those… aren’t people I regularly talk to… they’re people I see on holidays… they’re certainly not part of “the community”.
So, sure — if you live in a community, and it’s not a community of people similar to you but rather a random assortment containing a bunch of people who are paranoid, panicky, and essentialist, then you would likely want to spread the information that you describe… except, as I said above, this is presumably something you’d already be doing just in talking about this as normal, and there’s no reason for this to exclude information about actually preparing.
(You actually don’t entirely exclude this — like when you mention,
Yeah, that right there — those concrete steps? What those are is actually important!)
There’s one more point I want to make, which… this is something I avoided commenting on on your original comment, but, the whole bit about, follow your local government’s recommendations, I have to point out, that only applies if you live in a country whose government is actually trying to stop the spread of the new coronavirus. Unfortunately, a lot of us live in the US, where the federal government is run by one Donald Trump, who cares about appearances, not reality, and is working to hamstring the CDC’s ability to get accurate information out there — you know, attempting to hide how bad things are rather than fix things. Now state governments can likely provide better info! But my point is just, y’know, before listening to the government, make sure it’s a government that is actually trying to solve the problem rather than fudge the numbers.
(Serious question: Is there in fact more to the plans than just what’s repeated over and over — avoid crowded places and gatherings, wash your hands, don’t touch your face, etc., etc.? I guess this is going to vary by country…)
I can’t really give an example for you, as you seem to be US based, but say if you lived in Israel where I do it would be something along the lines of:
– Stay up to date with the Ministry of Health’s most up to date guidelines.
– The Ministry of Health regularly updates whenever someone that was confirmed to be infected had contact with people, keep up to date that you might not have been exposed.
– Make sure to be strict with yourself regarding personal hygine.
– There is no current uncontrolled chain of infection in Israel, the reason that there was a recent spike in infections in our geographic area has to do with an outbreak in Italy, this outbreak is believed to have been caused by the rare appearance of an infectious and asymptomatic carier, this is expected to be very rare.
– I usually suggest a source like the WHO’s daily situation reports to track the desiase, if their current source of news is facebook, or some other unreliable source.
– I try to explain what diffrent measures mean and what they are likely to lead to. Why the most extreme measures aren’t used in every case.
That’s just off the top of my head, I usually try to respond to the concerns of those around me, and try to focus the data I gather on that.
That’s true, I’m speaking as someone who lives in an urban area, with social circle that isn’t limited to online interactions, with lots of coworkers, and close family I see atleast once a week.
You are entirly correct that if someone doesn’t have a community, there’s no point in diverting one’s own resources to help it. My base assumption then is that you are part of some social community in your immediate physical space.
I’m starting to see I’m on a diffrent frequency here, and that I may be misunderstanding people. I’m reffering to prepping, not preparing.
To me “Prepping” is creating a long term agile strategy to deal with massive civil disturbance. “Prepping” is a long term thing, and trying to fit that into the timeline we’re dealing with on COVID-19 would involve diverting resources, and would take up a significant amount of your time.
In my mind the diffrence between that, and “preparing”, is that preparing for COVID-19 is something you should definetly be doing.
IE I see “being ready for the complete long term collapse of civil infrastructure” as diffrent from “having two weeks food supply on hand”.
I really haven’t been clear about the diffrence, but what I am trying to get across is that there is a point in optimizing your own survival strategy, where if you are too inward looking the latter can become the former, and that those extra energies can defenietly be redirected elsewere.
Great point, look, I’m usually used to being on the other end of the stick here, all of us in the rest of the world with people in the US assuming that we have the same mindset / problems / infrastructure that you have to being with.
I can just say I had assumed that Trump wouldn’t be interfering so heavly with the CDC’s ability to operate in this situation, I’m sorry to hear that’s not the case.
When it comes to politics we’ve been a bit distracted here in Israel by our own elections which took place earlier week.
I guess with your examples, like, that’s sort of the level 0 stuff. It’s the sort of thing I’m assuming everyone is already keeping track of! If someone doesn’t know, sure, tell them, but, again, that doesn’t really seem like the sort of thing that needs to be specified — people are already talking about this constantly. Like I said, no real tradeoff here.
The “urban area” part sticks out to me here as odd; if anything urban areas are known for fostering less close social ties, not more? I thought you were going to use a small town as your example! I hear, from people who have lived in them, that they’re much more everyone-knows-everyone. But none of this is really that relevant…
I see. Do you have any actual disagreement with the Scott’s original post then? Barring one stray reference to months of quarantine (which doesn’t sound like it’s meant as advice), it seems to me that everything he’s advocating would fall under what you call “preparing” rather than “prepping”. Like he said: Electricity’s probably not going to go, water’s probably not going to go… I’m puzzled as to where your disagreement is then.
Oh yeah, it’s a real shitshow here in terms of the response. The organized response may as well not exist. Hopefully there can be widespread testing soon? Hopefully? (And while the CDC has bungled things due to Trump’s interference, the FDA, as Scott has discussed above, managed to bungle things all on their own…)
Anyway, hope things stay OK out in Israel…
@Sniffnoy
Unfortounatley this has not been, and continues not to be, my expiriance.
Particularly regarding paranoia about potentially infected. I wish I had a source in english for this, but when things started getting bad in Korea, the Israeli government decided to round up all Korean tourists and ship them back. While that may be justified, the way they were treated was as if they were radiocative, so much so that the Korean government complained to Israel through it’s diplomatic channels.
Now that there are more poeple getting quarantined here who are Israeli, and the more people that get infected, I’m seeing the same sentiments regarding their treatment.
In addition, each time measures become more sever or the outbreak gets worse, there’s a noticeable uptick in peoples distrust of the containment effort.
It’s much harder (again in my urban environment) to practice social distancing, I depened on public transport, and am rarely far enough from any one person so that if they caughed I wouldn’t be in the “droplet zone”. While I can’t effect these people, my hope is that the more people try to distribute good information, the more likely the people around me are to be better informed.
I’m still not a fan of the self survival optimizing angle (although I am very supportive of the elderly relative notes, theres some very concerning data regarding the elederly, and while I hope there’s some other explanation regarding the higher death rates, its something that bears repeating), I wish Scott had taken the time a bit to step out of that disscussion to discuss the nature of that disscussion, I’m not a fan of the some the back of the envelope math he uses [even if on reddit he responed to me with a link to some better data] as I don’t think we need back of the envelope math to rediscover what’s already being published by groups like the WHO, but again if like your saying whichever relevent agency is really dropping the ball in his area, might actually be more appropriate than I originally thought, overall I found the tone a bit severe which feels like it could just fuel the self optimizing angel.
Re: betting markets – the CDC estimates “151,700-575,400 people worldwide died from [2009’s H1N1 outbreak]”. See here. My sense is that people under-reacted to that event – 20% of the world was infected!
Re: best source of information – I find I prefer worldometers.info for news and stats. Watch the Active Cases!
Correction: the “Age Distribution of Hospitalizations” isn’t “rate of hospitalisation by age”, as wrongly stated in the paragraph above. It’s “hospitalised cases carved up by age brackets”. (The paragraph below treats the graph correctly for the purposes of an inference, so it’s just an issue of phrasing.)
This. I was very confused when the graph seemed to imply that over half of people in the younger age bracket need to get hospitalized.
Thanks for this, Scott. Very useful information.
But that’s flu + middling precautions vs. covid-19 + extreme measures (quarantines, travel bans, etc).
Another factor could be that COVID-19 started only after half of the flu season was already over and in an unusually warm winter. If we get a warm spring, too, COVID-19 season might be over before massive death tolls. On the other hand, it will most likely come back in autumn.
Nope; assuming any of the several etiologies of the form ‘something really weird happened in Wuhan’ is true, there’s no particular reason to think this will persist substantially. One imagines the Chinese will come down hard on bat-eating/improper specimen disposal/bioweapons research security breaches/whatever going forwards – if the virus doesn’t mutate such that in can easily infect humans from whatever animal reservoir population it has/may have/the Chinese don’t exterminate, of course.
I’m not sure if I understand your point. Are you saying that the virus won’t come back in autumn because the jump from bats to humans won’t happen again in autumn?
If yes, I don’t think that’s the likely path of recurrance in the first place. Other pathogenes like influenza don’t jump from animals to humans every season either and I don’t see a compelling reason why the mechanism by which they persist shouldn’t be useable by the new coronavirus.
As John Schilling pointed out above, influenza isn’t the same virus recurring every year.
There will be a coronavirus next Winter, ~99.99999% confidence, but ‘a coronavirus’ is just a fancy term for ‘the common cold.’
This specific coronvirus does not appear to have entered the human population in an easily-repeatable way; my understanding is that it’s something like wildly improper specimen disposal but I’m not sure. Therefore, once the current outbreak (burns itself out/is stamped out, assign percentages as you like), there’s no particular reason to expect it to come back seasonally. The annual flu is thousands of individual virii with various reservoirs reservoirs, so that does come back every year; this is more like, say, polio, where something weird has to happen for it to get it wide circulation again.
It won’t burn out if reinfection rates are sufficient, or it mutates fast enough.
If it mutates, then the mutant versions almost certainly just become one more brand of the Common Cold.
True, but my understanding is that they’re not and it isn’t likely to, respectively – cf. the Chinese infection curve already starting to level off and the discussion elsewhere in this thread about this virus being fairly stable.
EDIT: @Lambert
On the “if it mutates” question, something that I’ve been wondering about for a while—will COVID-19++ be about as deadly as this one, or about as deadly as the common cold?
@ Nick
At this point, I think the best answer anybody can give is ¯\_(ツ)_/¯
@Nick
Have you seen the speed of John Schilling’s thinking today? He answered your question 7 minutes before you asked it.
What’s the actual difference between a deadly coronavirus and a common cold?
Is it raw replication rate or something?
What are the evolutionary pressures going on?
@Lambert, anecodotally, from Chinese relatives and friends, it’s more accurate to call it pneumonia, as it’s called “Wuhan Pneumonia” in Chinese.
So 80% of the time the virus will give you more mild non-pneumonia symptoms, and 20% of the time you’ll get pneumonia, which has a good chance of killing you if you’re old and/or a smoker…not sure why kiddos have dodged it though.
But like, why does it sometimes badly infect the lungs and sometimes not?
Why do some deseases cause pneumonia more often than others?
What are the selective pressures towards higher and lower lethality?
@DragonMilk: The WHO says 80% of lab-confirmed cases are ‘mild to moderate’, which includes people with relatively mild pneumonia. They give their criteria for ‘severe’ and ‘critical’ in some detail:
I think the 80% includes ongoing cases (at the time the report was written) whose symptoms may have since become severe or critical.
@Statismagician:
Why is this important? I don’t think nCov needs to re-enter the human population if it becomes widespread enough. Or do we have evidence that the waves and seasons of all the common viral infections in humans are mainly due to interspecies transmission? My prior on this is quite low.
@paragonal_
No, the large set of virii we call ‘the seasonal flu’ have their reservoir in humans, plus various bird and other animal species for particular strains of particular virii.
There are tens of millions of cases of ‘the seasonal flu’ annually, in the US alone, conservatively. That’s the kind of coverage you need to get seasonality, not a hundred-some-odd-thousand extremely concentrated cases under immense scrutiny from the entire world public health establishment.
@Statismagician:
Ok, so your basically assume that the virus isn’t going to infect 10%+ of the world population in the current wave and that this is a requirement for seasonality to occur. Seems somewhat plausible to me but no more than that.
Also I’m skeptical that that the cases will be “extremely concentrated”. Sure, right now, most cases come from only a few areas and China had the disadvantage that the disease could spread while people were unaware of its existence. But this might be more than offset by less severe measures being taken elsewhere or in China at later times and right now, there are infections in 83 countries.
I want to propose a possibility, which I hope is unlikely or wrong, based on the following study: https://www.ncbi.nlm.nih.gov/pubmed/32104915
As far as I’m aware, the immune system doesn’t function well (at all?) in the CNS. The result being that CNS-infected patients who recover could act as asymptomatic carriers indefinitely. This is also proposed as an explanation for why “reinfection” via post-recovery testing is seen.
Regardless, given the scariness of symptoms described in the above paper, I sure hope that the probability of this form of infection is very small indeed…
No, this really isn’t an argument against early quarantine. If you act normally you will (on average) get the virus at the normal time, the peak. If you want to avoid that, you have to take active measures to not be normal, either quarantine or do something abnormal to catch it early. Simply not doing quarantine is normal.
And if you do something to catch it early, then you are the most important person to be quarantined! Quarantine isn’t just about avoiding receiving the virus, it’s also about avoiding spreading it.
And quarantining works even if it becomes normal. If everyone quarantines, it slows down the spread. Even if it isn’t enough to stop everyone from getting it, a slow spread means a lower peak.
https://siderea.dreamwidth.org/1576034.html
More prep advice– covers some things most people don’t seem to be thinking about like getting home repairs done sooner rather than later.
https://siderea.dreamwidth.org/1584075.html#cutid1
Prepping for IT professionals– if you need to add the opportunity to work remotely, get it set up and tested asap. Actually, this applies to organizations generally.
I’m reading comments on some of siderea’s prep posts, but I’m going to read more of them.
For example, the discussion of prepping for people with food restrictions is just getting started.
Minor thing: I got an electric can opener. You may be more or less disabled, and need to make your food as accessible as possible.
https://www.metafilter.com/185381/Prepping-for-a-pandemic
This includes a description of being too sick to get frozen food out of the freezer and microwave it because of not remembering how the microwave works.
As a thought experiment, if God came down from his heaven and cast a blessing of implausible competence on humanity that made everybody in the world follow the “wash your hands and don’t touch your face” precaution perfectly, would that be enough to stop the spread of the virus? For that matter, could it kill influenza and the common cold?
Influenza is also spread by animals (birds and pigs, to name a few), so no.
Just hand washing on its own might not be enough. One can also catch the infection by standing close to a sick person and breathing in the small spit drops they produce while breathing, coughing or talking.
If everybody starts obeying the WHO recommendations perfectly (staying home and getting tested when you’re likely to have the virus, washing hands, standing further away from others) there probably won’t be many more infections.
I agree that China’s quarantine – by far the largest ever attempted on this planet – has been a success. But how sustainable is it? Manufacturing PMI is down to around 35. Car sales are down 96% in February y/y (sic!). Air flights are down 75% or 80%, as a quick look at Flight Radar 24 would visually confirm. They’re looking at a double-digit drop in GDP if this continues for several months longer. Outside China, there are few countries with its combination of authoritarian fiat and social cohesion, so I put very low chances on COVID19 being permanently checked at the global level.
From that perspective, Robin Hanson had a very interesting post two weeks back (“Deliberate Exposure Intuition“) in which he argued for counterintuitive approaches to coronavirus, e.g. preemptively infected some people. (My additional suggestion would be to pay young people to get infected, as they have high survivability and are more likely to be out and about on the streets, which should depress r0 to a greater degree than would be the case otherwise). The core idea being that, with mortality rates of <1% under modern healthcare vs. 4% without it, the priority should be to avoid surges in healthcare demand, as opposed to containment as such (which is probably no longer feasible). Perhaps quarantines could be progressively tightened and relaxed over the coming months in such a way as to keep the numbers of new cases at a steady level.
The prospect of COVID19 becoming a seasonal affair with no diminution of virulence is a highly foreboding prospect. Even for young people, the mortality risk is 0.2%. The chances of dying on a Boeing 737 MAX flight is 0.0003%. I do not like the idea of having to take the functional equivalent of a few hundred 737 MAX flights per year, for years and possibly decades to come.
One unmentioned selfish argument in favour of trying to catch it late rather than early – if you are really lucky, there might be a known-to-be-effective treatment other than “treat symptoms, especially those that might kill the patient” by the time you catch it. I’m not too hopeful there, but it’s a possibility.
It strikes me as a not-unlikely possibility. Isn’t there already an antiviral showing promising signs? Our current flu medication is exactly what you describe, IME works stunningly well, and it’s for a viral disease. The FDA might be reluctant to approve medicines for new uses, but in a pandemic I think even they are more reasonable (Scott’s points aside), and we have a number of antivirals to test.
If you catch it late enough, there might be a vaccine, and then you could not catch it at all.
One other good source of information, for those who like podcasts: the excellent TWIV virology podcast has done several episodes covering what’s known about COVID-19 so far. Very much recommended.
For a more policy focused podcast Epidemic seems to be pretty good with a couple of hosts experienced in epidemic response.
With regards to the endgame, hopefully in a year or so we’ll have a vaccine and while this is an RNA virus it seems to have error correction mechanisms and be relatively stable compared to the flu. So once we have a vaccine it seems like it might end up basically under control the way that Measles currently is.
That’s all I found about CoV error correction mechanism: https://www.pnas.org/content/115/2/E162 Do you know any other source for that?
I would like to advocate people store at least a little bit of water, have at least some sort of charged USB battery packs on hand, and acquire some kind of radio communication mechanism.
It is a safe assumption that water, power, and internet will stay on. As far as I know, they stayed on in Wuhan. But for this, you’re not prepping for “the power got cut off”. You’re prepping for “there is a temporary power outage and instead of it being resolved in 30 minutes, it’s resolved in 5 hours, because of the million and one complicating factors that the pandemic places on everyday life.
Same with water and comms. You should assume the water will stay on and be potable. But if a water main happens to break, it might be longer than usual before it comes back on. The purpose of prepping a small supply of water and batteries is to bridge that gap
People should not be prepping only for coronavirus. Right now is a perfect time to make you are are prepped for “generic disaster” and something that can happen in “generic disaster” is that you don’t have power or water for a few days, and you can’t get them delivered either.
Not having water really sucks, so have 3 gallons on-hand per person. You probably aren’t going to need it for coronavirus, but a tornado/earthquake/terrorist attack might take out your water, so get some now.
Is there a way to store 3 gallons of water efficiently? Like, I don’t want unopened jugs to go to waste if nothing happens, and then have to keep buying water while the tap is still available. If I get a tank, can I use and top it off on the regular?
One of the links shows how to store water in Prepper Grade Water Storage Tanks. https://theprepared.com/homestead/reviews/best-two-week-emergency-water-storage-containers/
But I just bought a gallon of drinking water and put it in the garage, and put another in the freezer, and another in the chest freezer.
That link was really useful, thanks!
Stupid-sounding question: if heat inhibits the spread of this type of virus, should indoor public spaces be cranking up the thermostat?
Scott, I apologize if this is too close to a medical question for you to answer, but I am curious.
On the subject of coronavirus testing. The test involves running PCRs and looking for the correct DNA, right?
PCRs are really, really common, as far as I know. I did a quick search online and refurb PCR machines go for about three grand. I don’t know what reagents are needed, exactly, to run a PCR, but I know we’re talking about really small amounts of reagent.
I’ve seen https://www.youtube.com/user/TheChemlife on youtube go through a bunch of hobbyist bioscience processes, and I’m pretty sure he did a video on PCR. It didn’t seem that difficult.
So my question overall is: let’s say I say the FDA and CDC are pants-on-head tarded and screwing this up for everyone. Let’s say I am sufficiently rich (I’m not) and panicked (I am) to buy all of the above (It can’t possibly be more than $5k total, can it?). Would it be possible to run my own coronavirus diagnostic checks in my garage?
I assume this is illegal, or at least I could do it but couldn’t call it an official diagnosis. But given that our leaders don’t seem to be doing their jobs, and this is going to be a time for individuals who can to step up and pick up the slack, would this be something that would be scientifically possible? Or would it not work (process too complicated? Special reagent for testing this specific thing not available? Special machine for interpreting results of PCR too expensive? Biohazard danger? Etc?)
Normally independent testing is legal, as long as you don’t charge for it. The FDA made a surprising decision to ban it for coronavirus. Big labs should have defied this ban. But the ban was lifted a few days ago, so the bottleneck is gone and the question about individuals is moot.
What could individuals have done? What is the point of testing? Maybe there could have been PR value in proving that the virus was already here. But the main value of testing is for contact tracing. This combines testing with a very different use of resources. Was independent contact tracing possible?
Re contact-tracing, I doubt it.
When I originally thought about this, it was less as a practical tool for fighting the epidemic, and more as a thought experiment for “just how much of this could we do on our own, if we had to?”. I was reading some stuff online, one which quoted the cost of a test in the US at $3k, one which quoted the cost of a test in China at $5, and thought “there is no possible way it costs $3000 to run one test I bet a suitably motivated individual could easily do it for cheaper”
There’s lots of areas nowadays where a hobbyist with too much time on their hands can figure out a chaeper solution than anything that’s commercialy available.
The issues are with stuff like reliability and quality control.
The CDC’s test description is here. It’s not trivial and there are a number of ways to botch it if you’re not experienced, but it’s simultaneously not bank-breakingly expensive or extremely complicated. The largest problem for a home lab would be the test primers: they’re not shipping these out to every lab, and obviously less happy doing so to the not-so-average Joe.
These are possible to synthesize, but doing so adds a lot of technical complexity and raises the risk of error.
Its about as simple as molecular biology gets. I’ve done it by moving a tube between different temperature water baths when I had a thermal cycler break on me at the wrong time.
But you are correct, there are numerous ways to botch it.
You can get appropriate primers from any company that makes primers. I bought primers and a positive control plasmid from a company that I won’t post here so they dont get inundated. But if you know anything about pcr you will be able to find primers. Make sure you get a positive control plasmid.
PCR is actually pretty difficult, mostly in that accurately pipetting such tiny volumes is difficult. If you don’t have experience running PCR or other wet-lab microbiology processes I wouldn’t expect you to succeed without training and tens to hundreds of failed attempts. Also reagents aren’t available to just any rando.
The difficult part is owning a pipette that pipetts tiny volumes. But there isn’t any particular reason you need to do a tiny volume other than companies market up pcr reagents a few thousand x over the cost to produce them (I once made taq polymerase at gram scale for a couple hundred dollars).
A low-end automatic pipette can be obtained for like $50 on our local ebay equivalent. You could probably do a lot with a precise syringe, as well.
PCR needs temperature control (nothing a heater and arduino can’t provide) and some reagents you can order online. There are DIY schematics, no need to spend three grand. However, that just gives you a lot of DNA – obtaining meaningful information from the DNA is a bit harder.
Unless you want to get quantitative data from the PCR itself? AFAIK for that you’d need to procure very specific primers, from a small bunch of companies that are currently very busy producing those exact primers for a lot of labs worldwide, using a rapidly collapsing logistics chain…
I did much of thr same write up.
2% death rate is based on immature datasets. 3.6% is the new two. Same calculation, more mature data.
Any aggressive assessment of the impact of a Pandemic needs to factor our treatment capacity, and what the death rate would be when overburdened. I did my best to do this, and one analysis I did came up with 1 million infected as our handling capacity, before things get far worse. It’s really hard to be truly confident, however.
http://tinyurl.com/sv5v4vc
Really excellent analysis and article Scott!
Edit: 1 million infected as an boundary for death rate increase is wrong. The number I meant is closer to 30 million infected. By treatment capacity. In real world any number that high will get far worse as there’s no practical containment, 30 million will become hundreds of millions.
The predictive math for this is hard.
Following up on the mentions of copper and zinc, I cane across a number of papers mentioning bismuth as a Coronavirus inhibitor (google scholar: “bismuth Coronavirus” to find the papers; they are about SARS, also a Coronavirus). Anybody know anything more about this? Would pepto-bismol be any use as a over-the-counter defense? Can’t hurt, I guess…
I feel stuck in a bad situation. I am a student at a large university in a major US city. My basic living space (by virtue of being a dorm) is uncomfortably infection-prone, but if I were to hide out at my parents’ home I would jeopardize my academic career, unless they suddenly cancel classes. I don’t know how prevalent the infection has to be for ditching all my classes and commitments to be worth it.
Don’t exchange saliva or other bodily fluids and wash your hands, and you’ll probably be fine.
This, and also you should be in one of the lowest brackets for mortality.
Just in case get some bottled water/preserved food in your dorm room.
Then what the hell is the point of college?
I think the most serious risk for individual students is just the risk of everyone getting sick at once and all the places you usually get your food being shut down as a result. Help your friends learn to avoid touching their face, and get used to washing their hands regularly, so that once the virus gets into the student body, it will spread more slowly and won’t hit everyone all in the same week. If the university cancels classes, or moves them online, make sure you aren’t sick before you go home to your parents. (You might also be able to anticipate such a move, and if you read the signals right, your professors likely won’t penalize you for missing one week of class just before the university decides to cancel.)
But in any case, the worry isn’t about you personally getting sick, but rather about you and all your friends and cafeteria workers getting sick in the same week. If you can all take turns getting sick on different weeks, then it might just be like a bad flu season plus (unfortunately) a small number of student funerals.
Lazy option for receiving packages: have a staging area where you leave them for a week. Only sanitize the stuff you need to use sooner than that, or which needs to go in the fridge. Also the virus lives way longer in the fridge, so focus your effort on that stuff.
I keep on hearing that a vaccine is at least a year away. Why, though? We already have multiple promising potential vaccines ready for testing. Couldn’t you massively speed up things through something like the following:
1. Take the 5(?) best candidates for a vaccine and organize a wartime-level mass production of hundreds of millions of doses each.
2. Pay a thousand volunteers per vaccine candidate ~$100k each to take the candidate, wait two weeks, and then deliberately expose themselves to the virus.
3. Wait two more weeks and test the volunteers.
4. Any candidate that substantially reduces infection rate and has less-than-horrific side effects gets approved, and the hundred million doses ordered should be nearing completion.
I get that bioethicists would complain, but given the scope of the problem, isn’t this the sort of thing that a competent authoritarian government – say, China – could pull off?
1a. How do you rank the candidate vaccines?
1b. Mass production on that scale is straight-up not possible. The capacity isn’t there, and this outbreak is likely to have resolved itself one way or the other by the time you could build it; we have enough trouble making and distributing the annual flu vaccine as it is.
2. This is nowhere near enough people for a test; you won’t get a statistically-valid sample this way and even if you did a thousand people isn’t enough to catch all the side effects you’d have to. Suppose we did this, vaccinated everyone, and it turned out that five years later everyone who got the vaccine was sterile.
Did anyone ever get sterile from a vaccine? Proving effectiveness is hard, but safety should be a routine matter. Sure I wouldnt trust something i cooked up in my own garage per se; but the approach to a corona vaccine would be completely analogous to any other virus I imagine.
Note that the seasonal flu vaccine also gets recreated and distributed on a yearly schedule; without being tested for 5-year sterility in between. This corona vaccine need not be any different; the ‘real’ differences will lie in how much the FDA will arbitrarily categorize this as ‘just another flu vaccine that needs proper manufacturing, storage and handling practices, and will be fine’ or ‘an opportune moment to do a 10 year study that will prove that vaccines dont cause autism after all’.
I honestly would not want to be placing any bets on the outcome of that pivotal question.
Flu viruses are similar to each other but different from Corona. Flu vaccines are probably similar enough that we assume they will be equally effective and safe.
Afaik there has never been a vaccine for any coronavirus, so we can’t make assumptions about its safety and effectiveness the same way.
On the other hand, there’s no reason to assume the vaccine for this virus will be particularly unsafe. If this virus sticks around, and turns out to be the kind of virus that vaccines can prevent, I’d expect a vaccine to be available in 1-5 years.
> enough to catch all the side effects
How much does this depend on how novel the mechanism is for making the vaccine? If it’a truly novel mechanism which involves rewriting your DNA or something, you’re talking lots of novelty and risk. But if it’s “standard flu vaccine process”, only using Covid19 instead of the selected flu strain it should have the same risk profile as the flu vaccine, right?
‘Should’, ‘probably does,’ and ‘proved sufficiently to satisfy FDA and get the manufacturers included under the National Vaccine Injury Compensation Program’ bear only a nodding relationship to each other.
Just offer a prize of say $10bn for the first company to deliver say the first 1 million samples of a proven vaccine. I bet you would mobilise a lot of people to work on this to win this prize. Institutional funding will focus first on the reputation risk to the people organizing the funding, so anything a bit strange or wacky, or from people who are not already proven won’t get funded. So avoiding Type A errors but not Type B.
Keeping the “proven” part honest might be harder than it sounds.
Establish a committee of eminent scientists as a jury to determine if the vaccine meets the standard. Of course some human judgement will be required but we live with this kind of risk on most contracts.
But what if the committee of eminent scientists isn’t diverse enough?
Prizes don’t work at that level. They work for things that can be financed by individuals out of their “mad money” budget, like Paul Allen building a minimalist spaceship, but that’s tens to maybe hundreds of millions of dollars. At the gigabuck level, there’s too much risk for the sort of individual investors you’e going to need, and as Nancy notes too much potential for corruption.
Large pharmaceutical companies deal with this kind of risk all the time, that their efforts fail. This prize would add extra incentive and make them more more willing to indulge ideas from their researchers on vaccines. Oil companies routinely drill oil prospects with 10% chance of success, because the payoff is large.
Oil companies don’t need to convince a committee of eminent chemists that the stuff they’re selling is oil. Nor is e.g. Exxon’s oil instantly worthless if it arrives at the market a day behind British Petroleum’s.
@John
If you are concerned about this second place issue, we can have a second prize of $1bn. Then at least the second prize winner gets some compensation.
On convincing people on the efficacy of their vaccine, I really don’t understand this concern. Are we really thinking that a committee of eminent scientists will turn down an effective vaccine at a time like this to save the sponsors money? And big companies face this kind of risk every time they submit a bid to the Government, like for an aircraft program, or public infrastructure. They are willing to spend plenty for a lottery style chance of a big pay off.
They won’t “turn down” the vaccine.
But they may decide that it doesn’t quite cover things well enough, or has too many side effects, or doesn’t provide immunity long enough, and really this was all research stolen from the public sector anyway, and you should be happy with the $1 billion, it covers your costs, or what should have been your costs, and a crisis is no excuse to let you get away with profiteering.
If you want companies to have confidence in the prize-model, the time to work on building confidence in the prize-model was 10 years ago.
For example, one area of drugs really not served well by patents is antibiotics: we want companies to invent them, and then put them on a shelf for 20 years until we really need them. So WHO could be offering 10 billion dollar prizes, right now, to companies to invent new antibiotics, at which point WHO puts them under lock and key. Worst case scenario is that, like now, none get invented.
Work on that. Maybe you can show that prizes work.
CMV: Surgical masks will protect you from covid-19, if you wear them reasonably. That this is not consensus among the rationalist community feels crazy to me.
Scott writes that the virus is not airborne: This is PRECISELY why surgical masks will help though! Surgical masks are not great at filtering out smaller particles, but this virus is transmitted through larger droplets, which the mask absolutely will keep from going inside your mouth. (Actually the mask will filter out 70% of small particles anyway, even if fitted poorly, so bonus points for keeping you safe from the regular flu and colds too! https://academic.oup.com/cid/article/54/11/1569/321689).
When you talk to coworkers, cashiers, etc. face to face, your mouth and nose is protected: If anybody sneezes or coughs, and you happen to talk at that moment, the droplets will mostly not fall into your mouth!
The CDC websites state that the droplet route is currently the most likely, so that should be a large benefit!
The danger only lies in touching your face too much to readjust the mask, but can be easily avoided through merely touching the straps.
Every article I read that says: “Don’t use masks, they are not effective and health care workers need them” infuriates me. If they aren’t effective, then why would health care workers need them.
Also worth pointing out:
“Don’t use masks, just avoid touching your nose and mouth” seems like weird advice. Won’t using a mask help prevent touching your nose and mouth?
Health care workers are exposed to a lot more viruses than you will be in your daily life. Even then, the surgical masks are to prevent droplets from the health care worker going into patients’ moths and open wounds, and need to be changed every few hours. The N95 masks may be needed when nurses get close to a very ill patient while intubating them, or similar situations that you won’t encounter on the metro.
As for your nose and mouth, many people will touch them while adjusting the mask or when putting it on, taking it off. You might be someone who will use the mask competently, but people in general probably won’t. So when weighing the need of health care professionals vs the general public, the advice to not buy / wear masks is correct.
> why would health care workers need them
Because we go to work with mild illness ourselves. If I have a mild cold, I’m not going to call off a shift on the ambulance. But if I’m going to a nursing home or something, I will put on a surgical mask because the last thing those folks need is a respiratory illness. It protects my patients, not me. I’m more than happy not to, but it could result in a bunch more people dying of pneumonia or whatever.
When I go somewhere I might be exposed to a droplet illness, I’ll put on a disposable N95 mask. This is to protect *me*. If I don’t have such as mask available, I’m not going in. So a lack of N95 masks would mean a potential lack of emergency and transport ambulance services. And that alone (disturbingly) would cause the healthcare system to collapse.
There was a discussion several threads back about answers to a child. The widely proffered information on masks, that they are “ineffective” for the general population, is an oversimplification that comes close to being an outright lie. This is a dangerous way to communicate with the public.
The complicated answer is that, on balance, given the overall availability of effective masks, the absolute need for healthcare workers to have them, the high potential for misuse among the general public, and the situations that the general public typically find themselves in, the correct advice may be that the general public should not be out buying masks. I’m not commenting on that policy prescription, but the way it is communicated.
Telling people outright, with no further explanation, that: “masks are not effective in preventing the virus, you shouldn’t buy them, healthcare workers need them” contains an glaringly obvious contradiction. The right masks are effective, that’s why healthcare workers need them. Without the additional context offered above (which requires research to find and is not presented in the typical “don’t buy a mask” article), this obvious contradiction will lead many to ignore the “leave the masks for the professionals” policy prescription.
If your model (which doesn’t seem crazy to me) is that wearing a surgical mask should be effective because it protects you from the droplet route — make sure you also wear some kind of glasses or goggles. Your eyes also have mucous membranes.
Is it possible that the masks are not as effective because once the droplets get attached to the mask, the act of breathing will cause you to inhale the virus from the droplets? That was my assumption because, like you said, saying that they are not effective otherwise makes no sense.
If this is indeed the mechanism, then it would explain why it is helpful to wear them when infected. The water droplets will get stopped by the mask and the act of breathing is not sufficient to propel the virus far enough pas the mask.
Some droplets will be small enough to get through gaps between the fibres of the mask.
Also the mask is not tight-fitting so bioearosols can go around it.
If you google ‘wuhan doctor’ you’ll see a lot more people wearing proper particulate-filter masks than surgical masks.
(some of them seem to be wearing both?)
Are there any plausible hypotheses for why this causes so much less illness in kids than influenza? In particular, are there any plausible mechanisms for kids being resistant that might point to novel ways of protecting adults?
A doctor friend theorizes idly that kids get exposed to such a variety of different things from their schoolmates that they probably have more useful antibodies, but this seems like it proves both too much (it would imply more resistance among kids to the “regular” flu than we see) and too little (why aren’t there any deaths among pre-day-care infants in the homes of family members with coronavirus)?
I also find it shocking that kids are not getting sick/dying. I have a 4 and 5 year old and they get sick all the time. Often I and my wife will not be sick while they are sick, or our symptoms will be much less than theirs if we also are sick. It is not uncommon for me to simply feel like I have a mild cold, but for my kids to have a fever and then a runny nose for several days.
I heard a Swedish doctor speculate that the virus might attack and live in some lung-structure that isn’t properly developed in kids, yet.
On the subject of prepping, I’ve found this retrospective on Katrina as an excellent look at what a real modern disaster situation might look like: https://sites.google.com/site/southernbelleprepper/lessons-from-katrina
Not terribly applicable to Coronavirus since there won’t be evacuations or power / water / comms breakdowns, but good to think about if current events are enough to convince you to put some effort into emergency preparedness. (Do you live near the Cascadia subduction zone? In wildfire, tornado, tsunami, or hurricane regions? Near an active war zone?)
I agree with Metaculus. There isnt enough time between now and the end of the flu season to take the current levels of growth to regular-flu beating numbers.
That said it wont just go away; and it will probably flare up even harder next season, with most people still not having exposure, but the virus not having to start from scratch anymore, but being present all around the world already. Having an effective vaccine before the next season might be pretty essential. Though it seems thats within the cards. Better hope you dont live within the jurisdiction of the FDA I guess.
As far as I’m aware, we have no strong evidence that this virus is seasonal in the way that influenza is. If you believe differently, can you link sources I can check out?
It’s far from conclusive, but it’s a bit surprising to me that we don’t appear to be seeing a ton of cases in countries like Thailand and Cambodia. One reason might be that the virus finds it harder to spread in hot, humid conditions.
The numbers of Thailand look more like they’re infected, and not bothering with lab tests:
https://ddc.moph.go.th/viralpneumonia/eng/situation.php
Basically, I don’t think the geography of infections is conclusive evidence at this point, as there are relevant socio-political correlations with geography that will take a bit more time to tease apart.
If by ‘strong evidence’, you mean observing the virus over at least one whole year, then no.
But as a general tendency of viruses like this that spread via air or other indirect routes; and are thus exposed to humidity changes and UV and whatnot; there is a pretty strong prior id say.
Also the point below is a good one; there is already a pattern where it takes hold more in the temperate regions than in, say, india.
One thing I haven’t seen remarked on is how vulnerable Health Insurance companies might be to this. If they have to sell depressed assets to cover a surge in costs that is a typical situation for bankrupting companies that work on their models.
Cold-blooded, back-of-the-envelope take: if this does get loose in the US and behaves like it has been in China, it could be great for insurance companies, because it’s many tens of times more deadly to old and immunocompromised (read: very expensive) people than it is to young and healthy (read: cheap) people. There’s a natural limit on outlay for COVID-19 treatment (organ-support, mostly and as far as I’m aware) in the form of available ICU beds; all they’d have to do is avoid a liquidity crisis while things sort themselves out and conveniently the Fed’s just made that easier.
It might however also create public outrage because people avoided testing in order to not pay the copay, which could lead to support for Medicare for all plan, especially if Sanders wins the nomination.
Japan is going to be a country to watch, they are already massively in debt, have an aging population and national health care, and their economy contracted by >6% (annualized) in Q4 2019 due to a sales tax increase. Oh, and their deficit was almost 5x GDP growth in 2018, and that was the lowest deficit that had in years.
Isn’t Medicare providing the bulk of funding for the over 65 population?
This doesn’t seem right, a quick google gives me a 2005 result of ICU beds being used at ~67% and a total cost of 82 billion, for the potential to add 40+ billion in costs over a year in 2005 dollars and net income for the health insurance industry in 2018 (again just quick google) was $21 billion. Just the increased usage in ICU beds has the potential to wipe out 100% of net income in 3-6 months, with them having to spring for way more doctors visits/pharmacy visits for the rest of the population. It is also not like people who need the ICU will be turned away from the hospitals, and there will be constant emergency room visits maxing their capacities out if the outbreak is bad enough.
Fair point, I wasn’t thinking about what it would look like if rather than going from ‘things are basically fine’ to ‘country shuts down’ relatively quickly, we just sort of stagger along with the health care utilization slider set to max for the entire flu season.
> in the form of available ICU beds
Epistemic status: vaguely informed. I hope a real intensivist can comment.
An “ICU” bed is a useful label/category in a map/territory sense. I have no doubt that it meets a certain regulatory/legal/billing requirements. Not every patient in an ICU bed needs all of the equipment/services required to be associated with an ICU bed.
In my mind, the more interesting question in: which of the services normally associated with an ICU bed would actually be required? How many other beds in the hospital could be augmented with the required services and equipment short-term or long-term?
On a short-term basis it’s may also possible to substitute large amounts of lower-level manpower for ICU equipment. As a related hypothetical: if what’s missing is a lack of equipment which can handle arterial line blood pressure monitoring, you might be able to “substitute” by having a tech measure blood pressure by hand every 5 minutes. It’s less accurate and a lot more expensive long-term, but something which can be scaled up.
New York is putting together a plan for the government to pay for everything. It’s an election year and it wouldn’t surprise me if something similar came together nationally.
I’m sure they can do this for modest case scenarios, but I am not sure how they can for a serious outbreak.
Wondering how else to help our neighborhoods beyond the personal prepping. I’m a veterinarian. I would not want me being a frontline ER doctor, but in a pinch, I can place IVs, monitor symptoms, triage patients, perform CPR, dose drugs, etc. If healthcare workers are either overwhelmed or starting to get sick at unsustainable rates, what next?
Does anyone know of any planning that’s going on to ready a healthcare worker reserve of people with some medical adjacent skills?
Boris Johnson has a plan to ramp up volunteers for the NHS. I am unawere of any other such plan for the US, or other European countries.
I’d suggest reaching out to your local hospital(s) ahead of time and asking such questions. A couple of possible avenues I can think of:
One silly idea is that you might actually be able to get privileges there. After all, there will be patients who have service animals who might themselves need care and having both recuperate together might be beneficial. Or something. Likewise, we in EMS are not allowed to transport animals for medical care, except for K9 officers (the dogs themselves), and it might be useful to be “on-call” for a hospital in that case.
Another would be to become an “occasional” staff member as an advanced patient care technician. You’d probably have to actually work a shift a month or so. (If you agree to do so as a volunteer you’ll probably get more flexibility). You’d be best looking at the specific requirements for your local hospital “careers” page. In general, you’d be well-served by getting an ACLS certification as well as taking some of the core NIMS classes. The up-side is that NIMS 100,200,700,800 can be done online for free. The down-side is that they are the benchmark I use for how painful an online training course can be.
The third option (which might help you become a PCT as noted above as well) is to get yourself an EMT certification. It would allow you to be out in the community, able to assist not only with issues in the hospital but also disasters in the field. And if a hospital enters a crisis and needs lots of people, being able to show up with an EMT certification immediately lets them slot you into a certain type of work.
I don’t have any experience at all trading currencies, so even if I got a good response here I possibly wouldn’t do it, but…
If I though the Yen was going to drop to ~90 in the next 6 months how would I play that if I only wanted to risk a modest amount with high leverage (willing to lose it all)?
Buy July Yen puts, strike price 95 or 100. These give you the right, but not the obligation, to sell yen to someone else at 95 or 100. If yen is at 90 or so, you’ll profit.
You can trade fx options @ CME. You’d have to see which retail providers offer that though.
Contract size is ¥12500000 (~117k), June 9150 put is trading at about $730 looks like. 9000 is about $230.
They don’t provide open interest, so no idea the liquidity.
Edit: had contract size wrong.
In terms of prepping/helping to reduce the severity of the outbreak, getting a flu shot is another big thing you can do. This lowers the risk that you (and others!) end up in the hospital with the flu taking up a bed, and reduces the likelihood that you (and others!) end up with the flu+coronavirus.
Seriously, people saying coronavirus might be comparable to the flu just drives home the fact that the flu is really bad! And we already have a (imperfect, but much better than nothing) vaccine for it.
On severity by age: I found Scott Gottlieb’s tweet that that figure comes from, and the paper it links for COVID numbers by age.
I’m guessing what Scott was using for hospitalization numbers was the entire study population (nothing else I noticed in the paper would match the description, and the numbers look right at a glance), but that includes outpatients as well.
Particularly relevant is the graphic in Scott’s third tweet, that extracts part of Table 1 from the paper. The percentages there are percentages of each age, within the group with severe symptoms; calculating the other way, severe symptoms are present in
12% ages 15-49
17% ages 50-64
29% ages ≥65
for 16% overall.
(“We defined the degree of severity of Covid-19 (severe vs. nonsevere) at the time of admission using the American Thoracic Society guidelines for community-acquired pneumonia.”)
Rates of “admission to an intensive care unit (ICU), the use of mechanical ventilation, or death” (the “primary composite end point”) were:
2% ages 15-49
7% ages 50-64
20% ages ≥65
for 6% overall.
I’m also surprised by how even the severity numbers are. I don’t know how much to expect this is biased by mild cases being less likely to go to a hospital at all (which I would expect to bias in this direction).
I put together a timeline visualization of data indicators of narratives about coronavirus:
– case numbers
– TV news airtime dedicated to coronavirus
– public interest on Wikipedia, Google Trends
– financial markets
– feature articles
– government actions
It shows the interplay between different segments of society
https://twitter.com/townhallindex/status/1234963382568132619?s=21
If you’re the person behind Town Hall Index, thanks!
Are you sure about surgical masks not being useful because the virus isn’t airborne? The CDC lists the main sources of spread as:
Surgical masks could probably help with the second situation by blocking droplets from getting into your nose or onto your face. They also keep you from touching your face.
Also:
Doesn’t this imply that surface contact isn’t how the virus mainly spreads?
I believe he’s actually saying they are a result of false _negatives_. That is, they were definitely positive, they appeared to recover and tested negative (because they weren’t shedding enough virus, or whatever), then a later test came back positive, but they were actually still infected the whole time.
The Chinese government’s ineptitude and lies is what caused this in the first place.
They concealed human to human transmission, allowing for open travel with China for longer, which resulted in it spreading.
If travel had been shut down at the start of January, this probably wouldn’t have gotten out of China.
Remember: the CDC now believes that the cases in the US originated around January 15th.
China’s lockdown didn’t happen until January 23rd.
So the Chinese lockdown was really too little, too late in terms of stopping it from spreading globally.
The PRC spin is that everyone else is incompetent. But the reality is that the disease had already gotten out.
This is the PRC’s fault. They’ve done very badly, and need to be roundly criticized for suppressing news about the outbreak until it was too late.
One big thing I am hearing from other health care professionals is that coronavirus concerns are taking resources away from other things. If the ER is jammed with people who think they have coronavirus, the guy who has chest pain may decide not to bother coming in, or he may not be treated as quickly compared to 2019. I suspect that these indirect factors may lead to more undesirable outcomes than the virus itself.
This is true even– or especially– if many of the people who think they have coronavirus actually do have coronavirus.
See also results of a surge of people needing ventilators, ICUs, and medical professionals.
> If the ER is jammed with people who think they have coronavirus, the guy who has chest pain may decide not to bother coming in, or he may not be treated as quickly compared to 2019.
There’s a difference between the ER itself being jammed up, and the waiting room being jammed up. ERs screen patients and assign them a priority score based on various criteria. Chest pain goes towards the top of the list regardless. If people are just showing up because they have the sniffles and are worried they have Covid19, they’ll be given a mask and told to wait. And wait. And wait.
If ERs find this to be a problem there are multiple approaches they can take. The “fast track” or “urgent care in the ER” approach which many ERs are implementing with mid-level providers is possible solution. A person comes in, gets evaluated, gets swabbed if appropriate, gets a pamphlet on the healing powers of chicken soup and is sent home.
And we already have problems with people not coming in when they have chest pain. Most of the cardiac arrests I work start out with chest pain that didn’t want to go to the hospital.
I don’t understand how you could ever get over Covid if you didn’t become immune to it. Your body would be constantly re-infecting itself.
I don’t think it’s a binary thing, more a question of ‘how immune for how long’, with variation between individuals.
“Rough Fermi estimate: there are 10 reported cases in the Bay Area.”
What worries me is that we don’t really know how many people are infected because CDC botched test kits production, and hospitals are unable to test patients with covid-19 symptoms.
One thing I haven’t seen mentioned is the likely effect of BMI on survival, especially the bad effect of low BMI (less than 18.5, and perhaps less than something higher, like 20). Here’s a study on this:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6304312/
It’s an observational study, but does account for the most obvious confounders like serious chronic medical conditons. It finds that being underweight (BMI<18.5) is associated with an odds-ratio for serious complications of influenza-like respiratory illness that's about five times higher compared to normal weight (18.5<BMI<25).
Unfortunately, they throw away data by converting BMI to a small number of categories, so we can’t tell whether somewhat higher BMIs, such as 20, are also associated with bad outcomes.
Being morbidly obese (BMI>35) is also bad, but you probably already knew that.
If there’s a rush on hand sanitizer and I can’t get any as a result, I can probably make an equally effective one of my own from ethanol or the nearest hard liquor, right?
The World Health Organization has a guide to making small batches, which CNN says you shouldn’t do. It’s alcohol, H2O2, glycerine, and water. (you may have to do some math based on the strength of your alcohol)
Hard liquor (except overproof) is generally not strong enough and should be reserved for internal use.
As if I didn’t already dislike CNN enough…
Just find a sink and use soap/water.
It’s significantly more effective than hand sanitiser.
How are you going to find a sink when you are in the train? After you handle money in the supermarket?
Wander along the train till you find a toilet.
Alternatively, wait till you reach a station and don’t touch your face before then.
Perform contactless transactions.
About the EMH: Even if you can predict that stocks would become less valuable that would not imply that stock prices would decline in terms of money. Judging by the price of gold, investors also figured that money would become less valuable.
Also, anyone shorting the market who didn’t get out on Friday may have had a bad few days. Even if you can predict long term trends, you probably can’t time the market well enough to fully capitalize on them.
Not really. I mean anyone literally shorting the market had 2+ weeks to put on their shorts at above 3300 on the S&P. Even if they shorted at the Jan 31 absolute low of 3225 and sold at the absolute peak yesterday at 3130 they still would have made a good amount of money on the trade, and the value of the trade from an EMH perspective would be 2X that.
To have your shorts be underwater at any point you would have had to put them on 4 full days or more into the decline. Any point during those first 4 days you basically couldn’t sell them at a loss if you tried, and the previous 5 days you would have had to change your mind very quickly and sell out to lose even a modest amount (or buy very short dated puts or something).
Beyond this anyone who decided not to short the market but instead did the typical thing and moved into bonds out of stocks has well exceeded average market returns without ever being behind market in any move like this taken since the end of December/early Jan, with a couple of highly specific exceptions (like if you did this on 2/3 or 2/10 you would have worse returns for a couple of days).
Contrary to what you say, Metaculus is not optimistic: Their prediction is a 10% chance that it kills over 100 million people. Also, the median estimate you report is several days out of date: On Feb. 29 the median was 140,000 thousand like you said but by now (Mar. 3) it has gone up to 800,000. Strangely these estimates have gone up extremely rapidly in the past few days, roughly doubling every day, which suggests Metaculus users still haven’t reached a conclusion.
Also, there are a lot of other disasters that can befall you over the years such as earthquakes and hurricanes, so taking this moment to focus on prepping can be helpful. For example, I’m now much more ready for an earthquake than I was two weeks ago.
How hard is it to ramp up production of various things which are in short supply? Test kits, masks, ventilators, ICUs. The hardest category will be medical professionals. Even figuring out what can be done by people who are less trained than usual is going to be work and take time.
It depends. If the government elects to suspend enforcement of certification requirements and other bureaucratic obstacles, production could be ramped up quickly given enough money. Without them burning the red tape, it will be difficult to produce more medical supplies quickly, especially considering a lot of them are made in China. As for medical professionals, the best option would be to get people to unretire using a combination of financial incentives and an appeal to patriotism.
> Test kits, masks, ventilators, ICUs.
I commented about ICUs above. But gear is going to be the most challenging, IMO. Routine medical equipment supply costs, especially drugs, have been driven down drastically. This has removed a lot of slack from the supply chains. There are currently over 100 drugs listed as being on shortage by the FDA. After that hurricane went through Puerto Rico we were short bags of IV fluids for months.
> The hardest category will be medical professionals.
Not exactly. There’s a whole pile of bureaucratic bullsh*t which gets in the way, but it’s mostly from the hospital risk management teams, not government regulation in this case, funny enough. The easiest approach is to use something referred to as “delegated practice”. Broadly (and this varies by State law), it’s the idea that a physician can delegate the performance of most any task that they themselves can perform to someone else, but are responsible for the results/complications.
For a single disease/outbreak where the issues at-hand are likely to be similar, it would be easy enough for ICU doctors to set up a set of protocols/algorithms to use (probably the same ones they’re using) and assign them to be followed by other lower-level but skilled providers. By-definition Physician Assistants can transfer over “seamlessly”. Other mid-level providers, paramedics and various patient care technicians could handle most of the cases that way.
If, for the duration, most elective procedures were cancelled, you could also call upon large numbers of surgeons and surgical staff, etc. There’s a huge amount of human-capacity slack in the system as long as we’re willing to accept 99% results instead of 99.9% results.
Anecdotally, I was at a medical office today and they said that a generic box of nitrile gloves, usually $4, is costing them $20. What is your guess on where it will max or when it will get back to $4?
I feel like SOPs are going to impact supply at various facilities more than production interruptions. A medical office will be looking to specific vendors for a specific brand of glove of a specific quantity and size, as is their regular practice. The process for approving other vendors and other brands will prevent them from driving down the street to the nearest dollar stare and picking up a bag of nitrile gloves for a dollar.
https://www.livemint.com/companies/news/paracetamol-antibiotics-vitamins-on-export-ban-list-to-fight-coronavirus-11583228746928.html
“As fresh cases of coronavirus are reported from India, the central government has banned the export of certain medicines including the popular Paracetamol, several antibiotics and vitamin formulations.
The export ban list includes Paracetamol, Vitamin B1, Vitamin B6, Vitamin B12 and their formulations. Export of 26 active pharmaceutical ingredients (APIs) and formulations require licence from the directorate general of foreign trade (DGFT) which has now ordered restrictions on 13 APIs.”
From the BBC: the problem is that they’re concerned about getting ingredients from China.
I must say, the conversation about coronavirus prevention measures devolving into tribalistic accusations of racism has made me pessimistic about the future of the US in a way few other things could have.
How does the United States keep going with its public discourse decayed to that extent?
I imagine the Chinese (ethnicity) people who actually were avoiding Chinese restaurants when those stupid pieces about how Americans were racist for worrying about coronavirus were going around just literally laughed in Chinese. Anyway, all that nonsense appears to have vanished now that the virus has a confirmed foothold in the US.
I was travelling in the US in january. Literally the first I heard of the virus (wasn’t really up on news) was from a Chineese-American AirBnB host, who said she cancelled all of the bookings made by Chineese people.
There was another outburst just yesterday, surrounding a demonstration in SF against anti-Chinese racism. Some people suggested that such a large gathering might not be the best idea in the current circumstances… You can guess the rest. The was the immediate context to my post above.
But beyond the partisan particulars of that controversy, what has me scared shitless is that there seems to be absolutely no crisis or catastrophe left today capable of making Americans pull together, rally around the flag. The US looks brittle and vulnerable to its enemies abroad.
Which enemies abroad did you have in mind? The Chinese are our admittedly-shady business partners, the Russians are (allegedly) allied to one of our political parties, and while it appears to be true that large chunks of the Middle East appear to hate America qua America, one might plausibly argue that we kind of brought that on ourselves, what with the whole decades-of-meddling-and-occupation thing.
I can’t think of a problem we have from the set where flag-rallying is a natural response, is what I’m saying.
Russia only propped up Trump to sow chaos. They aren’t allied with us in any meaningful way.
What exactly is the distinction between droplet and airborne transmission?
WP seems to say 5 micron is the cutoff. Is wet droplet vs dry nucleus also important?
(i.e. you’re safe from <5 micron particles/droplets)
Note on disposable respirators: If you do use one, make sure to handle by the straps where possible to avoid contaminating the inside. Also best not to store them in humid conditions (e.g. a plastic bag), but that's more about bactrial growth.
Question: Do you think it’s worth getting an oxygen concentrator while they are available?
I’m primarily worried about my parents/grandparents, and them getting sick after our hospital system gets overloaded. It seems like oxygen therapy is the most common hospital treatment (outside of fluids, which by all indications can be easily administered orally in the home setting). Currently I am able to get a used 5L/minute flow oxygen machine without straining my finances. Thoughts?
Metaculus is now predicting 1.04 million deaths, that changed drastically overnight.
Since this is an open thread for discussing new developments in the outbreak I think it would be better to have the comments sorted in reverse order like the other OTs by default.
I just noticed there’s a button to do that though, so that’s neat.
NB: it seems like that button doesn’t show up on the mobile browser.
A thread running through Scott’s writeup is the problem of whether the official sources of information are being honest, or are shading their advice/factual claims in order to achieve some other social goals. And this highlights why the “noble lie” strategy is so damaging over time–your official sources of information spend their credibility on noble lies, and then their factually true, well-informed statements are less likely to be trusted in a panic.
A little handful of noble lies and reaffirming social truths that aren’t factually true and staying on-message in the face of equivocal or uncooperative facts is enough to poison an information environment. And when that happens, it makes life a hell of a lot easier for the purveyors of conspiracy theories and lies and propaganda.
> Some of the reasons given are idiotic: the virus is not common in the US yet, so you are wrong to worry. This reminds me of all the people saying that AIs are not currently superintelligent, so any discussion that AIs might become superintelligent is just fearmongering. Who are these people? How are they still alive? How do they avoid driving off cliffs? They’re heading towards the cliff face, and their passengers scream at them: “YOU’RE DRIVING TOWARDS A CLIFF!”. And they calmly respond with “We are not falling off the cliff yet, we’re on perfectly level ground, there’s no reason to panic.”
Dumb paragraph that adds no value to any points you’re making. Pandemics are not the same thing as AI and operate by completely different rules. Making an equivalence between the two is most certainly some kind of fallacy, I think I read about mott and bailey here and that’s what you’re doing.
Question: Scott writes:
But the post Scott links to for Jacob says:
I can’t find anything saying Jacob made money. Jacob doesn’t say he invested in respirator and bean equities or futures, but the actual items. Is there something else Scott meant to link?
As to the EMH, the test would be if you could build a Taleb-style fund that identified cases where the market lacked the insights of rationalists and make money over dozens or hundreds of trades. I’d be fascinated to see such a fund in action – it would potentially be a good test of both the EMH and whether rationism produces concrete day to day benefits over whatever reasoning people use when applying Chesterton’s logic gates.
You can’t really test it that way because the EMH discussion has shifted to ‘risk adjusted returns’ and you could defend the EMH by declaring that their risk adjusted returns weren’t in excess because they took riskier bets.
Long story short, the H in EMH is there for a reason, its more a framework for approaching investing than a theory or a rigorous academic model.
It’s not a perfect test, but over enough time and bets, it’s a better one than any alternative I know. (It’s true that it’s hard to know if a portfolio is balancing above market returns against a minuscule chance of total disaster, but I would still rather see performance over time to test an assertion that a particular strategy can beat the market, and I would find beating the market to be instructive on whether rationalism helps day to day decision making).
On reflection, maybe Scott’s point is that when our conclusions differ from the market, it’s rational to go with our conclusions.
What Jacob talks about is acting as if he has concluded there is a higher probability of substantial crisis than the market seems to believe, which IMHO makes sense, although you can get to that conclusion with risk preference as well.
Nobody seems to ever mention this, so maybe there’s something stupid I’m missing…
…but is it effective to protect yourself when you’re out and about in public by wearing gloves? This, more than masks, seems to protect you from the coronavirus that is supposed to remain on objects for a few days. (Plus, it’s a tactile reminder not to touch your face.)
I don’t typically have other people breathing on me in my day-to-day life. At least, not from up close. But I do have to constantly touch objects that other people have touched.
As far as I’ve heard, the danger with gloves is that the virus will survive longer on them than your bare skin, and your skin isn’t really how it enters your body. If you’re diligent about not-touching-your-face, gloves don’t help that much, and if you’re not, they might actually make the problem worse.
Obviously, if you’re actively handling stuff you’re worried about, or you’re in a position to change gloves frequently, *or* if you’re trying to keep the virus in rather than out, they could be a good choice.
With that said, I think it’s probably good that we’re not generally pushing people to wear gloves.
The most useful scenarios I can speculate on are:
1) wearing gloves is a good reminder that something is different and you should take more care not to touch your face;
2) removing the gloves can act as an instant handwashing. You could wear gloves on the subway and then remove them as you exit and walk to work. But then, why not just carry hand sanitizer?
A presidential candidate already immune to the disease would be ideal for crisis management. A golem perhaps.
So the rationalists are finally on board the Corona disaster train! Only a month behind right wing twitter. Good judgment and intuition proved more reliable than empiricism and waiting for the “facts” from the experts. Who would have guessed? Still, I am glad you are finally on board. That being said, I still think there is not near enough skepticism regarding expertise.
Empiricism and “waiting for the ‘facts’ from the experts” often diverge. Viewing the early footage from China gave you a good idea of what was going on. China’s actions didn’t make sense outside of things being as they are now. I’ll call that good evidence and not spooky premonitions.
Metacalculus’s estimate seems to be trending log-linearly upwards. It’s currently at 771k after 377k yesterday. Not really a good indication that informed people have stabilised in their expectations.
So, the metaprediction is that in two weeks Metacalculus will be predicting imminent human extinction by coronavirus?
“The theory is: you quarantine yourself for a few weeks or months while the epidemic is going on, eventually there aren’t enough virus-naive hosts to sustain transmission, and we’re all safe until the next time some moron in China eats a bat.”
Not only the writer’s casual racism towards the Chinese is rather distasteful, but the facts also appear to be false in two significant aspects a) the source of the COVID 19 appears to be snake rather a bat, and b) there’s evidence from China that people do not develop immunity to the virus once they get better, i.e. virus-naivety condition seems to invalid in the case of COVID 19.
In what way is it racist against Chinese people? A is not at all significant. B is impossible.
It’s called a joke.
And the thing you did is called virtue signaling.
Also, I am offended on behalf of the snake people. Unlike the disgusting humans who merely wash their hands with soap, we shed our skins.
Are there any good estimates out there of the asymptomatic carrier rate for coronavirus?
I read here that as of last week on the Diamond Princess there had 4061 coronavirus tests done, finding 313 symptomatic cases and 392 asymptomatic cases. But I don’t know where to go to find more information on what the age breakdown was (it seems likely that more of the asymptomatic cases were younger) or how many of the asymptomatic cases later became symptomatic.
Obviously a high asymptomatic carrier rate is terrible news for anyone in an official position trying to limit the spread of the disease, but okay news for anyone in an area where the virus is already circulating widely, and whose base assumption is that they’ll probably get it at some stage.
Also it’s interesting to ask whether they’ll eventually develop symptoms but it’s taking awhile, and how much virus they’re shedding, and even whether there could be some kind of false-positive going on.
The ratio of asymptomatic to symptomatic cases is also similar to that among Italian people who tested positive.
How low would the US death count (achieved without widespread authoritarian quarantine) need to be before people who are currently impressed with Chinese quarantine cease to be?
Seen so many people telling me how I should be panicking but does anyone have actual data on why I should panic? From what I’ve seen this entire situation is closer to a social media viral phenomenon, not the zombie apocalypse.
A widespread pandemic with a 1-3% mortality rate isn’t the zombie apocalypse but it means that for an average person, one or two of your friends or family will probably be killed.
How much that should panic you is a personal call.
For young people, it probably makes more reason to worry about their parents or grandparents.
I wonder whether thinking about risk for other people allows you to act more rationally. Worrying about risk to yourself has negative connotations (cowardice), but worrying about risk to other people has positive connotations (care).
For example, buying a two-week quarantine package for your parents or grandparents is relatively cheap (a few kilograms of rice and pasta, some sauce, toilet paper, paper towels) and… in worst case you help them a lot, but in best case you still send a tangible signal that you care about them (and the things get used anyway). Win / win!
Fatalities won’t be spread evenly across the population. They’re going to be very lumpy, clustering geographically and around other focii (particular schools or businesses, perhaps). And as the sibling post notes, they’re also biased toward certain demographics.
So my bet is that with that with that overall rate, the median person will still be pretty close to 0 fatalities in their circle.
The Chinese bought you four weeks. Probably enough time to ramp up production of some critical equipment, begin rationing others, figure out protocol, and overstock supermarket shelves.
This mess is on the United States, and the US alone. And under reasonably hygienic conditions, people have a right to eat whatever the frick they want, by god; to impose otherwise reeks of cultural genocide, especially for cultures for whom food is more central than religion.
OTOH, given the relatively low death rate of the virus and the difficulty, high human and monetary cost, (and seeming pointlessness) of containment, the economic costs of a heavy handed response may well outweigh the health benefits. The US and Japanese response might actually leave their societies healthier in the long term, so a limited response might have been strategic rather than incompetent. It sure as hell looks incompetent, though.
From the SARS experience, East Asia really really likes masks. Masks provide limited droplet protection in the crowded streets of east asia, and stop you from touching your nose and mouth – very important. Also psychologically reassuring for the population.
The Chinese don’t even eat bats; that part of the post probably wasn’t entirely serious. The Fijians do, but those bats aren’t implicated. But if the Chinese DID eat bats, and bat coronaviruses kept getting into the human population as a result, I’d say that this clearly was NOT “under reasonably hygenic conditions”. And “cultural genocide” is a dumb term, designed to conflate mass murder with the restriction of cultural practices.
As for the idea that the United States is somehow entirely at fault, that’s a stretch probably even Noam Chomsky couldn’t justify.
I meant the outbreak within the United States is the responsibility of the USA, not the global outbreak.
And yes, it is a dumb overblowing alarmist term. It happens to be accurate. Restriction of cultural practices may or may not be justified, but it is destructive to cherished aspects of culture and can elicit visceral defensive reactions. I don’t eat bats or dogs, but I would defend one’s right to do so. I hate female circumcision as much as the next guy, and i would have it banned under individual choice mandates (which override cultural mandates), but I would still consider it cultural genocide.
Consider “taxation is robbery”, “conscription is slavery”, “abortion is murder”. Sure they are. But robbery and murder are acceptable under some circumstances, e.g. by the state or when the thing murdered is not capable of much suffering. Infanticide is a lesser crime than murder, after all.
And yes, you can catch diseases under reasonably hygienic conditions. It just depends on how often they pop up. It’s never a 100% reduction. That’s a curve, and my threshold on it is higher than yours.
Scott wrote a nice article about this kind of thing once, calling it the worst argument in the world.
Sure, but there are two possible responses to realizing that people are trying to pull that sleight of hand:
1.) Denounce them for a bad argument
2.) Admit and own the dysphemism, and say that the category isn’t uniformly deserving of rejection; it’s central members aren’t bad simply because they belong to that category.
To provide an example: imagine an ancap saying that ‘Taxation is Theft!’
You could say that they should stop using the word theft; while technically taxation is theft, you consider it non-central and far less reprehensible than its central members. The ancap will likely reply that he considers it indistinguishable from the central examples and ENTIRELY reprehensible. This approach has turned an apparently-object-level discussion into a semantic discussion.
Or you could approach it by accepting their terminology and rejecting the negative affect. Yes, taxation is definitionally theft, but theft isn’t wrong because of its definition. It’s wrong because (insert consequentialist/deontologic/utility argument here). The ancap will likely reply with a refutation based on a different moral argument (consent, perhaps.) Here, you’ve converted an apparently-object-level discussion into one about how how we define morality… which is where the fundamental disagreement lies.
Which is better? The semantic discussion or the moral one? It depends on context. It would be REALLY nice if ancaps stopped using words with negative affect and making people work to accept dysphemism. That tactic is of the Dark Side. But on the other hand, the second approach renders you far less vulnerable to words with negative affect on an personal level, and expedites this particular conversation to it’s most meaningful framing.
@pacificverse is doing the second approach here. He’s accepting the dysphemism ‘cultural genocide’, and rejecting that having that label always makes it evil.
Not legally, it isn’t. And I could easily walk up behind you, shoot you in the back of the head, and you would not suffer at all. Is that then acceptable?
You are not the state, and I am capable of much suffering, dude! (dudette?) (Unless you happen to be royalty, in which case you are still not royalty from my country, so you have no executive power over me)
We murder millions of cows and chickens every day, and governments rob each and every taxpayer, but these are good things because they put protein in our diets and teachers in schools! The benefits outweigh the costs!
I really need to work on my wording…
Why does it matter that you are capable of suffering, if you do not in fact suffer?
It might be cultural genocide, but the Chinese are doing it: https://www.scmp.com/news/china/article/3052151/china-bans-trade-eating-wild-animals-battle-against-coronavirus
Cultural sui-genocide.
Or we could combine it with mocking cultural appropriation and shallow orientalism, and call it cultural sudoku.
I’ll go on record as saying the Metaculus estimate is insanely wrong. 99%-ile on global deaths in 2020 should be something like 10,000.
If you want to go on record, I encourage you to make a Metaculus account and post your estimate there.
I’m OK with this being my record.
I think it’s insane to trust the mortality rates out of China over those of S. Korea. It’s almost certain that the denominator from Korea is way more accurate.
I could buy that as a reasonable median, but you seriously think there’s less than a 1% chance of 10 million people being infected worldwide? That’s an incredibly confident statement that it’ll infect fewer people than the flu, despite 1) it appearing to be more contagious and 2) nobody having built up immunity to it. What’s your basis for thinking (with such high confidence) that the global infection rate will be low?
We’re all going to die and we’ll deserve it, NYC edition.
A NYC school teacher went to Italy and is now showing symptoms of coronavirus. She was back in school for days, quite likely infecting other students and teachers.
They’re NOT EVEN CLOSING THE SCHOOL. WTF? You’ve got a population which likely includes infected and contagious individuals, and you’re going to continue to bring them all together?
Yeah, our response has, in general, been like that. You have symptoms of the virus, but you haven’t visited one of these three countries recently? No test for you! Oh, yes, we know there are cases elsewhere, but these are orders from higher up based on the situation last week, and we insist on following them.
We may yet be saved by the change of the seasons, when it gets warmer. But it won’t be because we handled this well here in the US. I think only Iran really has us beat for incompetence, here.
There have been other NYC cases where they DID close relevant schools, workplaces, and in one case a synagogue. They closed the schools in Washington State where cases were discovered. This is a specific case of extreme incompetence (probably from the NYC schools chancellor).
The ineptitude of the early handling of SARS-CoV2 testing in the US is really striking, coming mainly from two government agencies (CDC and FDA) I generally think of as pretty competent. This makes me wonder how much other dysfunction and ineptitude is hiding out in those agencies.
Follow up: that particular person was negative for SARS-CoV-2. NYC really lucked out, I think.
I started a little list of coronavirus risk reduction tactics for my extended family, but it occurred to me others may want to collaborate on such a thing, so here it is. PRs welcome.
The number of coronavirus cases in China has been declining for weeks. Many people assume that China is lying about the statistics, but now it appears that the number of cases in Korea (the country with the second most cases) is also slowing and gradually reaching a peak.
This confirms the Chinese statistics, and suggests that the same results can be achieved in Western countries (democracies with individual rights), and a pandemic avoided.
South Korea started getting serious as soon as people started dying, though. China didn’t take action until 7-8 people were dying every day (SK never even got that far). Currently, Italy is long gone (40-50 deaths/day), while Washington state needs to start serious quarantine measures VERY soon to have any chance of containing it (3-4 deaths/day).
https://imgur.com/a/x5Ql8l8
This story highlights the issue with not having the ability to test many people–a cruise ship with several thousand people on it had a passenger die of COVID-19, and the California health authorities are planning to test only 100 or so of the people on the ship.
Questions I have which I hope someone already knows the answers to:
a. Is it known how long after exposure you need to wait to get a positive test result? Like, I’m pretty sure if I walk through a cloud of your airborne sneeze droplets and then someone tests me five minutes later, I will test negative. How about the next day?
b. Is anyone doing antibody tests to measure whether there are substantial numbers of people who’ve already been exposed and recovered?
I also have this prediction: At some point, manufacturers will get ahead of the mask shortage. We will then see a pivot of public health types asking people to start wearing the surgical masks, especially if there’s any chance they might be contagious. Establishing a norm that anyone coughing/sneezing/unwell and out in public should wear a mask would be a win for mankind, and would also slow down the spread of the virus. My impression is that it probably won’t protect you much (other than keeping you from touching your face), but if all the asymptomatic carriers were wearing masks and squirting hand sanitizer on their hands once an hour, they’d leave a much smaller trail of sick people behind them!
As for b), I have been given to understand that an antibody test does not exist at this point in time, and that people are currently relying solely on antigen tests for diagnostic purposes. This is needless to say a very unsatisfactory state of affairs.
According to this CDC page, they currently are doing a test using PCR on samples (from nasal swabs, I think) to determine if there’s an active SARS-CoV2 infection, but they’re working on a blood test for antibodies. That would tell us if you’d been exposed a couple or three weeks ago, and it would be really useful for letting us know what fraction of the population had already been exposed and never noticed. It’s conceivable that once they do that, we’ll find out that it’s already circulated extensively and our current CFR estimates are wildly wrong, or that hardly anyone’s been exposed yet and the scary CFR numebrs are close to accurate. But it takes a couple weeks to start making antibodies after you’re exposed, so it’s not so useful for deciding if you’re currently infected.
A little web searching didn’t show me anything that said how soon after exposure you’d expect the test to be positive–I’m guessing it’s the incubation period, which I think is sometimes as short as a few days but might be as long as 14 days. But I’d love to hear from people who know more.
Singapore has successfully used an antibody test to identify two recovered minor cases of COVID-19 (where the person was a close contact of a confirmed case, had symptoms but not serious, and recovered without hospitalization). Here’s their original press release on it: https://www.moh.gov.sg/news-highlights/details/links-established-between-church-clusters-and-wuhan-travellers . There was another such case detected in the last few days.
They aren’t (to my knowledge) doing it widespread, though, which suggests that maybe it’s a pain in the ass (or maybe that would just take away resources from testing actual sick people).
I have a relative who does Meals on Wheels for older people. He delivers meals to the doors of senior citizens who are often cut off from other human contact. Also, he is stubborn and largely scoffs at prepping.
My question is two fold:
1. What precautions should he be taking?
2. More importantly, and this should feedback into question 1: what is a good way to convince him to take these steps? I cannot guilt him or scold him. He may be convinced with high-quality information from reliable authorities, though.
Not even by pointing out that it is his beneficiaries who are likeliest to suffer?
Not if he doesn’t believe it to be true.
I can probably convince him with facts, though.
This is a dude who should be wearing a mask, in case he’s carrying the virus. Some fraction of people as asymptomatic or feel like they’ve got a mild cold, but are shedding this virus that’s liable to kill an older, sicklier person who catches it.
What information can I use to convince him? Also, he may have problems acquiring masks, although I could ship him some if I got them.
He doesn’t come in and chat with them, usually just hands it to them through an open door.
For handwashing, how often do I need to wash the cloth towel I use to dry my hands?
What if multiple people in the household are using it?
Depends on your confidence that everyone using that towel is washing their hands properly. If they only rinse, no soap, then the towel is tainted.
The bigger question is if you touch the bathroom doorknobs on your way in and out. Even if the towel is clean, if you aren’t using something clean to open the door, you are immediately reinfecting.
On that same note, should we be wiping our keyboards and mice with alcohol every time we come back from the bathroom?
I hope Churches are pouring wine from the chalice into plastic shot glasses or something for each person.
Common practice; my concern is the “bread” part 🙁
Mine stopped the wine a month or two ago because of the flu season. No handshaking or handholding since last weekend.
True believers wouldn’t.
How could the blood of Christ harm anyone?
isn’t that whole “is this really, literally the blood of Christ vs. no, of course this is actually wine, it’s a symbol for Christ’s blood” something that’s controversial/differs between different versions of Christianity?
Yeah. Doctrines of transubstaniation (and the consubstantiation believed in by the Lollards) kind of assumes an aristoteliean view of metaphysics where the essence of the wine can be replaced with the essence of blood without the ‘form and accidents’ of wine changing.
Then Martin Luther called the whole thing bollocks and tens of millions killed each other with pike and shot etc.
No — I grew up Lutheran, and Luther very much considered the Eucharist to be, in some genuine and non-symbolic sense, the body and blood of Christ. The Lutheran doctrine isn’t exactly the same as Catholic transubstantiation, but it’s much closer to that than to the “lol it’s a metaphor” approach common among other Protestants.
Yeah. I think I was getting quotes confused between Luther and Calvin.
The latter — it’s considered literal by Catholics and metaphorical by Protestants. (Not sure about Ortodoxes, AFAIK the former.)
No. Catholic theology acknowledges that the contents of the chalice have the same physical effects as if it was ordinary wine. Just as it tastes like wine, it would make you intoxicated if you drank enough of it, and it can make you sick if it’s contaminated. It’s very common for Catholic churches to stop offering the cup during epidemics or just during cold and flu season in general.
Proposal: Put the blood of Christ in a silver squirt gun and perform the Eucharist without any risk of viral transmission.
Lambert:
We kind-of do that with holy water, once in a while. Though it’s a kind of shaker thing instead of a squirt gun–the priest walks through the church and splashes everyone with drops of holy water.
What do you think about losartan? https://www.bmj.com/content/368/bmj.m406/rr-2
A lot of people are saying this might mean Covid-19 “recurs annually” like the flu. This is bizarre to me and did not fit my preconception of epidemiology. Bubonic Plague had generational, but not annual recurrence, but after a few centuries this cycle became a muted non-emergency. Influenza has been around for thousands of years, but I gather we are not seeing a “once in several hundreds years” event wherein a new virus is added to the pool, a pool which only grows bigger and does not drain at any steady pace. How does this work? Will Covid-19 be “muted” in danger over time, or will that only happen in the very long term because of natural selection? How much worse would it make, say, the 2050 flu season if it did recur? When was the last time a major novel virus became recurrent?
I’m sort of just trying to understand how something that I thought was at long-run equilibrium (human immune systems vs. viral infections) could suddenly be knocked back into a much worse New Normal
1918 H1N1 Spanish Flu lasted only a year. SARS (a coronavirus) vanished. MERS (also a coronavirus) became endemic in some countries. The two coronaviruses which cause ordinary colds (OC43 and 229E) are endemic worldwide. The other two are also, I believe. I don’t think the reasons for the differences are well-understood.
Does anyone know a reason that RT-PCR tests can’t be adapted to run on large mixtures of samples? If you have a test that tells you whether virus is present in a given *set* of samples you can identify K positives from N samples with K log (N/K) tests. I don’t think dealing with imperfect tests makes this protocol too much more complicated. This should make it possible to screen huge populations with relatively limited testing resources. I can’t be the only person to think of this, so what are the obstacles?
You’d need more sample material, for one, which would increase the logistical burden, and the testing procedure would be substantially more complicated. Also, I’m not sure I buy your big O, there – think about happen when N = K.
I’m assuming you start with an estimate of log K, and start your search with samples that have about one expected positive, so if K=N you just test each sample separately. If you don’t know anything about K I imagine you can get an estimate with just an extra O(log N) tests, or just start at the top and do O(K log N). This technique would seem most worthwhile in the early phases of an epidemic when K<<N, so basically you are doing K log N tests anyway.
Maybe you need to do more cycles of PCR to deal with a more dilute sample, so the cost would technically have a log^2 term?
Lets say the sample procedure is to take a nasal swab rinse in a buffer and use some of the buffer as a template for the RT-PCR test. If you try to rinse say 8 swabs in the buffer you could be adding RT-PCR you could be increasing the concentration of RT-PCR inhibitors and at the same time the additional swabs might pick up some of the target that was previously in the buffer, so you might end up with a false negative for the set.
I think my proposal is: rinse each swab in a separate buffer, then pipette a bit of each buffer into a mixed sample. So ideally it should just be dilution. Obviously ultimately it would be nice to have a machine to do this.
If people either had a high viral load when they were infected or no viral load at all then dilution may not be a big problem. If we believe that that the virus might be present at low levels for a couple of weeks before becoming symptomatic then that is a problem.
Re the Spanish Flu, the cdc says:
An estimated one third of the world’s population (or ≈500 million persons) were infected and had clinically apparent illnesses (1,2) during the 1918–1919 influenza pandemic. The disease was exceptionally severe. Case-fatality rates were >2.5%, compared to <0.1% in other influenza pandemics (3,4). Total deaths were estimated at ≈50 million (5–7) and were arguably as high as 100 million (7).
Link
Isn’t 2.5% the crude mortality rate, and isn’t the case-fatality rate ~ 10%?
Speaking of Zinc, anyone have any opinions on garlic?
https://examine.com/supplements/garlic/
Today I ate some doughballs where the garlic butter was inside the ball and I must say, they’re not half as good as the normal sort.
It’s plausible that vampires were the missing link between bats and humans that allowed zoonotic transmission to occur.
Common foodstuffs that reliably prevent or cure disease in modest quantities are like $100 bills lying on the ground.
As soon as it gets noticed (vitamins, chinchona bark, willow bark, foxgloves) the medical community isolates the responsible compound and manufactures it on an industrial scale.
Zinc is required for thymus hormone activation. Thymus hormones drive immune production/differentiation of T-cells. It’s reasonable to expect zinc to boost short-term immunity.
Should people be encouraged to get flu shots right now?
Flu season is coming to an end, but if there are fewer cases of the flu then there will be fewer cases of worry and self-misdiagnosis in the future.
No, because flu shots often cause flu-like symptoms which will cause worry and self-misdiagnoses and also perhaps result in missing diagnoses of real cases.
@ The Nybbler
This seems at odds with a recommendation by the CDC:
link text
I’m aware of the CDC’s love for flu vaccine; I disagree, and I don’t think their own numbers support it.
Bottom line:
When they’re NOT well matched, which happens often, effectiveness is far less.
The CDC doesn’t consider the downsides of the flu vaccine (flu-like symptoms) to be significant. I disagree, and don’t consider halving the risk of actual flu to be worth it.
How often is often, and/or does this depend on the person? Because I’ve never had this effect – if I get it somewhere where the person doing the injection is good at it, the worst I get is a slight ache in that arm for a couple days – and I’ve done it pretty regularly for the past eight or so years.
If it does depend on person, might be worth considering your personal likely downsides. I would gladly have two days of my arm being slightly sore in exchange for halving the risk of actual flu – but I may react unusually well to the shot.
There are two issues: normal years and this year. The first two comments were specifically about confusion with coronavirus, the OS saying that that the shot would decrease confusion and the Nybbler saying that it would increase. That is not at odds with the CDC’s recommendation for a normal year, because that is a different topic; although he also disagrees with that.
The CDC recommends flu shots, but other countries do not. For example, NHS does not for most adults. It seems to me that the only organization serious about cost-benefit analysis in medicine is NICE. I’m not sure they have assessed the flu shot, but I’ll take the NHS guidelines over the CDC just on the off chance that NICE is involved.
People are talking about flu shots for healthy adults?
I read the comments about it and was like ‘yeah, I’ll check my grandparents are getting their flu jab this year’.
Most under 65’s don’t get free flu shots under the NHS.
My workplace offers free flu shots for all, at the workplace, and this is a fairly standard thing in similar jobs in this area. The workforce skews young, but they don’t want any of us off work.
Being over 60, I get the flu shot every year, either from them or from my regular doctor, whoever offers it first. But so do lots of the younger people.
Wow, I was surprised to learn that most people don’t get flu shots overseas. In the US, adults are expected to get flu shots every year, and a lot of companies offer free flu shots to employees. It didn’t even occur to me that other countries would be different.
@ Douglas Knight
From what I can tell, the recommendation is posted on the CDC page dedicated to COVID-19, under the section “CDC Recommends”. They must think it is worth it *this* year.
@ The Nybbler
What you say seems fine to me. I don’t have a good argument either way, I was just pointing it out for the benefit of the discussion.
AliceToBob,
Sorry, I didn’t notice that was the coronavirus page. But I would have written much the same if I had, because I don’t trust the CDC to think. If they had given reasons, I would look at them, but they didn’t. Most likely the web page was the result of a mangled copy-and-paste: someone was instructed to copy flu advice to the coronavirus page because much of the advice is similar and failed to think through the parallels. Indeed, the page has now deleted the vaccine advice and says
My understanding is that the flu vaccine is kind-of-marginal–it’s not all that effective in the best of times, and some years they get the strain wrong and it’s not helpful at all. It still seems like a net positive, and I get it every year (so do my kids!), but the only reaction we ever have to it is a sore arm for a couple days.
It isn’t eating bats that’s the problem. The problem is that China has busy “wet markets” that a billion people pass through every year and that sell live animals, which can pass their diseases on to humans. Just banning the selling of live animals would fix a big part of the problem.
But the point is moot because China announced that it’s permanently banning the trade and eating of wild animals: https://www.scmp.com/news/china/article/3052151/china-bans-trade-eating-wild-animals-battle-against-coronavirus
It’s of course possible that you are today safer from this virus than you ever will be. That any form of prepping or paranoia may appear silly when looking back.
I recognize that Jon Chait has a bad case of Orange Man Bad syndrome, and yet I’m struggling to find a more charitable explanation of these comments than his. Has anyone got a better explanation?
The tweet at the top gives you the most likely explanation — Trump is trying to find a silver lining to the coronavirus.
Simple enough: Trump is claiming that if it weren’t for the coronavirus, the Dow Jones Industrial Average (which, regardless of whether it is the best measure of the stock market or not, is widely recognized) would be at 30,000. He’s saying he was doing great until this unpredictable setback.
True but meaningless, very typical Trumpian blather, but not different in kind from other politicians.
More of the same blather, plus some re-assurance that even with the virus, the market isn’t hurting _that badly_. Chait makes the point that the stock market isn’t a great barometer of the economy. But Trump knows a lot of people (even people without investment portfolios) take it as such — mostly because as was discussed here in previous threads, it’s a very quick-reacting measure of the economy. Nothing else moves as fast.
Chait complains that Trump isn’t clear here, and he certainly isn’t grammatically unambigious, but I think it’s easily understood that he means the coronavirus might have an impact on the economy.
Chait complains that Trump’s protectionism is economically naive, and he’s probably right in the long term. But some US companies actually have seen a windfall in the short term; here’s an article about NYC garment district manufacturers getting a windfall from a drop in Chinese capacity. There’s also things like 3M ramping up mask production. Chait would probably argue that this is broken-windows reasoning, and he’d be right. But the short-term boost for some is real enough, and only some of the losses are domestic.
Basically what any politician would say, and probably what they should say (even if it’s incredible annoying). Panicking isn’t going to help.
So… pretty typical Trump. Some self-aggrandizement, some pushing of his protectionist ideas, and a lot of blather. Maybe a little worse than your usual politician, but not by any large degree.
I feel like this has become so obvious in the last few years that I don’t understand how it’s not the main focus of the rationalist community, or just smart people online in general. We’ve learned the art of “how not to find the coconut on Coconut Island,” as Taleb says. The discussion of how to deal with a world in which this is the case should be paramount.
What’s the issue here? Health workers, who need to know, have the full picture. Stupid people are discouraged from doing stupid things. Online rationalists are frustrated in their search for “the truth”, but that doesn’t kill anyone.
A Zinc datapoint:
“- #COVIDー19 has a Zinc receptor. As such, Zinc supplements must be stopped, while masks containing Zinc could be useful.”
https://twitter.com/aliostad/status/1236571657436790786?s=20
1. This tweet is unavailable now.
2. What?
Given the shortage of purell style hand sanitizer, I tried to find an alternative. I have a kid-safe toy disinfectant that says it kills “99.9% of viruses” including the flu and common cold. The active ingredient is 0.017% hypochlorous acid. In this spray, it says it is safe to spray on kids toys and let it dissolve without any rinsing or wiping needed. Some uninformed google searches seem to imply that it is promising since it is actually used for cleaning skin for wound care and acne purposes, but I am neither a chemist, biologist, not medical doctor.
This thread is the best place I could think to ask if this is legit, without seeming like some kind of nutcase. Thoughts?
Sounds like it’s basically bleach-type stuff that’s less concentrated than household bleach but more than swimming pool water.
Some beardy youtuber guy recommends 0.1% benzalkonium chloride. But apparently studies show it’s not great against COVID-19.
Everclear at the correct concentration will also work.
The World Health Organization has you covered; I’ll assume most people posting here can scale down from their ten-liter batch size and/or convert to customary anglospheric measures.
Things have begun closing down here in Silicon Valley. Group gatherings are cancelled, down to the level of my local bridge club. I’m WFH – not yet officially “for the duration” but I can’t see them actually switching back after telling us to WFH last Friday, whatever they claim. I’ve so far encountered no evidence that justifies the reaction, but at this point it’s got momentum, and Joe and Jane Random are publically encouraging outliers to join in the so far voluntary shutdown.
The surprising thing is how it makes me feel. The chronic dry throat/stuffed head I’ve had since before Covid-19 had a name suddenly seems like it might be Covid-19. I felt like I was taking a risk by collecting the library book I’d had on hold yesterday. Maybe we should be careful about walking the dog, or stop doing so. Etc. etc. And all are just as low risk as they had been the day before, at least based on all the information I’ve encountered to date.
I guess I’m just as human as the next person ;-(
But meanwhile, I’m really glad I bought a lot of non-perishable groceries last weekend. I’ve no idea what will be available today – and more importantly, what will not be.
I think the issue with coronavirus isn’t being explained properly.
It’s not a big problem for the majority of people individually, but it’s potentially a big problem globally. Worst case scenario, half the population gets infected. At a 1 percent fatality rate, that’s 40 million deaths. That’s a big deal, even though it’s not a big individual problem for everyone else.
Wouldn’t that be much like the great influennza pandemic at the end of WWI? I’m not sure how much explaining that needs.
OTOH, I’m old. That epidemic was well within living memory when I was a child; I know which relatives died in it. And I’m also a student of history.
Maybe this needs a fair bit of explanation to younger people who aren’t interested in history.
What with all the panic bog roll buying?
This is a respiratory infection, not dysentery.
Because early “how to prep for coronavirus” articles talked about how Wuhan residents were missing toilet paper, and in some areas this became a meme, and once you see empty shelves without TP your hoarder skills activate.
I’ve had no problem finding TP in the Southeastern US. The store is even giving me coupons and putting it on sale. But Australia is having panics about it. You can probably back-trace the reason this happened in some places and not others down to some kind of irresponsible reporting (either by professionals in the media or amateurs on social media).
It is a pretty standard item to purchase as part of disaster preparedness, especially in cases of disease where personal cleanliness will be critical. Also, it is not very dense, and takes up a lot of shelf-space compared to unit size when compared with stuff like food or medicine so shelves empty faster and it is more visible in the shopping carts of people stocking up. I don’t think there’s any serious TP shortage in the overall supply chain (unlike masks or hand sanitizer), it’s just that stores keep less of it on shelves/in storage cause it is so dang bulky and takes up so much space.
Forget mild symptoms, how possible is it to contract the virus, (test positive) and overcome the infection (and test negative) without ever developing symptoms?
What ever happened to the asymptomatic people in that cult in Korea who tested positive? Did they recover with, or without, symptoms? I can’t seem to find anything on this.
Egypt seemed to have 45 cases, all asymptomatic, on a cruise ship. And then 11 of them test negative. (Recovered?)
Given that these assertions are true, that many people can completely asymptomatically recover from the virus, and the virus spread is way larger than realized… is this a good thing (virus is a lot milder for most people than previously thought, case fatality rate is way lower), or a bad thing (virus has spread a ton more than expected, numbers are somehow ever more off than we expected)?
Has there ever been an infectious disease this weird before?
I wonder if there’s a lot of mutation of different strains, with different prognosis for the different strains….
Only a small minority of cases (under 18%) are asymptomatic, and asymptomatic cases are probably not infectious in normal circumstances. A lot of the people considered asymptomatic became symptomatic in the following days. So no the virus is not quite so weird, we are just in a “dynamic” situation where a lot of ideas are published before they can be fully verified.
The <18% number is based on a model. The >50% number is based on measurement. Ideally someone would follow up on the asymptomatic Diamond Princess cases and find out if the model was accurate.
Are you sure that the “Age Distribution of Hospitalization” is reporting % of total cases?
I suspect that it’s something like percentage of persons hospitalized, but I was unable to find the original source. Could you please add a link to Gottlieb’s original post/analysis? Thanks.
Re: the coronavirus dashboard link in the OP-
1) its domain and extension are not “jhu.edu” (unlike the map I reach via a google search on “JHU coronavirus map”)
2) A family member who works at NIH received a few hours ago an NIH email stating that a malicious website pretending to be a live map for Coronavirus COVID-19 Global Cases by Johns Hopkins University is circulating on the internet, and that visiting the website infects user’s computer w/ an info-stealing program which can exfiltrate a variety of sensitive data.
If link in the OP is indeed malicious, it would be great to hear suggested remedial actions.
The jhu.edu page on mapping 2019-nCov links to the same arcgis.com app as Scott’s post.
Ah thx Faza.
Link to CDC page on Coronavirus testing. They say they’ll keep it up to date. Should be helpful for keeping an eye on the testing capabilities of the country, which should effect quarantine efforts.
According to this paper, the Virus still survives up to 4 hours on Copper. This might be important to clarify, since I myself thought that it kills them immediately.
https://www.medrxiv.org/content/10.1101/2020.03.09.20033217v2?fbclid=IwAR3uhuRTLd8HKWtppzsLKPQxp0zaNmdsT8-IYepJu4v8–Vl43FtaVfjuZQ
Metacalculus’ total fatalities prediction has been rising daily. The current median is 2.98M.
Scott: very entertaining article, although I disagreed with the general poo pooing of the CDC, FDA, etc. Not that they haven’t handled this terribly- of course they have (most likely incompetence, but possibly intentional in order to avoid testing and therefore reduce “panic”). But treating this as “government regulation, screwing things up again lol” seems the worst point that could be made given the obvious success of the Chinese government at containing the virus relative to more open societies like europe and the US. If there’s one thing totalitarianism can do much better than democratic capitalism it’s contain a pandemic.
Ultimately, this virus- and the efficacy of “totalitarian” top down strategies at containing it (and the complete inability of western countries to do so) represents a greater threat to privacy, freedom of speech, freedom of movement, etc than anything else I’ve seen in my short life- including 9/11. If we develop some treatment or cure quickly it could be a huge face saving moment, but if millions die in the US and Europe while our stock exchanges go lower than 08 lows, the age of democracy and free markets may actually be on it’s way out as we wake from our liberal slumber to the reality China already sees. Because, while free societies are better at some things, they are not better at controlling something like this. At least not in the way they are currently organized.
PS- south Korea is democratic and capitalistic but has also been able to contain its outbreak (using strategies similar to China’s but very different from Italy’s strategies and europe/ the USA’s current strategies). So this doesn’t have to be some capitalism vs communism showdown reminiscent of the cold war. But the effective strategies South Korea has used (using personal data to track cases, masks, widespread testing, disinfecting public transit) have not, suffice it to say, been “laissez faire.” The FDA and CDC might suck, but not bc theyre government organizations. The Chinese and South Korean versions of these institutions have handled this much better, and they did so not by deregulating the f out of everything.
Regulation is not the same as government. Scott is making distinctions here.
That is an interesting point/ direction of inquiry. What makes certain government action (or attempts at action) more inefficient (or even laughably incompetent) than others? Why can China build a hospital in 10 days and the US can’t create test kits or simple face masks? The common sense libertarian arguments of “governments are inefficient because they don’t have competition/ market pressures” do explain SOME of government inefficiencies, but when you see the vast variety in government’s capacity to get some things done versus others these explanations seem insufficient.
It seems that perhaps another significant piece of the puzzle is that governments who restrict what they can and can’t do (rule of law, human rights, etc) face certain inefficiencies due to these self-imposed restrictions.
Anyways, I’m getting very far from Scott’s original piece which provoked this line of thought. Thanks for the feedback-
pjiq
This stuff truly is mind boggling. I run a local business and it’s crazy how much this COVID-19 stuff has turned my business upside down. Now it’s not all bad, we’ve adjusted to the situation slightly and hope things will pick up here soon. But this “social distancing” has definitely shocked our workers as we typically deal with customers in their home.
We’re now in a time that I’m honestly a little nervous for myself and my smaller business. I would assume I’m not the only one who looks at this from a long term perspective. And that is if we don’t see the end of the tunnel soon here in the next few weeks, many businesses are going to feel the pinch and struggle.
Even the news sites are putting the stories out there about it:
https://www.usatoday.com/story/money/2020/03/24/coronavirus-marketing-data-firms-small-business-cut-jobs/2902286001/