
As before, feel free to treat this as an open thread for all coronavirus-related issues. Everything here is speculative and not intended as medical advice.
How many real cases?
As of today, the US has almost 10,000 official cases. How many real cases per official case?
One epidemiologist says 8x. In this US News article, scientists estimate 9000 true cases back when the official count was 600, suggesting 15x, and BBC estimates 10,000 real cases in the UK to 500 official ones, suggesting 20x. A study in Science (article, paper) estimates 86% are undetected, for about 7x. So it seems like most people are converging around 5 – 20.
Probably this number is different in every country, depending on their test rates. You’re probably all already following the map of cases per country, but you can supplement with this map of how many tests each country is running per million people (h/t curryeater259 from the subreddit)
What about the evidence from famous people? If only 100,000 Americans are infected, it’s pretty weird that it would hit both Tom Hanks and Idris Elba (also, Tormund from Game of Thrones). The Atlantic makes this case more formally. Given that Iran’s vice-president is affected, what are the chances that only 1/12,000 of Iranians had the virus? Some people calculated it out and found that hundreds of thousands of Iranians must be affected for the prevalence among politicians to make sense, suggesting ratios of 100x or even 1000x.
I’m skeptical. Famous people travel a lot and shake a lot of hands. And they mostly interact with other famous people, forming their own little “compartment” where the epidemic can be worse than in other societies. I think it’s more likely that Hollywood actors and Iranian politicians have 100x higher risk than their host population, than that epidemiologists are wrong about the size of the epidemic by orders of magnitude.
We still don’t have an endgame
A brief flurry of interest last week as the UK seemed to be trying a different strategy from everyone else – isolating their oldest and most vulnerable citizens, but letting everyone else get the virus to build herd immunity. They’ve since backtracked after people did the math and found that an epidemic even among healthy young people only would overwhelm their medical system. Here’s another critique of herd immunity, appropriately enough on UnHerd.com.
But the UK’s original point – that without herd immunity, all we can do is continue the lockdown until something happens – remains sound and worrying. Everyone is hoping for a quick vaccine or antiviral, but this is a field where “quick” sometimes means months or years instead of decades. If we don’t get a deus ex machina, eventually somebody will need to implement some long-term strategy.
Last week I predicted that this might look like titrating quarantine levels – locking everything down, then trying to unlock it just enough to use available medical capacity, then locking things down more again if it looked like the number of cases was starting to get out of hand. This would eventually develop herd immunity without overwhelming the medical system. A paper yesterday out of Imperial College London (discussed here) said the same thing, arguing for alternating periods of higher and lower quarantine levels based on how the medical system was doing:
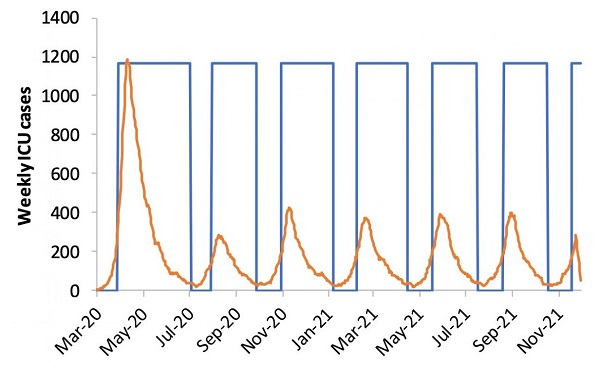
The orange line is projected ICU cases. The blue line is government-mandated social distancing levels. Relax social distancing levels, then after ICU cases cross some threshold, reinstate them again. That way at least we can have a few weeks of normal economic activity and seeing friends in between each lockdown. Control systems are the solution to everything!
Problem: it would take forever to develop herd immunity under this system, and we might just have to keep turning quarantine on and off for a year or two until a vaccine gets developed. Does anyone have any better ideas?
The closest thing I’ve heard is “what China and South Korea are doing”, which seems to be having so many tests available, and such good health services, that it’s easy to detect cases, track down their contacts, and manage the epidemic even while life goes on mostly as usual. So maybe the end date isn’t “have a vaccine available”, it’s “have millions of test kits available”, which I think looks more like a few months than like years and years.
Flatten the curve
Is flattening the curve just another name for the “have a control system to titrate lockdown levels so that only the right number of people get it at a time” strategy? Maybe everyone just assumes that we’re never going to get the cases down to too low a level, so we should try to get them as low as possible and maybe hit the right amount? And overshooting and reducing it so far that you’re not using the medical capacity you have, and wasting an opportunity to have a normal life and/or build herd immunity, is just really unlikely without China-level resources?
An article called Flattening The Curve Is A Deadly Delusion has been going around this part of the Internet, saying that there’s basically no way to match a curve of any flatness with our current hospital capacity. Nostalgebraist says the math is wrong, mostly because it uses a normal distribution when it should use an exponential one. But I’ve seen some other people making this basic point now, so it could just a be a question of how bad things get, rather than whether they’ll be bad at all.
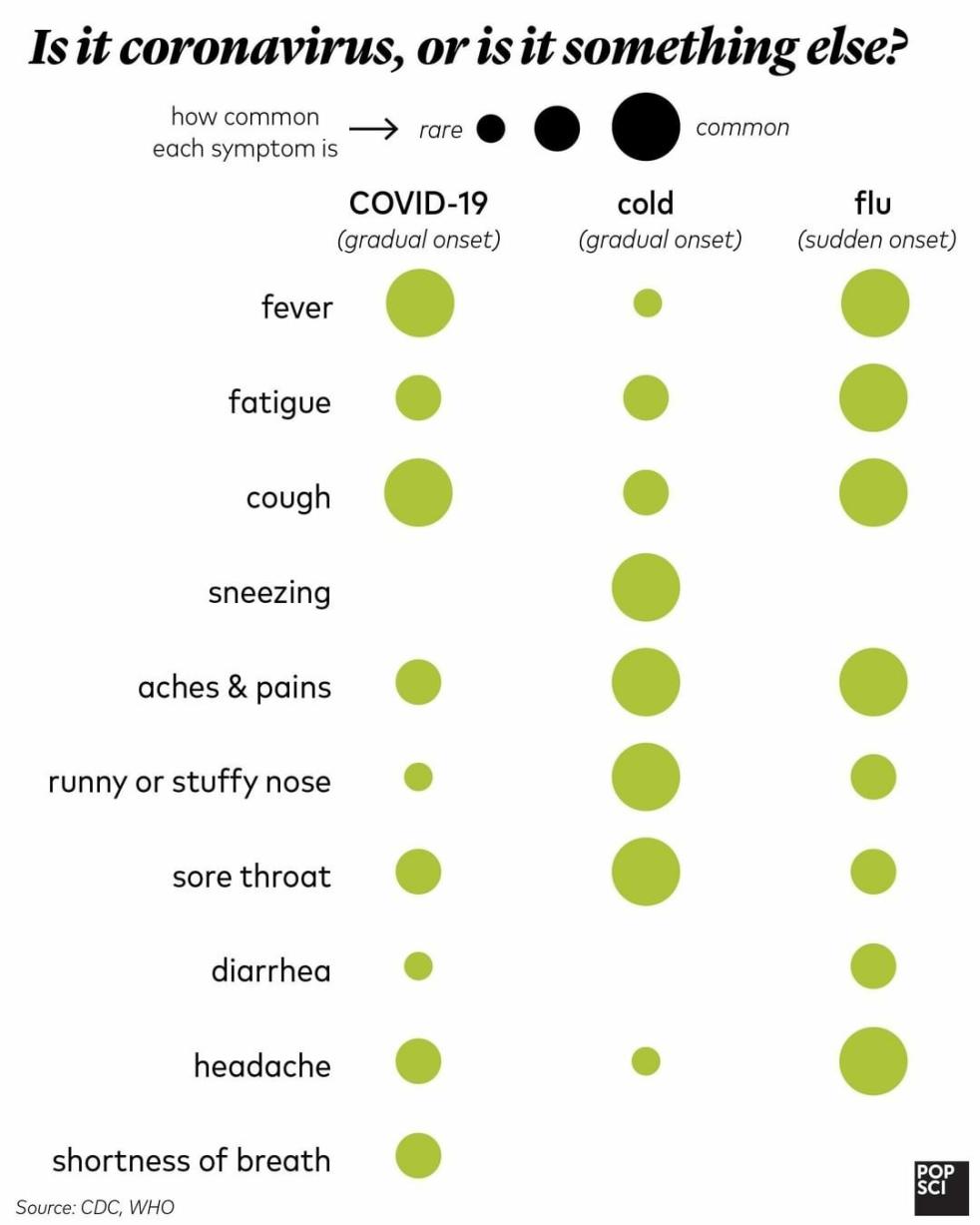
Do you just have the flu?
Courtesy of Popular Science:
Don’t use aspirin
Doctors in Germany and France are saying that a suspicious number of young coronavirus patients who end up in the ICU took aspirin or other anti-inflammatory drugs (Advil, Motrin, Aleve, ibuprofen, diclofenac, etc, yes I know several of these are the same drug, I’m trying to inform readers) before getting worse. There’s a plausible biological mechanism; anti-inflammatories dial down the immune system. BMJ agrees: Ibuprofen should not be used for managing symptoms, say doctors and scientists. Tylenol, acetaminophen, or paracetamol (YES, I KNOW) is still okay, so use that for coronavirus-induced fever.
[EDIT: WHO is skeptical, but French and German doctors stick to their guns. It seems like there’s a longstanding debate on this with the French and German medical establishment thinking it’s bad for lots of diseases, and most of the rest of the world not believing them. I have no strong beliefs about whether France/Germany or everyone else is better, but switching from Motrin to Tylenol in this case seems pretty low cost]
Ventilation
An anonymous reader writes:
Idea: for collective transport like buses and trains around the world, if they are still operating, then keep the windows open.
Actionable proposal: quickly evaluate whether this makes sense, then if it does organize somebody to communicate with relevant parts of governments and transport authorities in different countries and cities and urge them to implement, maybe first get an official looking letter that some prestigious sounding expert has signed to the effect that this seems like a good idea.
(Disclaimer: I haven’t done any due diligence or critical assessment of this idea, just firing from the hip. I heard of some study that showed somebody caught the virus on a bus from an infection person who left the bus 30 mins earlier and the two had not touched any of the same surfaces – this plus my intuitive model suggests that better ventilation could help significantly in these settings, and it would not cost anything and it would not impede any normal activities)
I’m also not sure how leaving windows open would interact with infections that spread by aerosol, but some places like Israel already seem to be trying this.
Ventilation, part 2
Right now the biggest bottleneck to treating coronavirus is likely shortage of ventilators and oxygen concentrators. Many people are trying to come up with ideas for solving the shortage. EndCoronavirus.Org is trying to get a team together, and is looking for doctors, engineers – and of course lawyers, to jump over the inevitable regulatory hurdles.
Meanwhile, at least according to Breitbart, existing ventilator manufacturers are just…not bothering to ramp up production yet? Does this make sense to anyone else? According to Forbes, ventilator manufacturers could quintuple capacity over the next few months, but…nobody has asked them to?…and they don’t want to take the initiative until somebody asks? Economists are begging the US government to ask, and maybe to ensure that every ventilator they make will get bought no matter what the circumstances are a few months from now – if they can’t, maybe private philanthropists should step in? Kudos to the UK government, which has just sent ventilator blueprints to a bunch of manufacturers and told them to get to work. But even if this comes through, how are we going to get enough skilled labor to ventilate this many people? [EDIT: As per WSJ, ventilator manufacturers are now ramping up production].
Also in medical supply news – when a hospital runs out of a critical $11,000 part and the manufacturer can’t supply more, a local guy with a 3D printer prints one up for $1. Now he’s being threatened with a lawsuit by the manufacturer. [EDIT: possibly not true or exaggerated, see here] This whole epidemic has been a fun adventure in “newspapers finally paying attention to what everything in health care is like all the time.”
Ventilation, part 3
When doctors need to ventilate someone in an emergency and don’t have time to hook them up to a real ventilator, they use manual ventilation, ie “bag and mask ventilation”, a really simple technique using a $30 piece of equipment which is literally just a bag attached to a face mask. Somebody squeezes the bag in a breathing-like rhythm, sending air into the person’s lungs until they’re able to get on a real ventilator. It’s not perfect but it saves lives.
In a New York Times article on the expected upcoming ventilator shortage, they say:
One doctor wondered if they could recruit enough volunteers to manually ventilate patients — which involves squeezing a small inflatable device by hand — indefinitely.
I know nothing about respiratory medicine, and I guess I always assumed that there were issues with bag-mask ventilation which made it unsuitable for longer than the few-minute-period it usually gets used for. If that’s not true, and the limiting factor is just getting enough people to keep squeezing the little bag, then surely our civilization can come up with some sort of automatic squeezing machine, right?
[EDIT: some discussion of why this may not work here and here.]
Come summer
The smart people seem to be going back and forth on whether the coronavirus might die down in summer like a seasonal flu. The good news is that this has sparked more interest in the absolutely fascinating field of disease seasonality:
Except in the equatorial regions, respiratory syncytial virus (RSV) is a winter disease, Martinez wrote, but chickenpox favors the spring. Rotavirus peaks in December or January in the U.S. Southwest, but in April and May in the Northeast. Genital herpes surges all over the country in the spring and summer, whereas tetanus favors midsummer; gonorrhea takes off in the summer and fall, and pertussis has a higher incidence from June through October. Syphilis does well in winter in China, but typhoid fever spikes there in July. Hepatitis C peaks in winter in India but in spring or summer in Egypt, China, and Mexico. Dry seasons are linked to Guinea worm disease and Lassa fever in Nigeria and hepatitis A in Brazil.
Their explanation for why we don’t know more about this:
“It’s an absolute swine of a field,” says Andrew Loudon, a chronobiologist at the University of Manchester. Investigating a hypothesis over several seasons can take 2 or 3 years. “Postdocs can only get one experiment done and it can be a career killer,”
As for the coronavirus itself? Unclear. The latest study says it might be seasonal, but a lot of comments on it point out continuing epidemics in tropical countries like Malaysia (currently 900 official cases). If your hometown isn’t going to get warmer this summer than Kuala Lumpur is right now (95 degrees at time of writing), you may not quite be off the hook.
John Ioannidis says we need better data
I mean, of course John Ioannidis would say that, he says that about everything. But his column in Stat News is actually pretty interesting. He points out that our mortality rate statistics use diagnosed cases as a denominator, and (as mentioned above) we barely have a clue what the real-case-to-diagnosed-case ratio is. Based on his calculations, the confidence intervals for the mortality rate are so wide that it could still be lower than the average seasonal flu (he’s not saying this is definitely true or even plausible, just a possibility). He calls for testing of a random sample of the population to help pin down better numbers.
Hail the Bay
I’m usually pretty harsh on Bay Area governments here. So I want to give credit where credit is due: they’ve reacted to the coronavirus epidemic with a level of swiftness and ferocity they usually reserve for attempts to build new housing. While New York and Seattle dither, the Bay Area (despite having fewer cases than either) has instituted a shelter-in-place order, essentially banning people from non-essential leaving the house. I think they’re the only people here who are going to come off looking really good in the history books (and hint to the 2024 DNC, SF Mayor London Breed looks pretty presidential right now). Most of the people I talk to (including patients from all slices of life) are cooperating enthusiastically and feel well-taken-care-of.
I’m even willing to give California state government a little credit. For the past week, most of the organizations that usually try to thwart me have instead been working to make my job easier. The state’s medical board usually puts onerous restrictions on telepsychiatry – for example, before you can prescribe a telepsych patient a controlled substance, you either have to meet them in person once or get a signed note from a doctor who has. Now they’ve lifted all of those and made video appointments a lot easier.
And the same is true of local businesses. I have never used the words “flexibility” and “insurance companies” in the same sentence before, but they have been positively pleasant to work with this past week as I try to navigate the difficulties of switching everybody to video appointments ASAP.
My contacts in tech mostly say the same thing about their own workplaces. Most of my rationalist friends self-isolated really early, before it was socially acceptable to do so, and their tech company employers kind of rolled their eyes but agreed to let them work from home. I know Google switched to work-from-home only long before the government mandated they do so, and I think the other big companies were also really on top of this.
Hall of shame goes to Triplebyte, which forced its employees to work from the office well into the epidemic, then fired a fifth of them without warning. The rumor is that it had planned the downsizing for a while, wanted the employees to be in the office to hear about it in person, and didn’t care how much risk it had to expose the soon-to-be-ex-employees to in order to make it happen. Not cool, and I’ve cancelled my Triplebyte affiliate link in protest. GameStop is also getting in trouble for staying open and requiring employees to bring their own sanitary wipes. And although Tesla originally got in trouble after Elon Musk dismissed concern as dumb, Musk has since claimed he will repurpose his factories to make ventilators if needed, so I will refrain from criticizing him until I’m sure we don’t all end up owing him our lives.
Short links
Chinese anti-coronavirus propaganda banners. “Visiting friends and relatives is mutual slaughter”, “Everyone you encounter on the street is a wild ghost seeking to take your life.” Thinking of getting a “Those who come visit you are enemies” banner for after the virus dies down, just so people know where I stand on social events.
It’s not a real global disaster until hordes of ravenous wild monkeys terrorize cities.
The current death toll of the coronavirus is negative fifty thousand, although the article is out of date and it may have risen to more like negative forty thousand by now.
In the last coronavirus links post, I suggested that the guidance against wearing masks seemed like more of a Noble Lie intended to prevent hoarding than good science. A Less Wrong post gave more information and expanded the case, and now it’s in The New York Times: Why Telling People They Don’t Need Masks Backfired. And notice the wording! It’s not newsworthy that the government deceived us, it’s newsworthy that the deception didn’t achieve its intended goal.
California governor Gavin Newsom responded to the coronavirus in a very California way: by shutting down all large gatherings of 250 people except Disneyland. A few days later, Disneyland closed anyway.
US: all nonessential public gatherings are banned. France: “More than 3,500 Smurf cosplayers gathered over the weekend in an attempt to break the Guinness World Record for the largest group of people dressed as Smurfs.” Also: “Mayor Patrick Leclerc defended the decision to hold the event, which he said was necessary to alleviate the “ambient gloom” around the country. “We must not stop living. It was the chance to say that we are alive,” he told AFP.
Police departments: criminals should do their part by not committing crimes during the coronavirus epidemic. ISIS: terrorists should avoid Europe for the duration of the epidemic.
More on how the FDA and CDC tried to thwart the Seattle study that finally discovered the coronavirus had been circulating uncaught in the city for weeks. And Pro Publica talks about how, in addition to thwarting more coronavirus tests, the FDA is forcing the CDC to waste its few tests by testing the same people twice.
Related: according to numbers I have not independently confirmed, a single billionaire is providing orders of magnitude more coronavirus tests to the US than the entire federal government so far. It’s a good time to be against against billionaire philanthropy!
Our World In Data has a predictably great piece on the coronavirus, including the opportunity to track how many cases in each country on each different day. Very useful for amateur research!
















So, the countries that appear to be most heavily hit by COVID-19, according to this page, are all in Europe.
If you click on “Total Cases/1 Million Population”, at the top of the list is San Marino, with 5511 cases/million. Going down the list, it’s a bunch of small European countries until we hit the first large one (Italy) at number 8 (1144/million), after which we have a parade of all the major nations of Europe until we hit the first non-European nation (Iran) at number 20 (295 cases/million). The US gets off comparatively lightly at 166/million, with Canada at 74/million, and Brazil at 11/million.
Why is Europe getting hit so hard? Is there more travel between Europe and China than between Europe and the Americas? Is an older population more susceptible to the disease? Or have the Europeans done more testing than other countries, and therefore found more carriers than others have?
(I’m not looking for a snide, “It’s the socialism,” here. If you insist socialism is actually the problem, ok sure, but please explain.)
We have really good reason to doubt the Iranian numbers. Their government lied about the existence of Covid-19 there for weeks, the numbers of Iranians tested outside of Iran suggest the numbers are higher, and Iranian health workers doubt the numbers, too.
We have reasons to doubt the US numbers, since testing has been trailing for weeks, and the poorer people are discuraged to get tested for financial reasons.
I also doubt the numbers in places like Russia, where officaly there are only handful of cases, but they report an unrelated raise of pneumonia deaths by 37% in Februar.
But taking the numbers at face value:
– A lot of travell with China.
– A lot of internal travell (a lot of the cases in Germany come from people that where on Ski Holidays in Italy)
– Bigger population density as the other places you cite.
Part of it is because the country is probably the wrong unit. The US has several major separate outbreaks; it’s not one big outbreak. No matter how you cut it, Italy is an outlier though (San Marino is very small and probably shouldn’t be included).
I’m also happy to blame mass transit (which also explains NYC).
That was my first thought. It can’t be the too much of the reason, though, because the majority of Europe’s population (well, at least the majority of the EU’s population plus a lot of the non-EU European states) are in countries with higher cases / million population than the US, which suggests that the EU or Europe altogether would have more cases / million population than the US.
+1
I’d be somewhat interested in seeing some sort of data that reflects something like “prevalence of travel between Spain and Italy” vs “prevalence of travel between New York and Louisiana” or something like that.
It seems plausible to me that Italy and Germany are more highly connected (and should thus be treated as a single outbreak) than Florida and Washington (state) are…
So I hadn’t been looking at the political questions of what’s taking Congress so long to pass some kind of relief, and it looks like each side is fighting over getting their own pet projects included, and I realize that aside from a few tiny spots of competence (like Dr Fauci) our Federal government has been horrible throughout this.
Economic relief is critical to getting people to comply with social distancing. “Help the community but you’re on your own” is a psychotic message. Anyone training a dog like this would get bit and deserve it.
No one likes seeing the sausage get made but I really didn’t expect them to be stuffing humans into the grinder.
That’s the standard message — like JFKs “Ask not”. It’s just usually those receiving it don’t recognize how “psychotic” it is because they conceive of themselves as the helpers rather than those needing help.
Well, Ontario is shutting down all workplaces of non-essential businesses effective 2020-03-25T00:00:00-04:00, but isn’t announcing what is considered essential until tomorrow. So if you’re maybe-essential, you won’t know for sure until about 12 hours before you’re expected to lock the doors.
The charitable interpretation is that they suddenly realized they’d have to do this, and it’s marginally better to give people 24 of potential + 12 of certain notice than just 12 of certain notice, so announce you’ll have a list ready tomorrow now.
The fact that the LCBO (government operated liquor stores) have already been announced to be essential makes me think the charitable interpretation is a bit too charitable.
Yeah, I noticed that too. The best case I can make for keeping the liquor stores open is that there are some hard-core alcoholics out there, and if we make them go cold turkey for a month, there’s no telling what damage they might do. Uncle Dave really needs his medicine. This would a bad time to have people showing up in the emergency wards from drinking bad home-brew.
Of course, none of this would be an issue if we let grocery stores sell booze. But that’s more a Shelbyville idea.
You would think grocery stores selling booze would solve everything, but here they apparently couldn’t figure out a way to allow you to verify your age in the self-checkout, and now you have to go through a normal checkout if you want to buy it, thus ruining everything. There was a magical period, though, where they were still trying, and consistently you could scan your alcohol, the machine would try to call an employee to card you, and then it would quickly timeout and revert to simply letting you buy it no questions asked. I wasn’t even underage then, but it made me feel young again.
People drinking bad homebrew wouldn’t be the first problem. Cold turkeying alcohol can be bad. Really bad. Having a dozen people with delirium tremens delivered, while your ICU is effectivly an corona ward, might cause a lot of headache for the hospital personell, and a couple of additional deaths.
Oh and making people who are not alcoholics, but like to drink a beer or two on a saturday angry might not help with compliance to the quaratine measures.
Fair, although I doubt the same reasoning applies to the government cannabis stores (also deemed essential).
Thanks for the comparison between the symptoms of COVID-19 vs flu!
Too bad they are the same, though. (Well, except for the shortness of breath.)
Does anybody have access to good line-level data regarding COVID cases, mortality, comorbidity, demographics? I see tons of aggregates, and a few papers citing a relative handful of cases, but I cannot find the sort of data that “20-0251, COVID-19 in Gansu Province, China, 2020, Volume 26, Number 6—June 2020” is based on.
How far have you gotten in this project? Have you tried looking at that paper and seeing where it said it got its data? It says this website. I don’t see a clean database on that website, but I do see press releases like this that lists sex, age, and township for 3 people which is a plausible kind of source for a paper that considers only those attributes and only 54 cases.
Not far. I contacted Dr. Bao and it sounded like he was going to send me the dataset, but communication stopped. I’ll try the other co-authors.
So when should we expect testing and modeling to become good enough that health departments can tell me their estimate of how many people are infected and/or contagious in my county today? Ever?
“Henceforward, musical performances will not be allowed” said Tom, disconcertingly.
Remove the tests per capita link. It is outdated and hasn’t received updates.
Daily deaths in the US were exponential through March 19, then declined 19->20 and 20->21. On March 22, deaths jumped from 46 to 117, an exponent of 2.5 – what’s the deal with that?
Noise.
Failure to report on the weekend.
not perhaps the key point here, but the mayor of San Francisco is called “London Breed”? Sounds like a Rockstar game about aliens invading the UK
I wrote some commentary on Neil Ferguson’s paper and used some more recent data for anyone interested. It’s intereactivish.
https://johnburidancommentary.wordpress.com/2020/03/23/de-imperial-colleges-npi-paper-led-by-neil-ferguson/
Okay, so if the shelter-in-place is working for the Bay Area, we should be starting to see its effects in new cases at this point and over the next few days — that is, the shelter-in-place has been in effect longer than the typical incubation period of the disease.
Confounding our ability to assess its efficacy, we’re probably (?) testing more vigorously now. Is anyone aware of anyone trying to gauge the success of the shelter-in-place, for either the bay area or California as a whole?
It took 12 days for the lockdown in Hubei to show up in the official data. Haven’t you seen this graph from this paper? (originally this graph from this paper)
Lots of differences between California and Hubei. Do you have any particular reason to believe it actually takes twelve days to take effect, or that if the real effect is sooner but it shows up in the data later, that whatever effect causes that is the same in California and Hubei?
Two random ideas:
1) On the herd immunity thing: ISTM that there are going to be an awful lot of enterprises that will pay a premium for covid-immune workers in the not-too-distant future. If there were a way to formalize this premium, I wonder if running “covid camps”, where young workers could voluntarily be paid a nominal sum to take the risk to get infected, spend 6-10 weeks getting sick and recovering, and then receiving a government certification of immunity, which would command a nice wage out in the real world, would make sense. There are obvious logistical and security problems setting up these kinds of camps at scale, but it seems to be a) a pretty good way to feed immune people back into the herd and b) an interesting way to stimulate the economy.
It also might be an interesting way of doing early-phase drug and vaccine trials at scale. You might also discover that you could converge on an inoculation strategy, where you infect people with the weakest strain of SARS-CoV-2 that confers immunity.
2) I’m a CPAP user. There are an awful lot of CPAP users out there. I’ve been wondering if it would be a good strategy to figure out how to turn home CPAP machines into extremely cheesy ventilators. Adaptors to accommodate O2 are easy to come by, and I assume that the production of oxygen bottles and regulators would be something that would be very easy to ramp up, as would the supply of full-face CPAP masks. Some questions:
a) You’re obviously not going to get anywhere near the max inspiratory pressure out of a home CPAP than you are out of a vent, and there’s very little expiratory help from your garden-variety APAP machine. But it’s quite a bit better than nothing, especially if you’re out of hospital beds. Does anybody know a reason why this would be a bad thing to do?
b) Assuming that you’re becoming your own do-it-yourself respiratory therapist, is it possible to create guidelines for O2 flow that would let people use home pulse-oximetry to keep from poisoning themselves? ISTM that it’s pretty easy to increase flow if SpO2 drops, but it’s harder to tell when you’re over-saturating people. Any ideas?
c) Any thoughts on what the max safe pressure is on a home CPAP machine? My guess is that you start having seal problems long before you’d get to the point where you could over-pressurize somebody’s airway, but IANART.
d) This would be a useful supplement for staging people into the hospital system, but it likely means that you’d have a lot more admissions that would have to go straight onto vents. You’d have to have some way to convincing home users that they’d get triaged fairly with the inpatients that were being considered for transition from mask O2 to vents. Still, unloading the non-vent population of covid patients seems like an unambiguously good thing.
Both of these may easily be stupid ideas, but I’d be interested in hearing what you all thought.
CPAP is better than nothing you’re right.
Here’s the issue in current treatment for COIVD19 with NIV (non-invasive ala CPAP/BIPAP) – normally we would use these as a mid-range step from simple hudson mask/nasal prongs to intubation in a viral pneumonia. However the data coming out of China and Italy suggests that if you’re severe enough to require more support than 6-8l of O2 then you will end up requiring intubation.
As such, most hospital groups and professional societies in Australia have said CPAP/BIPAP is contraindicated in COVID19. Because we know, based on current information, you’ll need tubing anyway, and NIV will aerosolise the virus increasing risk to anyone taking care of you.
If you’re able to stay home and you’re non-severe then yeah a bit of PEEP might help but a lot of the ventilatory stragies we use for severe patients require a bit more control than that. Barotrauma is absolutely a thing in ARDS, although lung compliance seems to be less of an issue with COVID19. This is where my knowledge starts to top out with respect to ventilation.
To answer you’re overall question there may be a role later on if we can accurately triage who is going to just need O2 and who will need intubation (currently difficult), at home O2 may be useful. Our guidelines are keep sats in non-COPD at 92-94%, no higher.
Thanks, that’s very helpful. Not super-reassuring, but helpful. “Not super-reassuring” seems like it’s the best-case tagline for 2020.
Gov. Cuomo says its too late for less than 40-80% of New Yorkers to get COVID-19, government measures are just to “flatten the curve” for hospitals.
“You’re losing your job, and your civil rights, and you’ll still get the virus at some point.” 🙁
Nice dog.
I agree, it is a nice dog.
I am (a non-expert who is) researching the mechanism for SARS-Cov-2 replication in a human host. I am considering the idea of disrupting this mechanism by infecting a host with a known alternate which has milder effects (e.g. does not cause a response like filling lungs with fluid) but uses the same cells for reproduction that SARS-Cov-2 would use, in the hope of slowing the infection rate.
Does anyone here have suggestions of where to look for data that suggest which cells are targeted by this novel coronavirus? Also, “getting sick to get better” may be a crazy idea. Is it a bad idea as well (what could go wrong with such an attempt at disruption/co-option)?
FWIW, here’s a pretty nice summary of some of the strategies being looked at, including an explanation of why chloroquine might work.
One virus using a set of cells to replicate does not preclude another virus doing so (unless you largely wipe out a population, which is super problematic in lung). Don’t think this idea has much merit tbh.
“SHOULD I CONTINUE TO PRODUCE SODA, MR. PRESIDENT? SHOULD I?”
Has anyone modeled what would happen if the government took minimal containment measures and the virus actually didn’t provide sufficiently long-lasting immunity (thus keeping herd immunity from working)? All of the graphs I’ve seen for minimal containment measures show one giant spike in deaths that quickly falls back down, but I wonder what that graph would look like without the assumption of herd immunity. Would the entire population eventually get the virus, perhaps multiple times, until a vaccine is discovered? This sounds like it would cause massive amounts of deaths and permanent organ damage, so just a small chance of this scenario playing out might be enough to offset the potential economic damage caused by strict government containment measures.
If having it doesn’t lead to at least moderate term (years) immunity, I’d expect a vaccine to be impossible. In that case, the ultimate survivors will be those few with natural resistance, unless we manage to eliminate the virus entirely – and that latter task would be next to impossible. Welcome to the “after the collapse” novel or movie of your choice.
For those creating plots for novels and movies, there are other options. Gene therapy might transfer that resistance to others. But perhaps at the cost of making them more like the naturally-resistant animals the genes came from. (You don’t get C-19, but you start to sprout feathers ;-() Actually, this could be quite a fun plot, especially if multiple species provided resistance genes, and we got bird-people and bear-people and …. an ever shrinking handful of normal human survivors, who e.g. generally die before they are 40, from the cumulative effects of multiple courses of this plague…
If you can get temporary immunity lasting months, could there be a vaccine that people take every few months?
Here’s Yaneer Bar-Yam calling for a five-week lockdown to contain the virus:
Spain and France are on track to turn into Italy, with hospitals “overwhelmed.”
Will it be news when they do?
Is anyone tracking this?
What are objective measures of whether a hospital is “overwhelmed”? The first thing that happens is that they run out of ICUs/ventilators and have to triage. I have read that this has happened in Seattle and Madrid. After(?) that they have to triage regular beds. Then they run out space for patients yet to be admitted and use triage tents outside the hospital. Another metric is how many hours the staff work.
These are not directly comparable across countries, because they depend on the number of beds available in the first place. But they may be the best measure if you don’t trust the death counts.
I haven’t heard that has happened in Seattle. I’ve heard dire prophecies that it soon will happen, and I’ve heard that hospitals are writing policies and plans for when it will.
I probably misread that article. I was surprised that it didn’t get more coverage, but maybe that’s because it hadn’t happened.
I thought this was a good example of a Coronavirus backlash article by the young and healthy: https://bpodgursky.com/2020/03/22/you-should-be-angry/
The general idea is that the current US approach provides a small benefit for the elderly at tremendous cost to the young: “The young — the ones who will pay for, and live through, the recession we have wrought by fiat — do not even benefit from the harsh medicine we are swallowing. But they will taste it for decades.”
His suggested solution is that we follow the example of some Asian countries, prioritizing keeping the economy alive, trying to minimize the spread of the disease while accepting that there will be an increased death rate among the elderly: “The solution to this crisis is simple — we do our best to emulate East Asia. We isolate the sick. We improve sanitization, and we mobilize industry to build tests, ventilators, and respirators. And we do this all without shutting down the economy, the engine which pays for our future.”
Regardless of whether this is the best approach, I think this is a theme we’ll be hearing a lot of in the coming months. How do you think this movement develops?
I don’t think there will be any movement as such. Easy enough to write a contrarian article, but no politician is ever going to get behind “let the old people drop dead, because it increases total utils.” The UK floated something much milder and it collapsed within days.
This:
on the other hand, has a chance of happening if we get our act together.
I don’t think so; I think New York let it go too long. And I’m suspecting Deblasio of a coverup, too.
It’s only possible if we get the current explosion under control with the full-on shutdown. Then if we had adequate tests and masks we could gradually loosen restrictions on people that test negative twice a week apart or something like that.
That said, given what I’m hearing about zoomers, parents, and haradim I don’t expect such a getting under control any time soon.
Perhaps we can get most places back in control with testing and contact tracing, but NYC has to suffer for an extra 6 months.
Someone joked(?) about West Virginia closing their borders. But states cannot close their borders. Maybe we’ll see some state try it to keep out the NYC infection.
States posses enormous power under circumstances like these dating back English common law. Since we haven’t had a pandemic since before the modern Supreme Court era started these precedents have never been overturned.
I suspect “hearing” will be the end of it, since the young getting mad about being screwed for the benefit of the older and wealthier has failed to accomplish anything for awhile now (unless I’m overlooking something serious). If things get sour enough for people to get angry enough to to actually accomplish something in this regard, I’d be interested to see what happens, but I suspect there will be nothing but whimpering.
My guess is that the tide will turn once we start seeing layoffs in the white-collar, work-at-home sectors.
Right now, most of the white-collar younger people I know think that this won’t affect them because they can just work from home and order doordash or whatever. And these are people who never bothered getting mad about social security or whatever, because to them the payroll tax is just a fact of life and they have company-match 401Ks anyway.
Once the true effects of economic shutdown “trickle up” to the big corporations and we start seeing massive layoffs of white-collar types, the popular social media narrative will change dramatically.
The boomers can win a political battle against the young poor, but they might not win it against the young poor AND young middle/rich…
If the boomers are significantly weakened by the virus, maybe this problem will just solve itself. (Sarcasm)
Seriously, though, the amount of disdain for the old and wealthy among the young is extreme, I think. Among many people I know, you won’t get reprimanded for actively hoping that the virus kills the elderly. I figure, though, that while many big money-havers are older people, most old folks are not oligarchs, so that might be a bit extreme.
Young people will matter right after the election when they start voting. That’s eight months away at soonest.
Young people voted in underwhelming numbers in the last election, but are confidently predicted to be motivated by mumble-something to vote in great numbers in the next election.
This is approximately as much a universal constant as death, taxes, and fusion power being twenty years away.
Agreed that voting won’t do much: Young people barely see the point anymore. Hard to blame them.
Maybe when everyone under 40 is tired of wandering the streets eating gravel because participation in the economy is impossible for them, maybe they’ll get angry enough for a violent revolt. Unless cheap french fries and the internet keep everyone complacent while society crumbles around them. Kind of feels like that’s what’s already been happening for awhile. My anecdotal impression is that young adults (which I was recently one of) are thoroughly fatalistic and are pretty much ready to let society die as long as they can be entertained during the ride.
If the slacktavists of the insta generation can’t be bothered to vote, they certainly aren’t going to put together an actual revolution. The memes will be fierce though.
I searched the post for the word lung, didn’t find it, then closed the post. I really don’t want a bad case of this disease. If 1/5 young people who get it end up in hospital, and any significant percentage of those have permanently reduced lung function, that’s a much more significant impact and story going forwards than a bunch of old people actually dying. You’re looking at an entire cohort of permanently crippled people across all demographics, who from the sound of things may not really be able to hold down any kind of job at all, ever. And if those people can’t get treatment during a peak of infections, the odds just get worse. Would you roll a six-sided die knowing that if a one turns up your life is effectively over? Anyway, I’ll eat my words if this doesn’t start to be a story in places like Italy, but I think it’s a failure to properly grapple with the consequences of this if you’re only looking at death rates.
You’ll hear about young people with lung damage, but that doesn’t mean it was permanent. SARS didn’t cause permanent lung damage, but it took a year to recover. Obviously, we can’t wait a year to find out.
Here is a paper with 9 month follow-up on a small sample of SARS survivors. Here is a larger sample, but only at 6 months when there was still substantial damage. I thought I saw a paper on 1 year follow-up, but I’ve lost it.
It was too late for the US to emulate the South Korea/Singapore approach 2 weeks ago.
Shutdown/Mitigation/Whatever gives you time to hopefully get to a point where you might be able to emulate that approach without completely overwhelming the hospital system, as the East Asia approach is probably going to be the endgame for everyone.
The cynic might note thats hardly a surprise. Building new houses, or boomers dying, has the exact same effect on their precious rent seeking trade.
More news on COVID danger by age.
~37.6% of Americans are 18-44. 22.4% are under 18.
If 165 million Americans caught the kung flu, up to 12.4(-1.24 to 2.48) million adults under 45 and 4.13 million children would need to be admitted to normal hospital wards and field hospitals without ICU beds and the adults would require 1.24-2.48 million ICU beds.
However! This doesn’t count the fact that testing is so bad that 19 undiagnosed carriers per known case is a fairly conservative estimate. While it would be grossly negligent to take action based on such an X factor, that number being true would mean the young (0-44) require a total of 764,500 normal hospital beds and >124,000 ICU beds.
I can’t find data on how average ICU stay length for the infection varies by age.
Does a stay in a normal hospital ward actually help anything?
I’ve read lots of articles suggesting a secondary economic fallout from inadequate state resources to handle skyrocketing unemployment claims. Simultaneously, it seems there are massive supply chain problems in grocery stores, medical equipment production and distribution, healthcare workers, etc. Could state and local governments not coordinate putting the massive force of recently-unemployed workers to work on these supply chain problems? It seems to me that this would pit the two crises against one another.
I don’t know exactly how difficult the logistics are, but I imagine the on-boarding for temp grocery store work / supply chain work would be really fast. Further, the companies experiencing overwhelming demand could themselves pay this temp workforce, removing the financial burden on the state, no? Maybe I’m missing the limiting factors here (geography differences between hospitality vs. supply chain, or something else).
Healthcare is a different animal since there’s certification/liability problems in addition to healthcare being skilled work. But is there not an enormous amount of legwork that could be done by a massive influx of unskilled workers (coordination / setup / moving things / disinfecting / non-medical work)? How long would it take to give otherwise unskilled workers training equivalent to say, army medic? This also comes with the risk of increasing infection rates, so I’m not as sold here.
Lastly, it seems that since hotel and cruise industries are about to be decimated by the lack of business for 6+ months, why not convert these places into makeshift hospitals / isolation areas for the moderately sick? I imagine most large cities in the US are port cities that could dock cruise ships. Maybe the resources required are too many, but it seems like NYC in particular is starved for beds, and these places just happen to have isolated beds set up for short-term living!
Actually it’s worse than that: these industries could have business reduced by 100%!
More difficult than government bureaucrats can handle, that’s for sure.
If they handed the keys to the money printer directly to Jeff Bezos and the Waltons, they might be able to figure it out though…
I’ve heard that the army is already doing this in NY and DC with hotels and sports stadiums…
+1
I (in NY) have been more nervous about what decree will come down next than I have been about the virus.
This Wired article reflect fears I have. This suggests a permanently locked down society, where the government lets people go out in accordance with hospital capacity. The fact that no one seems to be questioning the powers the government has been assuming or worrying much about the long term economic consequences scares me considerably more then the virus (granted I’m no in a high risk group)
https://www.technologyreview.com/s/615370/coronavirus-pandemic-social-distancing-18-months/?fbclid=IwAR1o-id92xjXeiOmmoLJqAjrW0kMwCrMhRgm4rSCtF0nJuNerriC0rAmsjo
“We will have to live in a totalitarian police state where the police have powers undreamed of by 20th century regimes. Let’s hope we’ll all be equals under the totalitarian police state!”
Arghdeblargh I don’t even…
Does anyone how valid the information in this article is? https://www.faz.net/aktuell/gesellschaft/gesundheit/coronavirus/neue-corona-symptome-entdeckt-virologe-hendrik-streeck-zum-virus-16681450.html
“Almost all infected people we interviewed, and this applies to a good two thirds, described a loss of smell and taste lasting several days”
More on this: https://www.forbes.com/sites/judystone/2020/03/20/theres-an-unexpected-loss-of-smell-and-taste-in-coronavirus-patients/
There’s a bunch of anecdotal reports on this around from patients with Covid-19. Here’s one (this is a friend of a friend; she’s a US chess grandmaster and a US Women’s Chess Champion): https://www.facebook.com/irina.krush.3/posts/2534377286892603
I’d contend that’s not unexpected in an infection that initially manifests as a respiratory tract infection. It’s pretty common to the extent it’d be bloody useless even as part of a screening tool.
Counterpoint: I’ve had this exact symptom and heard of others having it. In my case I never had any loss of my sense of taste or smell before, I don’t have a blocked nose and the effect is drastic: vinegar smells and tastes indistinguishable from water. I have not been able to get tested and my symptoms are mild otherwise (headaches, no fever only little coughing).
I’m reasonably convinced it’s a symptom of the disease in my case (90%) and if so it is drastic enough that it should have diagnostic value.
It seems like the “contrarian” articles saying “let’s maybe take a more targeted approach that doesn’t cause such widespread economic damage” have gotten more numerous and prominent in the past few days, e.g.
https://www.nytimes.com/2020/03/20/opinion/coronavirus-pandemic-social-distancing.html?action=click&module=Opinion&pgtype=Homepage
https://medium.com/six-four-six-nine/evidence-over-hysteria-covid-19-1b767def5894
Not saying they’re right, and maybe this is just an inevitable backlash against the pain of the more severe CA/NY type measures; but more evidence that it’s a point of view worth taking seriously.
I guess that officially makes COVID19 culture-war material now?
It was archived. I’m not sure if that makes it culture war, but there is a significant overlap between culture warriors and people who say “trust our experts and don’t think for yourself”.
Most of the article is basing things on increase in confirmed cases, so I think it actually is nonsense (since increase in confirmed cases in many places are heavily dependent on testing, giving almost no signal on disease progression). But I didn’t think being wrong was against the rules.
I think the new response is just particularly infuriating to people who were inquisitive about the situation in January and got tut-tutted at. I’m in IL and we are basically in lockdown as well, and there is really no end in sight. 100% of “nonessential” cut off for 2 weeks, and then what? C19 is still going to be out there in numbers high enough to jump right back into exponential stage in 2 weeks, 4 weeks, and 8 weeks most likely.
The only way the current plan works is if somehow secretly like 30% of the population already has asymptomatic C19, they spread it to their families in quarantine, and in 2 weeks almost everyone 0-45 is immune. That seems unlikely.
A somewhat amusing take –
Flatten the Curve of Armchair Epidemiology
Hope this doesn’t apply to anyone here 😉
It appears to be a contentless sneer.
Has anyone released any statistics regarding the socioeconomic background of cases?
Anecdotally, we’ve all heard about particular clusters… most of them that involve athletes, movie stars, frequent international travelers, ski resort hoppers, etc.
Even the “I’m just a normal person but I caught the virus!” takes getting passed around the last few days seem to be college educated white collar aspiring-elites who caught it at a tech conference (or AIPAC!!!) or something.
I haven’t heard much of “I’m a grocery bagger and I caught it.” Of course, that could be because grocery baggers don’t think to write thinkpieces for the Atlantic. Or because nobody is allowing them to be tested. Or for many other reasons.
But for as much data as we’ve seen on cases and fatalities sliced by age and co-morbidities, I don’t think I’ve seen a single one that mentions SES. At this point I’d even settle for “% of cases above and below national median income”
I’d expect it to be rich people who caught it first in the US, because rich people do the most international travel. But NYC has quite a few public transit workers who have it.
I agree.
Where are all the infected international airport workers. I fly back and forth from the midwest to China regularly and there are all ages, from young to very old.
Grocery store workers in every city and seeing the whole population. Yet not getting sick in any large numbers. Maybe because they arent over 70 with serious health problems?
Perhaps most infections are passed through more substantial interactions than what grocery store workers have with customers.
And I’m not at all confident that we have an accurate idea yet of what the infection rates are for grocery store workers.
I’m also hearing an increasing amount of anecdotal social media accounts of “I was pretty sick 2-3 weeks ago with much of the COVID symptoms, but not enough to keep me from going to work, and it never occurred to me to go to the hospital and demand a bunch of tests or anything.”
Is it possible that this disease has already passed through much of the blue-collar population and they just shrugged it off because it manifested as similar to the flu?
Seems unlikely. As the diagram above shows, the symptoms of COVID-19 are a lot like a cold or flu. But colds are common and COVID-19 is rare, so people with those symptoms probably did in fact have colds.
Except that the rarity of it may be spurious, an artifact of how people didn’t get tested.
Roughly 2.3% of people who contract COVID-19 die. In an ordinary year roughly 0.8% of Americans die. If a hefty part of the population got infected and suffered the consequences, the aggregate death rate would have doubled. Maybe more, maybe less, but something on that order. That would have been noticed. Death statistics are closely tracked.
I suppose a smallish, isolated population could mistake a COVID-19 wave for a bad flu season, particularly if they skew young. But in a large multi-generational population there would be a very noticeable spike in deaths, and before that of demand for ICU care. So I don’t buy this scenario for the general population.
https://www.cebm.net/global-covid-19-case-fatality-rates/
https://www.macrotrends.net/countries/USA/united-states/death-rate
johan_larson,
That 2.3% cited is case fatality rate, not infection fatality rate. CFR is only reported cases in the denominator. IFR will be much lower than 2.3%.
Additional follow-up question: Who is the richest/most famous person to have died (or even had to be admitted to ICU/placed on a ventilator) from this illness?
We keep hearing so many cases of famous athletes, actors, and politicians having this. But as far as I can tell, they’re all asymptomatic and all appear to be fine.
Where are the contrarian arguments based on simple math?
In early December a Wuhan doctor tried to leak that there was an increase in pneumonia cases. Wuhan has an international airport with direct flights to SF and NYC, among other places.
At the same time, Covid19 is so virulent you cant even be near other people, because it spreads all over the place. I read a story about a Biogen meeting in Massachusetts where one person supposedly infected 90 other people, or that is the guess.
Where are the millions of infected that equation spells out. And the deaths. This has been spreading since at least early December, out of China, on full international flights, through airports. 5 months!
LA has a homeless population of 100,000 living in tents, some shooting heroin, socializing all day. Wouldn’t the virus infect all of this group? Shouldnt the LA hospitals be full of dying heroin/crack addicts who have the double whammy of this infection plus coming off of heroin?
None of these ideas work together. The supermarkets have people who are somehow immune to the last 4-5 months of spread, speaking to people everyday. Where are all the infected international airport workers? Shouldnt they be in the front line of hundreds of thousands of infected?
The Philippines first case was early February. If have ever been to Manila you understand that the idea this is a super spreading virus that kills, does not make any sense.
You’re telling us your equation spells out millions of deaths, but unless I missed it, you didn’t present us with an equation.
But let’s just say, for the sake of running a little simple math, that the number of people with the virus tends to double every week, left to its own devices. So our equation is
number of infected = 2 ^ (weeks since first human case)
Let’s say the first human case of this virus happened around 22 weeks ago, and that the virus doubles its number of infected people every week. That yields about four million infections by now. I wouldn’t say the picture we’re seeing so far is wildly inconsistent with the idea that this thing doubles about weekly.
It’s only if you think the virus doubles much more than about once a week that you start having to wonder about where all the “missing cases” are.
Thanks for replying.
Its hard to make an equation. And I didnt say millions of deaths, but there should be tens of millions of infections, so many that is is obvious there is an epidemic. Its the opposite. Essentially there is no epidemic except for some rare cases of people in the hospital. 200 deaths in the USA? Thats less than a rounding error.
But the idea that this spreads incredibly easily and has been spreading since early December on international flights and international airports to all the major cities in the world, and after 4-5 months this is it, does not compute.
One infected person coughing on a Shanghai subway car should infect hundreds. Repeat. Tokyo. London. Seoul.
Sydney Mardi Gra was in mid-February and had up to 500,000 people there, dancing, drinking. Its a pretty wild LGBT event, shoulder to shoulder. The parade has 10,000 people alone. Where are the infected? 1.7 million Chinese students in Australia. There is a huge flow back and forth.
If the government of all these countries says when you cough the droplets go into the air and everyone around you get sick, plus it stays on objects like tables, chairs, door handles, mass transit for up to 3 days. So for 22 weeks it spread, where are these infected?
Direct flights from Wuhan into SF and NYC. Starting early December.
Its hard to make a simple equation for that, but there should be infected everywhere and we dont see that. Or 95% of people infected dont get any symptoms at all and its the weakest flu virus ever, except for the people it kills.
You’re right. I did slip up there, saying “deaths” instead of “infections”.
I think your last comment shows the source of your problem. You say,
“One infected person coughing on a Shanghai subway car should infect hundreds. Repeat. Tokyo. London. Seoul.”
I don’t think anybody is seriously claiming that one person coughing on a subway car would infect hundreds. That would assume an R0 way out of line with any infection disease I’ve ever heard of.
What the actual public health folks are saying is that they estimate that, without mitigation of any kind, one person will on average infect two or three others.
I don’t think anyone serious is claiming that one person automatically coughing on a subway car will automatically infect everyone. That’s just not how real-world infections work.
I suspect we’ll find the major correlate of spread turns out to be mass transit (full disclosure: I hate mass transit). And there’s probably something to climate inhibiting spread, which would explain the Phillippines.
Right now the vast majority of people dying are very old plus serious health issues like being a cancer survivor, heart disease, obese with diabetes.
There is probably some other very odd co-factor to go along with that. Otherwise how can Italy have a large number of deaths and Germany have a couple dozen.
What on Earth is wrong with New York?
Airports are still operating!
“Non-essential” businesses will have to close except for work-from-home white collar work, but:
Hey, I have a better idea: make people bank online and use ATMs, prevent children from being daycare-enabled asymptomatic super-spreaders, shut down the airports, and post police on the highways so no one enters or leaves the NY/NJ/CT commuting area except new health care workers?
Where is the evidence that children are asymptomatic super spreaders?
I agree. I have seen the opposite. That there has not been one verified case of a child becoming ill and spreading it to an adult. Not one.
How would such a case be verified, when AFIK nobody is testing children?
Children are superspreaders of pretty much everything else that looks like a coronavirus, so our prior should be high that they are superspreaders of this particular coronavirus. And, absent testing of children, “not one verified case…” gives us zero information to update that prior.
With potentially millions of lives at stake, I’m going to go with shutting down the schools for at least a few weeks to see what happens. OK, from a libertarian perspective, shutting down the state-run schools and asking the private (US sense) ones whether they want to serve as a natural experiment.
Weren’t children tested extensively as part of contact tracing in China and elsewhere? There are lots of documented cases of children being infected by their parents, but none of parents infected by their children.
Yeah, how about not. I don’t want to be shot just because I tried to leave the area to find food. (Governments prioritize sympathetic people for assistance; I’m on my own, so if the prioritized have cleaned the grocery stores out, it’s either catch squirrels with my bare hands or starve. And those little bastards are fast)
What state do you expect having to drive to to not starve?
West Virginia, maybe, since the NY/NJ/PA/CT/DE governors are all in concert, and taking orders from Cuomo.
Of course since WV has the least number of cases, they might just close their own borders.
I googled this and found a city government website that gives the rationale
https://www1.nyc.gov/site/doh/providers/health-topics/novel-respiratory-viruses.page
I guess it kind of makes sense. There are too many cases to do contact tracing on all the positive tests. So a positive test doesn’t matter, you’ll just end up telling them to isolate themselves, which they should do anyway.
The “discouraged hospitals from testing asymptomatic health care workers” sounds weirder, but if there really is a “critical shortage of collection swabs and viral transport media supplies” then I guess you have to ration the testing materials and you might want to stop testing asymptomatic people.
Maybe they should, but there’s a good chance that they won’t. If all you’ve got is “you have a cough and a fever; that could be more than just the flu, go isolate yourself for two weeks”, that may not be the most compelling argument to someone who e.g. knows his boss is going to lay off half the workforce next week and thinks being at his desk might make the difference. “You have a cough and a fever and a positive test for COVID-19”, is a more compelling argument.
That’s particularly the case for people who are asking for tests. People who are at the margin for e.g. “should I go to work and risk infecting my colleagues, or stay home and risk losing my job”, are more likely to ask for a test than people who have already made up their mind one way or another.
Nurses and doctors have children. Do you want them roaming the street while their parents work?
Not particularly, but what on Earth is the point of closing schools if the children are going to be in groups of 50+ anyway instead of “shelter in place” like their parents?
We could probably use new temporary daycare requirements.
Like, keep children in smaller, fixed groups throughout the week. If 1 or 2 kids drop out, no merging groups.
It increases the labor requirements a lot. But, y’know, at the moment we have quite a bit of available labor.
In fact the regulations for SF at least specify that group childcare is excepted only if it satisfies restrictions like this– IIRC it’s something like <= 12 kids and same kids with same staff week-to-week.
How do you expect healthcare workers to function if noone is looking after their kids?
Uh oh.
This was posted in here, talking about how the virus survives for 1 hour on cardboard:
https://github.com/matthewravery/casual-inference/blob/master/content/post/data/Lin%20COVID-19%20SARS-CoV-2%20slidedeck%2020200315.pdf
I looked at the original paper (which I should have done earlier) and it looks like the colors are reverserd
https://www.medrxiv.org/content/10.1101/2020.03.09.20033217v2
So the old virus lives for 1 hour on cardboard. This one lives for 24 hours on cardboard.
Am I misreading things?
There is an update where he corrected that
https://drive.google.com/file/d/1ZaiDO87me4puBte-8VytcSRtpQ3PVpkK/view
@ matthewravery, you might want to update your git.
Anecdata:
Relatives in Boston complain they “can’t get tests” but I’m not sure what that means (reported second-hand through parents).
Parents’ neighbor has flu-like symptoms. Possibly coronavirus but doesn’t seem to want to get tested.
Niece’s test was, as predicted, negative.
My father is a doctor at a VA hospital in SoCal and says (as of last week) he can’t get tests to test his patients who he thinks have it.
I don’t buy that actual cases are only 20xs what has been reported. But if that number can be trusted, then all eyes should be on New York.
There have been 11,178 confirmed cases in New York and 56 deaths out of a population of 8.6 million as of 3/21/2020. In the rest of the country there have been 11,530 confirmed cases and 223 deaths out of a remaining population of about 318 million.
That means that in New York, if the actual cases are 20xs as large, 1 out of every 37 people has the virus.
And in the rest of the US, if actual cases are 20xs as large, 1 out of every 1418 people has the virus.
With the moderate quarantine measures that are in place throughout the country (including New York), it is hard to imagine an illness that is only hitting one out ever 1400 people really becoming a huge problem. It should mostly die down in a few weeks.
But with moderate quarantine measures in place it is very easy to imagine an illness that hits one out of every 37 people still finding a way to grow exponentially.
Odds are there is a lot of noise in this data. In New York the confirmed cases to deaths is about 200 cases for every death, while the rest of the country is at 50 cases for every death. This is most easily explained by cases spreading quickly in New York over just the last few weeks, and also by New York just testing better than other places.
But if cases statistics can be somewhat trusted, then New York is greatest danger to the US as a whole at this time. Everything hinges on if they can be contained.
(although I don’t think case statistics can be trusted, not even within a 20×1 window probably. We’ll see how this shakes out/ what comes next)
New York is testing much more heavily than other areas, AFAIK. They’re probably closer to 5X than 20X.
That’s a case count for New York State (19.4 million people), not just New York City (8.4 million).
NY is the U.S.’s Wuhan… is anyone doing anything about it?
Misread as USS Wuhan. Perhaps an appropriate name if for some reason we want to make people think the Navy is ready to engage in biological warfare?
This is from https://www.worldometers.info/coronavirus/country/italy/
March 20 (GMT)
Italy: in the city of Bergamo, there were 108 more deaths in the first 15 days of March this year compared to 2019 (164 deaths in 2020 vs. 56 deaths in 2019) according to the mayor of the city Giorgio Gori. During this period, 31 deaths were attributed to the coronavirus (less than 30% of the additional deaths this year)
“There are significant numbers of people who have died but whose death hasn’t been attributed to the coronavirus because they died at home or in a nursing home and so they weren’t swabbed,” said the mayor [source]
I would recommend not to take an NSAID or tylenol either. See this Atlantic article:
https://www.theatlantic.com/health/archive/2020/03/coronavirus-fever-ibuprofen/608233/
The evidence that lowering a fever by NSAID or tylenol is actually bad for you seems compelling to me, and makes logical sense. It’s reasonable that what’s true for the flu (fighting the fever is bad) would be true for Covid-19. Therefore I think the safest recommendation would be to use neither.
Is there any illness in which reducing the fever helps disease progression? It has always been just for comfort, right? When I was young I had a sustained (>one week) fever of 105+ and didn’t want to take the fever reducer and the doctor said it was fine, fever reducers don’t make you better any faster.
My non-medical-person understanding is that beyond a certain level, the fever itself can damage/kill you, and medical people try hard to reduce it – but by that point the person should be in hospital anyway. For “home sick in bed” situations, the fever probably helps, and some home remedies even encourage it.
But this is just random factoids, not backed with solid data.
My fever peaked at 107-108 and I’ve never heard of a fever higher than that, which is why I doubt it. It does seem like at some point there should be a problem but maybe there’s no biological way to get your temperature up that high.
My son had a fever of like 104 and the nurse was trying to force Motrin on him and I asked what the big deal was, she said he could have a febrile seizure. Well, as far as I know febrile seizures are harmless and are not a result of high fevers per se but of really rapid increases in temperature. But anyway, you will see healthcare professionals push to bring the fever down but when you push back they have a hard time explaining it.
The one thing I could see is that you don’t feel much like eating or drinking with a high fever. So if you have a young child who won’t drink anything, it may make sense to bring the fever down so they drink fluids rather than having to get an IV.
I don’t know about coronavirus, but the flu lasts about as long with or without fever, so I’d much rather spend that time less feverish. Plus, lowering the fever a bit probably helps with the sleep as well.
I wanted to ask if anyone with expertise in graph theory and epidemiological modeling has any thoughts on this approach I’m proposing:
> To a first approximation, the single most important problem to overcome for containment is the exponential growth of the early stages of an outbreak. Of course in some cases an exponential growth is not itself the problem: and R0 = 1.001 leads to exponential growth, but it is still so slow that it can be easily dealt with. Likewise, a sub-exponential growth can still be unruly, as in a polynomial growth with an exponent of 20. But to a first approximation, I would argue that if you can get rid of exponential growth you can manage an outbreak. The example above of a Ringworld shows that exponential growth in contact networks can be slowed all the way down to linear growth at relatively early stages. Similarly, “thin” toroidal planets would also enable easy containment of outbreaks (Anders Sandberg‘s amazing work on the physics of toroidal planets finally pays off! It remains to be seen when his work on stacking high-dimensional polytopes finds real-world applications).
…
Summary:
Remove nodes with a high “Pandemic Klout Score”
Creating sub-exponential chokepoints:
Option 1: Gradient descent methods:
You make piece-meal modifications to the contact network one connection at a time in order to improve the prospects of the entire network.
Each person would receive a set of options for mild modifications to their contacts so that whichever they chose would lead to an improvement of the network geometry.
Option 2: Network nucleation:
You create a criteria for what constitutes “infection-free” such as:
Self-enforced quarantine on one extreme, and
Provable DNA-matched tests on the other extreme.
Allow people who qualify to meet each other.
Everyone submits a list of people they’d like to hang out with.
The algorithm would optimize the connections to make everyone happy and at the same time maximize the sub-exponential chokepoints of the network (such as by making it a planar graph with a high clustering coefficient, etc.).
https://qualiacomputing.com/2020/03/20/qc-coronavirus-edition-preventing-pandemics-by-living-on-toroidal-planets-and-other-cocktail-napkin-ideas/
Neither the LessWrong post nor the NYTimes editorial show that masks are useful for the general public. The only evidence the LessWrong post gives is this paper, which is entitled “Protecting healthcare workers from pandemic influenza: N95 or surgical masks?”. Nobody has ever argued that masks are not useful for healthcare workers, so this is a red herring.
The NYTimes article is written by “a professor of information science who specializes in the social effects of technology”, aka not a physician or epidemiologist. The first argument she uses is inane:
Pilots can use a plane as a means of transportation. I can’t, because I don’t know how to fly one. Yes, I can learn how to fly one, but that requires so much time and effort that I’m unlikely to try, and even less likely to succeed. If I get a plane and attempt to fly it without professional training, I’ll likely hurt myself and make negative progress in transporting myself from A to B. In the case of masks, I’m confident that a trained and disciplined professional would know how to find a N95 mask that fits properly. I’m sure that she would take care not to touch the outside of the mask, not to reach under the mask to scratch her face, not to take it off to talk to someone, and not to reuse the mask. I’m 0% confident that the average Jane can exercise the same good medical judgment and discipline.
The NYTimes author’s second piece of evidence in favor of mask wearing is that lots of people are recommending it, and lots of people–including WHO officials–are doing it. Needless to say, that’s hardly decisive proof that it works.
The only somewhat relevant paper she links to is this one, which concludes “Hand hygiene and facemasks seemed to prevent household transmission of influenza virus when implemented within 36 hours of index patient symptom onset.” As far as I know, the CDC didn’t say you shouldn’t wear a mask if someone in your household has COVID-19, so this paper isn’t strictly applicable.
The paper is also extremely fishy. The statistic referenced in the abstract in that the odds ratio of contracting RT-PCR-confirmed influenza, when intervention was applied within 36 hours of symptom onset, was 0.46 (95% confidence interval: 0.15–1.43) for hand hygiene only, and 0.33 (95% confidence interval: 0.13–0.87) for hand hygiene + facemasks. That’s hardly a ringing endorsement of mask wearing, considering the wide confidence intervals. Also, the very same Table 5 shows that the odds ratio of contracting clinical influenza under definition 1 was 0.46 for hand hygiene only, and 0.86 for hand hygiene + facemasks. Under definition 2 of clinical influenza, the odds ratio was 0.64 for hand hygiene only and 1.45 (higher than the control) for hand hygiene + facemasks. When all influenza cases are included, and not just those where intervention was applied within 36 hours, the odds ratios are 0.57/0.77 (RT-PCR-confirmed), 0.92/1.25 (clinical 1), and 0.81/1.68 (clinical 2).
So to sum up, the only relevant paper the NYTimes cited found that wearing facemasks INCREASED the chance of infection in 5 out of 6 scenarios (not necessarily by a statistically significant amount), and only decreased the chance of infection by a statistically insignificant amount in 1 out of the 6 scenarios. That, again, is hardly solid proof that wearing masks is a good idea.
Respirator masks really aren’t rocket science. You don’t need to be a trained professional to figure out how to put one on. Sure, trained professionals will likely make fewer mistakes, but if the effect of the mask is reasonably large, laypersons won’t make enough to completely negate the effects.
That might be true, but nothing that Scott links to proves that. They certainly don’t show that “the government deceived us” as part of a Noble Lie.
Then how comes most of the people I see in the supermarket are wearing them wrong?
Thanks for pushing back on this. No promises, but I’m hoping to write a longer post looking into this in more detail.
There’s also this paper supporting the use of masks although only in a household setting.
The surgeon general made a blanket statement that masks are “NOT effective in preventing general public from catching #Coronavirus”; not sure why you are singling out the CDC, since Scott had commented about guidance in general. That said the CDC advice was also somewhat misleading e.g. they said “CDC does not recommend that people who are well wear a facemask to protect themselves from respiratory diseases, including COVID-19”, but then later in the same recommendation acknowledged that people should use masks if caring for someone at home (though the latest CDC recommendations page has remedied this).
The claimed difficulty of properly using/fitting N95 masks is also mostly a red-herring, since there’s little evidence that they are more effective than regular surgical masks; for instance this study found no difference in effectiveness for “flu and respiratory virus protection”. Also, see eigenmoon’s link/study suggesting that masks help to protect non-professionals in household settings. Furthermore, if masks are helpful in household settings, it’s likely that they are also somewhat beneficial in other close quarter settings (e.g. public transport), not to mention benefits in terms of protecting others (from asymptomatic transmission).
In general, the misleading messaging on masks has surely had a harmful effect in terms of undermining official credibility.
https://covidactnow.org
This site was launched earlier today and has a USA state-by-state model comparing four different scenarios: do nothing, social distancing, shelter in place, and Wuhan-style lockdown.
The difference between doing nothing, social distancing, and the lockdown-style measures is striking: with shelter in place, it indicates my state, California, will never overload its hospital bed capacity.
Here are the assumptions and the massive Google Sheet model the site is based on if anyone wants to check the numbers. I spent 30 minutes on it myself and didn’t see anything egregious.
I have a very hard time believing the California style blind shelter-in-place is going to change R0 numbers by that much. I would not be surprised to see it not change them at all. Bruce Aylward of the WHO has argued that it wasn’t the general lockdown that turned things around in China, but the very aggressive testing, contact-tracing and fast-acting effective isolation of trouble spots. He describes it in this NYT article. It’s very impressive, the speed, specificity and energy with which the Chinese did those things.
I have a very hard time believing the California style blind shelter-in-place is going to change R0 numbers by that much.
Do you mean compared to shutting most things down, or compared to business-as-usual?
*EDIT*
very aggressive testing, contact-tracing and fast-acting effective isolation of trouble spots
My current assumption is that one of the goals of our current mitigation strategies is to let us get to the point where this works. You need (a) a manageable number of cases and (b) lots of tests. I don’t know exactly where we are on (a) but we are buying time for (b) which feels to me to be growing significantly by the day.
Regarding how many tests are out there, the best source of numbers I know of are from the Covid Tracking Project, which has the US numbers for each day here.
This would be more effective if it said more about how the numbers for R0 under the various scenarios were justified/derived/guessed. As it is, what it says looks awfully like:
1. anything that lowers R0 to <1 saves a ton of lives and prevents sustained overloading of hospitals
2. anything that doesn't, doesn't
3. here are some numbers we made up about what will or will not.
Maybe it's helpful to hammer yet again on (1) and (2), but these seem like common sense already to anyone who knows how exponentials work. And while I, in CA, would love to believe that their numbers on (3) are right since it indicates that all this sheltering in place will be worthwhile, it's not clear why I should believe that– or for instance why I should believe that the R0 reduction value of shelter-in-place will get better over time, rather than e.g. getting worse as people come to find it harder to endure psychologically.
I’m surprised they give a R_0 of 1.7 to what they call “Texas-style” distancing. And the assumption is “schools may be closed,” and it seems like the schools being open or closed would matter a lot for that assumption.
Or not, depending on whether kids are super-spreaders despite very rarely getting symptoms. Which school closings assume they are, but which I don’t think is known with high confidence, is it?
Highly suggest following Bill Mitchell on Twitter for some incredible denialist takes. An interesting case study.
Is Shrek gonna die?
I don’t do twitter and don’t know who Bill Mitchell is. Can you elaborate on why he makes an interesting case study?
I’m confused by many of the explanations I see concerning “herd immunity”: https://en.wikipedia.org/wiki/Herd_immunity.
Frequently, the implication seems to be that because of herd immunity, considerably less than 100% of the population will become infected during a pandemic. This might be true for other reasons, but I don’t think this can directly be explained by herd immunity. In my understanding, herd immunity is formula saying that the “effective R0” of a disease goes down as the immune percentage of a population increases. If 50% of the population is immune, a disease with R0=1.5 only causes .75 actual new infections, thus any “point” introduction of the disease into the group fails to spread, with only a fixed number of new infections per new introduction.
But as far as I can tell, this property only applies when in the steady state of an uninfected population. It doesn’t directly tell us much about what percentage of the population will end up infected when starting with a large number of infections. This would requires a different calculation, based on the chance that an non-immune person will run into contact with a carrier, and the chance of infection per contact. I haven’t tried doing the math, but I’m pretty sure that if you start with a highly contagious disease with a significant percentage of the population starting out infected, the total number infected ends up much higher than the Herd Immunity Threshold.
Is my understanding wrong? Does Wikipedias claim that Covid-19 has an R0 of 1.4-3.9 really mean that we should expect the initial spread of the virus to stop on its own with only 29-74% of the population infected?
Yes. What you call “effective R0” is the “effective reproductive rate” and is just called R, and the expected proportion of infections is expected to stop growing at (1-1/R0). However, this is not the total proportion of the population eventually infected. That’s called the epidemic final size (I’ll call it F) and is given as
F = 1 – e^(-R0*F)
It’s not a closed form but Wolfram Alpha tells me that with R0 = 2, it’s about 80% of the population infected. With R0 = 1.4, about 51% of the population is eventually infected; with R0 = 3.9, 98% of the population is infected.
This is in the simplest model — fixed length of infection, homogeneous mixing of the population.
Thanks, that’s very useful. Having the correct terminology makes searching much easier, and brings up lots of papers on the topic. I’m finding this one helpful in thinking about the problem, since it defines its terms well:
A note on the derivation of epidemic final sizes
Joel C Miller; Bull Math Biol. 2012 Sep; 74(9): 2125–2141.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3506030/.
Over on Overcoming Bias, Robin Hanson has been posting wacky ideas like deliberately exposing people to COVID-19. One variation on this is to develop a predictive model re: who requires hospitalization. This predictive model could take into account factors like: age, pre-existing health conditions, the strain of COVID-19 they caught, whether they were getting enough sleep, what supplements they were taking, and all the rest. Then institute some kind of relaxation of quarantine rules, but only for individuals who your predictive model says won’t get hospitalized (or otherwise reduce hospitalization based on predictive model learnings by e.g. widely sharing supplements which make the thing milder). That could allow for faster development of herd immunity.
You could also use machine learning to identify individuals who have COVID-19 strains that seem unusually mild (“the model says they should have died but actually they survived, and they’re all located in one city”–could do this with a categorical variable for each city and see which have coefficients strongly related to increased survival, esp. if other regional stuff like temperature is also included in your model). Then publicize this fact and encourage people who want to self-vaccinate to travel to that city armed with lots of water, supplements, etc. so previously infected can cough all over them. And loosen quarantine measures in that city of course.
A few pretty interesting points related to keeping R ~ 0.5 only for a few weeks and then being able to relax social distancing to a point where R ~ 1 until the crisis can be understood better, testing ramps up and a vaccine is found:
https://medium.com/@tomaspueyo/coronavirus-the-hammer-and-the-dance-be9337092b56
He calls it the “Hammer” (R ~ 0.5) and the “Dance” (R ~ 1).
Skimming briefly through this, it seems qualitatively about right. But then I get to Chart 3, “Infections and Deaths if we do nothing in the US”. And he’s got 11.5 million dead. That seems a bit off. Looking into the details, he’s got the mortality specified as 4% because of overtaxed health care system. OK, but 11.5E6 / 0.04 comes to 285,000,000 total COVID-19 cases.
In a country of 328.5 million people, meaning his (borrowed) model is predicting 87% of the population will be infected.
That’s way off; corresponding to the herd-immunity equilibrium for R0 = 7.55 using the simple and conservative model. But, looking again at the fine print, he’s got R0 set at 2.4.
So, I’m not trusting the numbers on this.
87% is the peak fraction of infections for R0=7.55; the fraction of the population infected before the epidemic stops growing. But what he’s giving is epidemic final size, which is quite a bit higher
F = 1 – e^(-R0*F)
Which for R0 = 2.4, Wolfram Alpha tells me is 88%.
So he’s right.
a website for predicting the spread of Covid-19. no specialist knowledge required.
https://delphi.cmu.edu/crowdcast/signup.php
How fucked is US? EUR/USD futures are falling, but not by amount I would expect from uncontrolled epidemic in a country with joke of a healthcare.
Edit: I misunderstood the direction of EUR/USD. The fact that futures are falling is… even more incomprehensible?
The American healthcare system has many problems, but none of them should result in worse die-offs and illnesses from this than in Europe, if I understand your statement correctly. Maybe a lot of now-unemployed-and-thus-uninsured people will find themselves with 10K+ in bills after a hospital stay, but that’s not going to destroy the value of the currency.
I mean, that is exactly the reason why they will stay out of the hospitals if possible, leading to more and more infections.
Underinsured people staying out of hospitals wont be a meaningful driver of infections because they will just be staying home. If America has a systemic risk that Europe doesn’t is that our safety net is less robust so more service industry workers may go into work than would in other countries. This is largely being handled by governors and mayors shuttering service industries like restaurants. The other major systemic risk is that herding Americans is much more complex than herding Germans, or Swedes. Partially that is because of our much higher racial diversity, but its also cultural diversity, even our “white people” are both Germans and Swedes and English and Polish!
New political slogan: “Diversity is our weakness, but we’ll manage!”
Why would they? As far as I understand, most of the people infected are asymptomatic (and some are still able to infect others).
@deltafosb
…
If they’re asymptomatic, they won’t be going to hospitals, no matter what funding structure is in use. Unless I missed something, no country is admitting people to the hospital unless they’re in dire need of immediate emergency care.
And if they’re one of the unlucky people who get hit hard by the ‘Rona, they’re probably going to get an ambulance ride and get shoved into an ICU no matter what their financial status. They will have a huge bill at the end of it, though.
As stated, the problem is people going to work when asymptomatic.
In what way is that affected by the healthcare industry model a country uses?
@Clutzy, @CatCube
I admit, you are right about this. I still feel uneasy about people with mild flu-like symptoms though, since they are effectively disincetivised from seeking any medical help. God forbid they might test positive, be quarantined, lose their job and later be billed for that.
Poor people can’t lose their jobs because of Coronavirus if they lose their job because of the Coronavirus quarantine first.
*meme of guy pointing to forehead*
Consensus for now seems to be that EU will be much worse off than the US. Part of that will be that EU monetary policy is so so bad. US is bad but much better than the EU and we’ll see, maybe they’ll switch to level targeting and much of the recession will be alleviated. It will be a bad recession no matter what but it will be much worse if the central banks allow deflation.
The USD has spiked because everybody is trying to get cash. It’s not a vote of confidence in the US. They are selling other assets, even US Treasuries, in order to obtain cash.
Isn’t the Euro cash as well?
When I asked my friend exactly the same question, he replied “If you are a US boomer and see the stocks falling, you just click SELL and don’t bother with some commie currency” (he’s more of a r/wallstreetbets kind of guy). Efficient market hypothesis should take care of this though.
There are lot more stock holders in the US than in the EU, since Europeans have their retirement in public pension schemes.
If 5% of the European population want to liquidate their assets, and 20% of the US population want to liquidate their assets, it will put more preassure on the Dollar than on the Euro.
This map uses internet-connected smart thermometers to track flu-like illness over certain areas of the united states.
NIMBYISM – Not just for bay area housing anymore!
UPDATE: Darien’s drive-through testing has been canceled, according to a tweet from First Selectman Jayme Stevenson. The testing was to start Thursday. Some neighbors expressed complaints with the location of testing so close to their home on social media.
In a press release from Town Hall, First Selectman Jayme Stevenson and Department of Health Director David Knauf said “We appreciate the important work being done by Murphy Medical Associates to provide testing to our residents at their other locations.”
Just a flu, bro.
Ioannidis is estimating CFR from the Diamond Princess cases and correcting for age, but this probably yields an underestimate: people who go on a cruise, while older than the population average, probably tend to be in relatively good health for their age group. Also, these people were being monitored closely and promptly treated by a still not collapsed health care system as soon as they developed the first symptoms.
It could be that the low corona 19 rate of death amongst the young is an indication that the the corona 19 statistical model is a piece of shit.
If that is the case it is very good news (and of course very bad news as to how susceptible mankind is to hysteria and influence/manipulation)
I’m confused, what’s the good news?
Along these lines.
https://www.statnews.com/2020/03/17/a-fiasco-in-the-making-as-the-coronavirus-pandemic-takes-hold-we-are-making-decisions-without-reliable-data/
Scott, The WHO’s guide to mental health during the outbreak had the following advice:
https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf?sfvrsn=6d3578af_8
“Minimize watching, reading or listening to news that causes you to feel anxious or distressed”.
I’m curious how you feel about this as a psychiatrist. The way that OCD and anxiety disorders work is that avoiding news that makes you anxious or distressed makes your condition worse. For example, if you’ve got OCD about contaminating others with germs, and you change the channel every time news about Ebola pops up, your OCD will get worse. So basically The WHO gave advice that might or might not be helpful to people who are a LITTLE worried but is actively harmful to people suffering from actual disorders, who need help the most.
Possibly just not watch the news? At all?
Though the OCD complaint I have heard is about the barrage of “wash your hands! wash your hands! now now now you’re not doing it enough no one’s doing it enough WASH YOUR HANDS!” messages and their effect on OCD patients who compulsively wash their hands.
The linked map of tests conducted per country appears very out of date at this point. Two different sources have the US on about an order of magnitude more tests than this.
For a half decent cross country comparison, see link text but even this is several days out of date at this point, and testing can change very rapidly.
The specific fact this references (Jack Ma donated 500k coronavirus tests) is presumably correct . But I’m skeptical of the description, and it could be wildly off. Once the CDC corrected its initial mistake, it sent off 1.5 million tests to state labs within a couple days (about 2 weeks ago now); here is one link but this number appears in many places.
But those 1.5 million tests are also described as “2,500 new test kits”, so 600 tests per kit on average. Is Jack Ma really donating 300 million tests to the US? Seems plausible that terms are being mixed up here… South Korea, which has been widely applauded for its testing regime, has tested ~200k people.
In any case, given that the CDC was able to send 1.5 million off in a few days (once it ironed out the bugs), this is not where the shortage is. The shortage is on actually running the tests – in particular the machines that take the test samples and analyse them. Whether it’s 500k or 300 million tests, Jack Ma has bought himself some nice press but this likely has approximately no effect on how many tests the US can actually conduct. Which is in the ballpark of 25k a day, and is rising rapidly.
https://news.rice.edu/2019/05/01/student-invention-gives-patients-the-breath-of-life-2/
Give it web access, and add a webcam for the bedside monitors, to multiply the capacity of a qualified respiratory therapist who works from a central monitoring station. The therapists could be RT students under permanent supervision, similar to flight controllers.
Even better but probably taking a bit longer to set up: integrate patient monitor and respiratory control in one tele-respirator package.
Someone at the bedside is also necessary, but that can be low-skilled med or nursing students who only have to learn how to disinfect themselves and check/correct masks; leaving everything outside this specialization to competent nurses.
re:ventilators:
10 years ago MIT designed a $100 ventilator for disaster zones.
http://news.mit.edu/2019/umbulizer-sloan-health-care-innovation-prize-0225
But you couldn’t build and use it in the US.
1: the government would shut you down if you tried and insist you spend years getting certificates because the regulatory environment is 100% fine with people suffocating for lack of access to a medical device because that’s considered nobodies fault.
2: the courts would fuck you. if you produce 10,000 of them, save 5000 lives and some people die (who would have died anyway without the ventilator) because a part failed then their next of kin will be allowed to clean you out even if you handed out the devices for free.
Great reference and thanks, but all the articles say the Umbulizer costs about $2,000 to make, not $100. (Which is still a lot cheaper than $30,000). From what I can tell, it’s pretty much a ventilation bag and a squeezing machine, but there’s probably more to it.
gah, I linked the wrong one.
https://www.fastcompany.com/1661942/mit-students-invent-100-ventilator-for-disaster-zones
I don’t see a lot of discussion about the OP’s “End Game” segment. The difficulties of one proposed strategy, an on-off NPI set (social isolation, quarantines, closings, etc.) where the switch is thrown based on contagion or death rates, providing “a couple of weeks of normal activity,” seems to me to be incredibly complex to implement in reality.
How would it be done? Do the Feds say “NPIs turned off” and all government bodies and industries nationwide flash into action to provide all the goods and services that weren’t being used during the high-NPI segment? (If it’s not coordinated, you get tons of people going from the locked down areas to the unlocked areas, which is really bad.) Then, if contagion/death ramp back up, they say “NPIs turned on” and everything shuts down? (This would happen based unpredictable disease statistics, producing unpredictable durations of “normalcy” followed by unpredictable durations of “shutdown.”) The graph shows them as clean and neat, which to me seems extremely unlikely.
It seems to me that if we tried this, it would drive people crazy and ultimately end up back in the original UK “herd immunity” proposal.
I’m moderately skeptical about the claims that reducing GDP is going to substantially reduce life spans. I feel like the correlation between GDP and lifespan is plausible, but GDP is a proxy measure for other factors – e.g. sanitation, hand soap, access to antibiotics – that save lives, and aren’t going to just go away if there’s moderate societal disruption.
Depends on your timeline. I imagine that there are several technologies that will prevent global warming (or advance medical research, or make safer cars, etc) that were due to be invented in 10 years. With this drop in GDP those things will certainly be delayed.
There also may be less disposable income available for charitable donations.
The increase in unemployment and loneliness may increase suicides.
The big “other factors” are food, shelter, clothes, central heating, and things like that. Not medicine.
I hope I don’t sound morbid — I don’t have a problem with analyzing things apart from emotion — what I’m wondering is:
How would the overall death rate of the US change if coronavirus went unchecked?
This article says a 1.4% death rate in Wuhan — if you get the virus. The governor of California estimated ~50% of people would get the virus, in a business-as-usual scenario. 50% of 1.4% is about .7%.
Since the predicted life span of a US citizen is ~70 years, I would expect that a little over 1% of people die each year. I quick check of CDC says something like .86%. I guess that is because we have more young people than we have old people?
If you add the two numbers together, you get 1.56%. Obviously, that’s a lot bigger than .86% but not that much.)
But does it make sense to add those numbers together? As in, how many that die from Covid would have have died anyway?
For Spanish Flu (the thing we keep comparing it to) a lot of young, healthy people died. Those people would have been unlikely (or less likely) to die without the flu. But for Covid, it seems to affect those that are very old and/or already sick.
We know that Covid is much more likely to kill older people. Absent the disease, those people would die at a much higher rate than a typical American. This study in Italy says that 99% of those that died already had existing conditions (half had three or more!)
So, of the .7% of people that would die from Covid, it seems like those people would normally die at a rate on the order of (wild estimate) 3-5%. So these people would go from (say) a 1 in 25 chance to die to a (say) 1 in 20 chance. All of this is over the course of a year. Whereas the rest of the population would see a tiny tick up in death rate — though not sure how to calculate that.
This is what I’m curious about. Did I make some bad math mistakes here? Would love to hear other people’s thoughts on this.
I would first point out that pre-existing conditions here include things like asthma which have a relatively small effect on life expectancy under normal conditions. I too would like to see numbers on this. There’s a difference between “kills mostly people who had <3 years to live" and "kills mostly people with underlying conditions that in and of themselves don't have a large effect on lifespan".
It’s an interesting question.
There’s at least one bad premise here. 3-5% is likely a wild overestimate. People who live to 60 are *way* more likely than average to live past the average lifespan. Infant mortality rates drag the average lifespan down. There are other factors – men also tend to die a lot in their teens and 20s, so if you survive those danger years, you’ve upped your odds of a long life. This is the kind of stuff actuaries calculate when they’re pricing life insurance, and demographers calculate just because.
That’s fair.
But let’s say everyone that reaches 60 will eventually make it to 100. That’s 40 years. That means that 2.5% of the people between 60 and 100 will die every year. Right? Or am I missing something?
It’s not exactly a “math mistake”, but I think the weakest part of your chain of logic is the assumption that Wuhan’s 1.4% Case Fatality Rate (CFR) is a useful predictor of future fatality rates. The CFR is (likely) very dependent on the quality of care that the infected receive. In Wuhan, my impression is that the medical system was still mostly working, and most people received professional care. If the number of infected was greater, the number of people receiving high quality care would drop. The drop is not linear, but has a sharp “kink” at the point where the number of appropriate hospital beds is less than the number of infected who would benefit from being in on.
What’s not known (to my knowledge) is the impact that absence of care has CFR. That is, how many of the untreated but infected die (or are permanently disabled), and how does this depend on their age and prior health condition? Without reasonable estimate of this rate, I don’t think it’s possible to make accurate predictions, and I don’t think we currently have any reasonable estimates. I think the best we can say is that the “untreated CFR” is probably something greater than the ~1% “observed treated CFR” and almost certainly less than the current 5-25% hospitalization rate. Depending on where within the range the actual number is, and if we assume a high infection rate, the societal effect ranges from “bad flu season” to “worst humanitarian catastrophe the modern era”.
Can anyone point to better estimates for what the outcomes of the untreated actually are?
Yeah, there are quite a lot of unknowns right now. FWIW, this article in the NY Times says the CFR in South Korea (with good health coverage) was 0.8%. Which is about the same percentage of USers that die in a normal year.
Honestly, I spend too much time thinking about it. When I do, I oscillate between thinking we are over-reacting and we are under-reacting. My current tilt is over-reacting, but that will probably change tomorrow 🙂
Over-reacting to a catastrophic risk (such as a country-wide epidemic) means you wasted a bit of effort. Under-reacting means you suffer a catastrophe.
Which should a rational man risk?
This thing can grow by a factor of ten every week. Every week you delay your response means ten times as many deaths. And here we are, wasting time.
Over-reacting in this case could mean wrecking your economy to the point that you have reduced or eliminated your capability to fight global warming, or cancer, or poverty, or another pandemic.
No, it means you caused actual harm, possibly quite a lot of it.
All of California is under shelter-in-place at this point, other states are following suit. What’s the level of reaction where you say “good enough”?
You are massively underplaying the risk of overreacting.
I live in IL, and I think this quarantine is likely to kill 100k people in the state indirectly if it lasts much longer than 2 weeks. The unemployment is a killer, the misunderstanding people have a bout staying inside, etc.
I am fine with the shelter in place orders.
For now.
But we really really need to think about what lesser measures we can do. I am way above average in conscientiousness, and I am feeling it starting to drag on me.
And if the reaction to any discussion of lesser measures, even here on SSC, is “won’t somebody think of the
childrenelderly?” then we’re doomed and let’s just burn it all down now.Over-reacting in this case can mean you don’t just wreck the economy, but you cause infrastructure to shut down.
Quoting myself from reddit:
If people want to eat, farmers have to farm. Trucks have to move materials. Warehouses and stores must be running. Repairs must be made. Manufacturing of equipment and parts must happen. Ships must be unloaded. Water must be purified, filters must be cleaned, sewage must be treated, and the roads must roll. At some point, you stop people from going to work and this all breaks down. And I think it’s often non-obvious what parts you can safely shut down.
At this point the numbers from my area (NYC area) make me pessimistic on the possibility of achieving South Korean levels of containment before breaking something like in the above paragraph.
All of California (about 40 million people) is now ordered to “shelter in place” except for “essential workers”.
I wonder if the across the street housing construction will stop now or if San Francisco will still deem that “essential”?
Construction of housing, public works, and medical facilities is exempted under the order.
The single thing that is hitting me hardest in all of this is that I have one living grandparent on each side. Each is well over 90 and despite no specific health concerns is reasonably likely to die in the next six months completely independently of COVID-19. One lives alone and normally sees family multiple times a week, and family assist with various household tasks, and cleaners come by, etc. The other lives in an apartment in a senior community. Neither uses video chat. One has never used the internet.
There is a very real chance these people are going to die alone, in squalor (if cleaning services halt), having not seen their family or interacted with another human in the last 4+ months of their lives. That feels blatantly unethical to me. But I don’t know what else to do.
Agreed. I have a 90 year old grandfather who lives in Northern California and is currently undergoing chemo. I have similar concerns.
I am very sad for your situation.
Me and my siblings are thinking about renting a separate house near my elderly parents. We could physically see them and help with a lot of things, but missing physical contact sucks.
All I can see next is to do a second-level quarantine, where we choose one of us to live with our parents, but that person is also quarantined, never leaving the house.
I am semi- considering fully quarantining for 2 weeks and then moving in with my grandfather but I don’t think the logistics work. Driving (gas stations) or flying would break the quarantine, and I don’t have confidence that I will have the freedom to travel across states in 2 weeks. I guess the alternative would be to travel there first, quarantine for 2 weeks, and then move in with him? I’d have to quit my job because he does not have internet and I don’t think we can get it installed at this point. And I’m currently the only one in my family with secure employment.
Are you sure you can’t get it installed for him? It might be worth trying. Keeping an internet connection working is probably an essential service these days.
We had a discussion in a prior thread about how to keep clean while driving and/or flying. https://slatestarcodex.com/2020/03/15/open-thread-149-5/#comment-865773 It depends how far you have to drive.
“Two weeks” is the outside window where people who have caught it are 99% likely to show symptoms. You can do it shorter, like one week, if the risks of you not being there are
You could try sending a non-working sibling, but the things that make people non-working tends to make you worried they would break quarantine. I know when I think about sending one of my parents’ grandkids to take care of them, I’m not sure they would be properly serious.
While most of my cousins and siblings are now non-working due to closures in the hospitality, entertainment, education, and leisure industries (not sure why that would make them more likely to break quarantine), my grandfather’s house has enough mold and other issues that I am the only one with the health to be able to stay there for weeks/months. My mother also can but she is 60+ and in shelter in place in California. I am not in California. My grandfather is >1,000 miles from either of us.
(not sure why that would make them more likely to break quarantine)
Sorry, I was projecting a bit there.
My family has some people who are non-working, but weren’t working before, and the ones of us who are working aren’t sure they have the conscientious to follow the steps for proper hygiene each and every time like it really matters.
Ah, yeah that’s different. We all had stable employment or college 2 weeks ago. Now I’m the only one in my generation. I haven’t checked on the generation one above but my guess is they are also down to 1-2 across my grandfather’s children and their partners.
You can connect to the internet via a cell phone, although it isn’t a very fast connection.
It depends. My cell phone’s connection is fast enough for watching movies with reasonable quality and for teleconferences with video on, so much that I’m not even considering getting a wired ISP subscription as it’d be several times more expensive. (And that’s in Northern Italy, where networks are most likely way more busy than usual from all the people working from home or watching Netflix instead of going to the pub.)
It doesn’t help with the cleaning, but it would be nice if someone could develop a completely user-free video chat. (Some of those muppet commercials make the facebook one look like that.)
I have a friend whose father is in a similar situation – no visits from family, living in an assisted living home, can’t operate video chat on an iPad, and pretty much the only things he enjoys are visiting with family and sports.
What’s the most reliable video chat you could set up? Something that would let people call him, then presumably have him accept or decline calls by voice command, and that was unlikely to need technical support beyond “plug it in.”
A tablet that’s plugged in and always on, with a bunch of big buttons with names of people to call. Googling “Tablet holder” shows quite a few practical designs too.
It increasingly looks like coronavirus can manifest in infinite ways, including not at all (entirely asymptomatic). The guidelines right now seem to be, if you have *any* cold or flu symptoms, don’t go out *at all*, otherwise, don’t go out more than necessary but walks are fine, the grocery store is fine, and please do go out if you, say, are the cook at the local elementary school who is still preparing lunch for 200 students a day.
I’m unclear of what this actually means in practice. Let’s say I have mormal-for-me symptoms of seasonal allergies and live on the 12th floor of an apartment complex with my two dogs. These allergies will last months, during which I’m not supposed to leave the apartment. Do I let my dogs go inside for that time? Do I let my trash pile up? Or maybe if I’m reasonably confident it’s allergies I can go out. But if I develop a fever I definitely shouldn’t but am still stuck with the same issues. Are things like dog walking and trash removal being addressed in any way in the U.S.?
Looks like sneezing is not a corona symptom (which makes me sneeze with sheer abandon and pleasure) and a runny nose is a rare one. So if that’s the extent of your allergies, I think you can go on as usual and maybe be prepared to explain your allergies.
I don’t know if this has been covered here already, but apparently the initial CDC primers suffered from massive technical incompetence in design. My understanding is that there’s a definitive free online “validate your primers here” website where you can test to make sure your primers won’t stick to themselves, etc., which would have caught all of these issues. My reading on Reddit is that primer design is a fairly basic lab skill these days – that the CDC screwed this up this badly is disturbing.
I could be wrong, but based on what I have read, it sounds more like the CDC error was in manufacturing, rather than in design per se. Which is why some state labs could get them to work (I presume, by luck, they got clean test kits) while others (who got compromised ones) could not. Also this seems consistent with the fact that labs could have swapped the faulty reagents out for identical (except for not being faulty) ones they themselves got produce, except crazy FDA regulations didn’t allow them.
A look at the data from this site shows that the daily percentage increase (in the U.S.) of positive tests is just about the same as the daily percentage increase of actual tests.
That seems to suggest that the growth in case numbers is strongly dependent on the growth in tests.
How do modelers tease these two apart, especially given all of the obvious confounders of trying to use data (which might have similar issues) from other countries (that have wildly different demographics/societal structures)?
Thanks for the link! I’d been hoping to find a data source for daily tests.
This site uses a different methodology but comes out with numbers in the same ballpark. They also have a graph of the positive test %, which makes your first point particularly clear.
I think it is very hard to do this, until testing expands enough that the positive test rate falls. If this never happens, well then we are in trouble… either it means testing capacity stalled (a bad thing) or 8% of everyone already has it / will have it shortly (the only silver lining here in this eventuality is that this probably would imply the mortality rate has been substantially overestimated).
They have criteria about who they test. If that doesn’t change then the rate shouldn’t change much if test supplies are decent. If they loosen the test criteria and the rate doesn’t change that would be deeply weird.
Here is data from one specific lab in WA (which is where the first big outbreak was detected).
It looks like the % positive rate has fallen slightly over the past week. But it is remarkably stable, yet testing has grown a lot. Either they are barely keeping up with the growth in unobserved cases, or whatever methods are used to determine testing priority are not particularly good at telling high probability cases from low probability ones.
https://twitter.com/adam_tooze/status/1240771475604414465
Can these layoff numbers be correct? If they are, and considering that they’re from before California’s lockdown announced a few hours ago, I kind of want to panic. There’s no way these measures can possibly be worth the cost.
Numbers smell right to me. 10% of the US labor force is in Leisure & Hospitality (~90% gone), 10% in Retail Trade (~50% gone), 13% in Professional & Business Services (unsure, ~75% gone?). Unless there is widespread labor hoarding, at least half the workforce will be out of a job shortly from the spillovers from this first wave of industries.
My very rough math says averting my baseline scenario is worth around 4 months of GDP, but expected benefit is somewhat higher because there are kind-of plausible worse scenarios (permanent lung damage in survivors, worse-than-expected mortality, short-lasting immunity, reduced male fertility) that it would be worth 2+ years of GDP to avert if true.
These seem like bad estimates
I’ve waited a bit to reply to this. I was wrong to claim a short timeline as I had expected shutdowns and shelter in place to be rolled out at a faster pace than they have. Assuming the shutdowns continue for at least 2 months for > 90% of the population (currently ~97%), I continue to expect around 50% decrease in employment (including furloughed employees as non-employed) by July. Happy to arrange a bet if you believe something different enough, let’s say less than a 20% decrease in employment.
Agreed.
It sounds unfathomable, but as far as I can tell, nobody actually even attempted attempted a cost-benefit analysis on this. Nobody attempted to quantify the cost side of things, at all. They just heard “MILLIONS WILL DIE IF GOVERNMENT DOESN’T ACT” so they said “OK, let’s act!” and now we’re here.
You must be new here.
This pattern-matches pretty much every single big social intervention I am familiar with. It was only a matter of time before we got here and we should thank our lucky stars that it has happened with something so fundamentally benign as COVID-19.
We’re probably stuck making a Cost-Ineffective™ strategy.
But we should be doing different Cost-Ineffective™ strategies. From all the possible Cost-Ineffective™ strategies that exist, I doubt that “just lay-off 25% of people,” which we just stumbled into, is the cheapest.
Like, hire screeners with IR thermometers at every restaurant (which now has 50% less seating). This is, normally, an insane proposition, but in the universe of Cost-Ineffective™ strategies, it’s down right rational.
The British did, came down on the side of not shutting everything down, and the public outcry made them reconsider.
“We’re going to let your parents/grandparents die to save the economy” may be right in the cold light of day, but it’s not politically viable.
Every detailed report on government decision-making I have seen is clear that the new academic paper out of Imperial university made them reconsider.
That paper very explicitly did not take any economic costs into account:
https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020.pdf
Yes, I am responding to the claim that public outcry was the cause of the change in policy.
Obviously, though, that new information could have influenced the costs-benefit analysis that may or may not have been taking place inside the government.
See e.g. https://arguablywrong.home.blog/2020/03/12/epidemiological-modeling-costs-of-controls/
Of course, it’s not massively rigorous, but nor is anything else as far as I can tell.
Of course they can be worth it. People are (somehow) still stuck assuming that we have a fairly good understanding of what society would look like if we didn’t do anything and just tried to go about our daily lives. We don’t.
First, we don’t know what the real death rate is. We have estimates that run the gamut, and even those are predicated on assumptions like, “Some people get proper medical care” that could fail if enough people are sick/dying. The worst cases aren’t likely, but they’re very bad.
Second, “business as usual” isn’t an option. If you think “shut it all down” is an overreaction, you have to state what bits you’d select to shut down, how that ends up as a stable equilibrium, and what the effects on spread of SARS-CoV-2 are in that scenario. You don’t know any of those things, so you’re left with tons of uncertainty, which includes huge down-side risks. If you think “no federal/state actions” is the right COA, you have to argue why society will still function when some notable percentage of the population dies off over the next few months. I just don’t think we will tolerate that.
Third, our current state is path-dependent. People did things and made choices two+ months ago that determine where we are now. If you want to argue for an alternative, you need to argue when that decision needed to be made and why it would have been the right decision at the time with the relevant information available. (This, I would argue, isn’t that hard. It was clear in early/mid February that we were going to get hit by this, and it was clear in January that there was obvious prep work we should be doing, including getting our shit straight on tests. Those were the times for decisive actions, but, like much of the West, our leaders opted to down-play the threat in every way imaginable.)
Yes it is.
You may not prefer it, and you may be correct that it isn’t the best option. But it’s definitely an option.
More granularly, there are a bunch of logical levels of restriction one could imagine:
1. business as usual
2. large gatherings/events banned, otherwise BaU
3. large gatherings banned + “nonessential” businesses closed to the public, but schools remain open
4. (3) plus schools closed
5. (4) plus “nonessential” businesses closed entirely and even small “nonessential” informal gatherings banned, aka CA current state
6. (5) plus stricter enforcement and narrower definition of “essential”, aka Italy current state
7. Wuhan in February
Arguably it’s at most justifiable to do the least restrictive of these that produces R0 < 1, and right now nobody knows what that is except that (7) is sufficient and (1) isn't. It would be really really useful to get better models/analyses, along with data on e.g. how much kids actually spread the disease, that would let us understand whether e.g. (3) might be enough. Because (3) is waaaaay less costly and more sustainable than the more restrictive stuff.
Can a society actually maintain business as usual in the face of say, 2% of the population dying, and 10-20% at a time being ill?
It might be the best decision, but it’s not going to feel fine. People will be scared. Scared people make different decisions. You can’t do top-down control to stop people being scared and taking their own precautions.
What will people actually do in the face of a severe and uncontrolled epidemic? Well, for starters, people who can afford it will isolate, and work from home if they can. People who can’t will be very upset about facing a different risk of death to wealthy people. Rioting is risky enough during a pandemic that I think it’s unlikely, but I’d be very, very worried about what happens after it’s over. Most poor, but young and healthy people will survive. But they’ll all know at least one person who died, and likely be very, very angry about being abandoned to face the risks.
On a realistic level, you get things like what’s happening currently in Iran, and what’s happened in most major epidemics in human history. Rural communities start setting up roadblocks and trying to stop people getting into their towns. Rich people flee the cities, carrying the illness with them.
Business as usual during a major pandemic isn’t actually possible.
If it’s heavily weighted towards the elderly, I’m guessing probably yes. Close to 1% of the US population dies in an average year anyway. We should try to avoid this, but we should’t kill ourselves trying to avoid this.
@John Schilling:
The 2% of the population dying is heavily weighted towards the elderly (so long as there are enough ICUs for everybody), but the 10-20% being ill is only moderately so (there are plenty of 60-, 50-, even 40-year-ods in ICUs).
@John Schilling
Pandemic deaths look different to the normal pattern though. I’m not saying it’s not the rationalchoice. I’m saying that if coronavirus comes to smalltown x, pop. 10,000, exponential growth means there’s a space of like a week where half the town gets infected. 2-3 weeks later, the morgue has 200 bodies in it. Probably at least one doctor, plus everyone who couldn’t get their car crash/heart attack seen to because the hospital was overwhelmed. That’s really different to the usual 1-2 deaths a week. It’s scary. It feels world changing. Even if it isn’t, it feels like it.
You might be able to decide to carry on as usual, to venture out of your house even though you risk infection, but you’re a SSC reader. You’re a weird outlier. We have really strong instinctual fear of illness, and that changes behaviour.
This thing is also a really nasty illness at the “mild” levels. Having 10% of your workforce out is a serious problem for a lot of places.
We’ve stopped basically all routine dental work in the UK because the dentists can’t get PPE. You run into problems with people’s personal ethics. People can’t face being the reason someone else dies. Dentists are horrified by the idea that they could infect someone, that their hyper-clean office could become a place where illness is spread.
Here in the UK we’re apparently setting up pop up morgues in “discreet” locations to avoid freaking people out. Because you know what freaks people out? Digging a plague pit on the village green.
And so, in order to prevent that serious problem, we instead require that a lot more places have 100% of their workforce out. I think most businesses can adapt to a 10% shortfall better than they can a 100% shutdown.
The fear of mass death part is a better argument, I’ll grant you that. On the other hand, it’s possibly an argument for government censorship and disinformation.
@AlexSpark
Except not. There are currently 5600 (known) cases and 43 deaths in New York City, population ~8 million. Initial infections were definitely more than a week ago. First case was confirmed March 1 (infected person came to NYC on February 25), first case we know resulted in spread confirmed March 3rd.
Right, but it’ll go from 25% of the pond to 100% in like a week. A trickle and then a flood. For all intents and purposes, a town can go from a small number of cases to basically everyone infected in 1-2 weeks.
And new york is much bigger than hypothetical small town, where a single family with kids in elementary, middle and high school could expose every single child in the town.
Some things will be absolutely killed by a 10% rate. The new york air traffic control system is having some problems right now I believe. There are other problems too, like how even if there aren’t restrictions, people know that eg. going to the cinema risks infection, so the cinemas die regardless of whether they’re actually closed. The advantage of the government ordering stuff closed is that conventions and things can claim insurance.
China didn’t think their censorship system could hush this up. That’s a sign that you probably can’t. They’re fiddling the edges, most likely, but you can’t actually hide a pandemic. It doesn’t matter how much you censor, people will notice if half the population of a care home drops dead inside a month. And you can’t ramp censorship from 0-60 in a couple of months.
AlexSpark,
New York Air Traffic Control was evacuated because someone tested positive for the virus. This is another example of one of those reactions that may have done more harm that good. It probably burnt an extra 500,000 lbs of jet fuel, for a start.
https://www.avweb.com/aviation-news/virus-scare-briefly-closes-new-york-artcc/
Except not. The absolute numbers for NYC belie that; NYC certainly had multiple points of infection (international travelers), but it hasn’t reached your predicted number of deaths in the time predicted. This isn’t smallpox or the Black Death; it isn’t even the Spanish Flu, though it may be the worst we’ve seen since then.
You keep misreading what I’m saying. It’s not from first infection to everyone, it’s from a relatively small number of cases to everyone being infected. Not to people being dead. There’s then a 2-3 week lag before people who are infected start actually dying.
And again, community size does matter in terms of how fast this happens. It’s going to take a bit longer for a city with millions of people to infect everyone. If you have a case in every church in a small town you could probably infect 60% of the population in a single day. That doesn’t start looking scary until you’re two weeks down the line and have over a thousand people in your tiny rural hospital with two ventilators. And at 60% infection rates and 2% fatality, that’s 120 deaths. Probably within a week or so of each other.
I am not misunderstanding what you are saying. I am saying your numbers do not work.
We’re already at that point in NYC. There aren’t 200 deaths. (Number of infections is essentially unknown, which is why I’ve been concentrating on deaths). You will not get from a “small number of cases” to 5000 in 2-3 weeks; with an infectious period of about 2 weeks and a “small number of cases” being about 10, that would imply an R0-value in the hundreds.
AlexSpark alluded to it, but the option isn’t “Business as usual,” it’s “Government does nothing.”
The government doing nothing is absolutely an option, but people will not carry on conducting business as usual if it turns out that was inadvisable. Right, wrong, or indifferent, people will freak if hospitals get slammed. If hospitals get slammed and there’s a pile of bodies, they will absolutely remember it in November. If the Chinese government–with a real authoritarian streak, a bunch of concentration camps, and a very active censorship regime–wasn’t willing to let a bunch of their citizens die of this, I don’t see any Western governments holding the line.
Most people just don’t think about hidden costs, even if they’re huge compared to the visible ones. After the Grenfell Tower fire, Megan McArdle wrote an article counseling against a knee-jerk reaction in rewriting building codes, reasoning that it’d be better to sit down with a calculator and figure out how much new requirements would increase building costs and whether the lives saved would be worth it. To this day, years later, she still has idiots following her around Twitter shrieking like squirrels in a blender. These people are totally incapable of considering things they can’t see.
I don’t disagree. And I do, in fact, believe this is what is driving most political action. Everyone is terrified as being seen as “not doing enough.” That said…
The costs of these actions are hidden for a very short time, but they won’t be for long. When you and half your friends are laid off during the panic, and struggle to find new work after the panic because now it’s a recession – you’ll remember that in November too.
Would voters punish “1% of the population dies” more or less than they’d punish “20% unemployment and stocks at 15-year lows”? I honestly don’t know the answer.
It shouldn’t be true, but inconveniencing people can be worse than killing people.
And hey, if I can get a little personal (and admittedly selfish) here for a bit…
I’ve been planning my wedding for months, and it will almost certainly have to be cancelled and re-scheduled. As far as I can tell, the object-level reason for this cancellation is NOT “because people are sick.” Because I’m not sick. My fiance isn’t sick. Our wedding party isn’t sick. Our families aren’t sick. Our vendors aren’t sick.
No, the reason my wedding will be canceled is because the governor signed an executive order requiring that it be canceled. So now, I get to listen to my fiance cry herself to sleep.
I won’t be forgetting that come November. I may forgive it, if it turns out the virus really was as bad as everyone thinks and these actions really did end up improving things a great deal.
But if that’s not the case, I will vote against my normal partisan affiliation to vote against every incumbent on the ballot.
And currently, she of all people is pounding the table for stimulus and defending social distancing. (paywall)
(I know the go-to explanation is “they must be placating the All-Powerful Left(tm)”, but I find it unlikely either that she would do so and/or pick now.)
What do you think Wuhan looks like today if the government took zero actions? What about no government action and little or no media coverage(the panic is the real problem)?
How the hell do you know? Did you get tested? Do you know how common asymptomatic (but still contagious) cases are, especially among young people? Do you think that the mess we got in Italy was only spread by people who knew they were sick?
@Spookykou
Wuhan? Who can tell? Given that China has lied all along, we can’t even tell what Wuhan is like now. No new infections strikes me as implausible, at the least.
I would if they’d allow me to, but they won’t, because I’m asymptomatic.
By the time the date of the wedding is here, I’ll have been effectively “social distancing” for over 3 weeks. If we’re all still not sick by then, we’re almost certainly not sick.
Hold on a second, you were advocating “business as usual”. You can’t claim any benefits from distancing if your plan is to carry on as usual.
So this wedding, where the most elderly of your extended family will be, will very likely include someone who is infectious
So, in the hypothetical where you knew somebody in the wedding would be infectious (but you don’t know who is infectious), do you actually want all of the elderly in both your families exposed at this event?
I would do my best to explain the risks to everyone the best I could, and allow them to make their own decisions (possibly including a very direct “If I were you, I wouldn’t come” sort of statement).
And encourage proper social distancing at the wedding itself (eliminate the dance floor, keep pictures very limited, etc.)
In any case, I was advocating “business as usual” in terms of the government. I myself had began working from home, dramatically increased my hygiene regimen, stocked up on goods, increased social distancing, etc. at least a week ahead of when the state started mandating we do so…
IOW, you really do think it’s a bad idea for people to be gathering in large groups with close contact.
Think about that. You think the optimal course of action really is social distancing, you just don’t want everyone engaging in the optimal course of action. You’d prefer it if other people engaged in less optimal courses of action.
Or, you really do want everyone to change their behavior, you just object to the mandate. If so, then your initial complaint about the economic impacts rings hollow.
I also highly doubt you are thinking through how you could accomplish a wedding with everyone engaging in physical distancing.
Yes. There are lots of things that happen in society that I think are bad ideas. I think it’s a bad idea for people to smoke cigarettes, for example. That doesn’t mean that I want the government to imprison everyone who does so, or even that I won’t be friends with or associate with people who do so.
This is incredibly rude of you. “How can I still give my fiance something that even comes close to approximating the wedding she’s dreamed about without providing an undue risk to the lives and health of our families” has been one of the primary thoughts racing through my head, preventing me from sleeping or accomplishing much, for the past three weeks.
But feel free to accuse me of having “not thought about it.”
“optimal” depends on costs, not just benefits. Tech workers are almost perfectly suited to semi-permanent work from home, the costs are minimal, so they do so pretty much without prompting (I’m one of 2 people still showing up in an office of previously ~45 people, in Ontario where there’s no mandate to work from home, and that started before the government shut down dine-in restaurants).
A mandate eliminates the ability for people to determine for themselves whether costs exceed benefits.
Matt M’s tradeoff seems to be “willing to stay indoors and away from people, except for his wedding”. That doesn’t seem crazy to me.
You can make a standard “externality” argument, but even then the better policy is a tax (we already have max-occupancy for buildings, so maybe a tax that scales with % of that?), instead of blanket bans with pull-aristocracy exemptions.
In general, it’s not fair to use someone’s prior pro-social behavior to prove that changing from that behavior is bad. Maybe new information came out, maybe they were banking up good karma because they knew something else was coming later, maybe they are trying to keep another person happy.
We don’t need a new tax, we already have negligence law. Just let everyone who gets sick or dies where Matt M’s wedding is a cause (in strict liability under the ultra hazardous activities doctrine) sue him in tort. Then as long as he has adequate insurance to cover 95th percentile damages, by all means let the event go forward.
1. Assumption of risk.
2. Attending the wedding is unlikely to produce more than a 1% chance of death even for elderly guests, which I don’t think makes it an ultrahazardous activity.
Also I’m reasonably confident that my grandmother isn’t going to sue me for allowing her to attend my wedding. Even if she gets sick later.
First of all, it sucks that your wedding plans need to be altered. Such are the vicissitudes of life, but that doesn’t lessen the sting.
My wife is nurse practitioner in private practice. She is almost assuredly going to get pulled into the hospital to provide care as the system becomes overloaded. That’s just life, but it doesn’t make me worry less about her health and the health of my family.
However, you are admitting this is not dead simple. Changes do need to be made. The risks and costs of inaction are very real. This is not “business as usual”. Given your extreme distress and trying to figure out how one could possibly make this work, your claim that you wish that things should be “business as usual” do not make sense. Business will not precede as usual in a time of pandemic, regardless of the actions of government.
Tragedy of the commons is very real, and applies here. Yes, your event can happen without undue risk to all others, but everyone’s cannot. From a libertarian perspective, you might like it, perhaps, if that commons did not exist, but it does.
Complicating the analysis: if it works, it will look like we overreacted.
Sometimes you see people opining “why was Y2K such a big deal – nothing melted down” (you probably wouldn’t see that here, because many of us were *there*, and know better).
But I’m pretty sure we’re going to have widespread bailouts – even Republicans seem sort of OK with it. I think this is a combination of lessons we’ve learned from the last recession, and the nature of this one – in past downturns it was always possible to (usually motivatedly) reason oneself into thinking that peoples’ financial problems were due to their own moral failings. It’s just too hard to do that this time.
*sigh* I hope it’s too hard for for people to convince themselves this time that other people’s problems – and for that matter, other people’s deaths – were due to their own moral failings.
But I can make the argument for “moral failings” myself, though completely tongue in cheek. It’s easier if I presume something like the Propserity Gospel, where the flip side of “God wants you to be rich” easily becomes “so if you are poor, it’s because you’ve been behaving sinfully”. But many fervent right wing supporters of capitalism routinely talk about having money as a sign of virtue, without religious justification. Having an office job, especially in STEM, seems to “prove” one buckled down and worked hard, got a degree etc. – unlike those other people who are poor because they didn’t get a degree, or got a useless one.
So the “reason” I have a month’s supply of food, a 6+ month emergency fund, am still working, with good medical coverage, and am working from home (= lots less risk of C19)- is, to them, virtue rather than luck. (Some will allow a bit of luck too, but usually in the form of bad luck, happening to someone who would be where I am, except for some bad thing happening that they didn’t deserve.)
Some poor sod who loses his job, and then his home as a result of the economic downturn – after first bringing C19 home to their family, from trying to work their low paid face-to-face job as long as possible, and losing family members to it – is far too likely to become, in the public mind, yet another one of those nasty homeless people infesting their nice clean city.
[Edit: and if the poor guy climbs into a bottle in response to despair, that proves he ‘deserves’ to be yet another bum, whereas if I do the same, with far less reason, my health insurance sends me to a nice comfortable detox unit, and my disability insurance continues to pay me enough to keep my house etc.]
It’s harder for me to simulate/parody the same pattern on the other side of the political aisle, but there are humans on both sides, so I’m sure there is one – I’m just too human to see it clearly.
I really hope I’m wrong. Just for once, it would be nice to see people actually caring about the unfortunate, and understanding “there but for the grace of God go I”. But I’m far too cynical to expect it. I fear that if there are bailouts, they will be partisanly motivated attempts to help the politician’s base, not those who are worst affected or most in need.
Are you genuinely assuming that the layoffs and economic downturn are the results of the lockdown and not, you know, the deadly epidemic we’re currently at the beginning of?
Yes. The “deadly epidemic” has infected 20,000 and killed 275 people in the US. The direct effects aren’t nearly enough to cause the layoffs and economic downturn.
Exponential growth is a harsh mistress. It could be that the downturn is caused by other people being better at predicting the future than you.
But that cuts both ways. They could be predicting the consequences of the illness, or the consequences of the lockdowns (including predicting the consequences of lockdowns that hadn’t even been announced yet).
To tease the two apart you’d need to look at financial instruments that are conditional on the presence/absence of specific responses.
By invoking (then) present numbers, are you suggesting that policy should be based on them instead of the overall outcome as estimated by epidemiological models?
Likewise, are you expecting individual actors aware of the aforementioned impeding outcome not to change their behavior even in absence of government policy? Or are you supporting the notion, expressed above in the thread, that they should be actively misinformed in the name of economic measures?
No. I am, as I said, pointing out that the direct effects of the epidemic are currently far too small to explain the layoffs and downturn.
Indeed, a lot of them wouldn’t. Particularly if it means being laid off, losing one’s business, or having to lay people off. People are already chafing at the restrictions.
As for the overall outcome, there clearly isn’t enough data to even put in to the models (that is, we don’t even have good estimates of R0), and too many people are the simplest SIR model which assumes thorough mixing of the population, plugging in R0 estimates from whatever source they find, and predicting doom.
How are the current effects alone meaningful in explaining business decisions? Should they not be based on plans for and forecasts of the future?
And obviously people will be compelled to continue working despite the danger when the alternative is financial ruin and all the dangers that it, in turn, implies. (I consider this a bug of the system. I assume you consider it a feature.) I was not referring to them, though, I was referring to patrons. They have all the same reasons to stay away with essentially none of the downside, and even a fraction of them doing so will result in all the same businesses going under. So, to repeat the question you didn’t answer, should they be actively misinformed in the name of economic measures?
Finally, incompleteness of data is not an argument against using them to model the future, and not an argument against acting on them. It just means the results have a bigger margin of error. Note that it’s bigger in either direction – the less we know, the worse is the worst we must prepare for.
What plans and forecasts for the future would tell businesses (other than the travel industry) to start laying people off now? The way businesses are acting makes sense as a reaction to the lockdown; it does not make sense as a reaction to predictions of the future of the epidemic itself.
If you’re a restaurant not yet seeing a slowdown, but you estimate there’s a good chance you’ll see zero foot traffic for a couple of weeks, starting in ~two months, you might let people go now, and hope the money you save by then can let you pay rent/other fixed expenses and survive through to the other side.
That only makes sense if firing people increases your short-term profitability, but that’s possible depending on their roles (if their role mostly increases long-term profitability, or they’re trainees who aren’t net positive until after a few months on the job).
The availability of business credit should dampen this, but it’s unclear what that’s looking like right now.
Hoopdawg,
I run a tourist operation in New Zealand. 10 days ago we were at about 70% of normal revenue, give or take. Then border restrictions were put in place with a requirement to self-isolate on arrival, and we dropped to about 30% of normal over a few days. Now the borders are closed to non-citizens/residents. We are now at 2% of our normal revenue. With no border restrictions and letting the virus burn out we would have a rough three months: with all these restrictions, it will likely be 6-18 months and then 5 years of recovery, which we would not make it through.
Every tour operator, restaurant, bar, cafe, is in the same boat. Landlords are losing their tenants as they scramble to get back to their countries of origin. People are getting laid off all over the place despite the 12-week wage subsidies. In three months, when those subsidies finish and there’s no end in sight to the restrictions, virtually every business here will close, and landlords will have their properties foreclosed. Things changed overnight around here once the border restrictions went in place.
When I and the people in my town here are making huge sacrifices to save people, it makes me angry to see people here saying that the virus itself would have caused as much economic damage when that is obviously not the case. The imperial study, for example, shows three months of pain for the ‘do nothing’ scenario, then back to life as usual. Doing lots, shows at least 6 months of heavy restrictions, then some heavy restrictions thereafter. The likely scenario is that we spend five years recovering from this.
I can already see the next populist talking points:
The coastal elites, “experts” and academics decided our course of action for us, which, for them, meant “work”-from-home stay-cations drinking fancy wine and craft beer and using their recreational marijuana. For those of us with real jobs, who deliver their meals and coffee, fly their airplanes, bag their groceries, drive them around, take care of them when they are sick, grow their food, and keep God’s country running by hook or by crook, all we got were mass lay-offs or unpaid triple shifts. And what thanks do we get? Eviction notices, pink slips and “we did you a favor.”
I’m appalled at how little bailout money has happened.
Giving people $1000 each should have been done 3 days ago. Would it be enough? No. We need a lot more after that. But it would help the marginal people teetering on the edge know that something more is coming.
@LesHapablap:
You were already down to 70% revenue with just a couple of isolated cases in your entire country, and people in the roughly-defined west (perhaps sans Italy) still largely unconcerned and unimaginative about the disease. You can figure out what would happen once the deaths started piling on.
Your populist take seems entirely correct, and it’s very possible the governments will fuck the recovery up in exactly this manner for exactly this reason. If they do, fuck them, they’ll deserve all the blame. But don’t blame them for the half-assed (compared to, e.g., China) measures they’ve undertaken that merely sped up what, with the epidemic left unchecked, was coming anyway.
Hoopdawg,
The 30% drop didn’t have anything to do with concern about the virus, more the border restrictions in China and elsewhere preventing people from going on holiday. Once the 14-day self-isolation requirement came in, and every country around the world calling their citizens back, and the airlines shutting down, no tourists are coming to NZ any more. 99% of our business is foreign tourists.
I’ll just leave this here:
https://fivethirtyeight.com/features/coronavirus-is-hitting-restaurants-hard-even-in-states-that-havent-shut-them-down/
I’m very willing to believe restaurants have been hit hard even without government mandates. But lots of places without statewide bans have had countywide restrictions enforced, so 538’s analysis is incomplete.
It really depends on what actor I am dealing with. If we are talking about a place like IL, where I live, the governor just issued a shelter in place order. He is also a fundamentally unserious person who was not worried about C19 until about a week ago, and was trying to facilitate travel of international students back to IL campuses through January and February. So its safe to assume his response is another unserious response caused by panic, not a genuine prediction of the problems a pandemic can cause.
I genuinely am not sure what the UK’s strategy is at the moment. All the press are saying the the government has reversed course and is no longer trying to flatten the curve but to stop it entirely. They point to the paper from Imperial that you’ve linked and that we’ve rapidly been introducing stricter measures.
However the government is still talking about flattening the curve in press conferences, and they’re saying that introducing increasingly strict measures as the growth rate increased was always the plan (which is true, they said so from the start). The measures came in mere days after they said “not yet”, but the growth rate has taken off too.
A third possibility is mass-testing-as-exit-strategy; we’re one of the top countries for tests (less good per capita) and are working had on new tests that can check for anti-bodies so that might now be the strategy.
Are there any organizations or nonprofits working on the problem of PPE shortage for healthcare workers?
I have some friends in healthcare who let me know about the shortages in filter masks leading to less than adequate protection for healthcare workers. I’m trying to find concrete ways to help with that issue.
TIL the Philadelphia Police have published a list of crimes they will no longer pursue in the interests of officer safety. Today I also learned the Police Commissioner of Philadelphia is named Commissioner Outlaw. Her first act as Commissioner was to change the rules so that she could wear black nail polish at work.
> How many real cases per official case?
There are two different numbers here. One is the point-in-time ratio Confirmed(t) / Actual(t) while the virus is spreading exponentially, which you want to use to e.g. forecast the timeline of the outbreak in your area. The other is the probability of getting tested and testing positive, conditional on being infected, which you need to calculate the infection fatality rate from the case fatality rate. The Science paper estimates this probability.
During exponential growth, the point in time ratio is higher than the conditional probability. There is a lag from infection to confirmation, so on a given day you’re confirming infections from ~7-14 days ago (seethis post for a good illustration). A rough approximation for the point in time ratio is 6 times the conditional probability (the factor is exp(r * d) where r is the daily growth rate and d is the average lag (I used 18% and 10 days). My best guess is that the (inverse) conditional probability is 6-10x (basically the 95% CI from the Science paper) and the point in time ratio is 30-60x.
I realized that in the second paragraph when I mention the point in time ratio and the conditional probability I meant the reciprocal of these, i.e. Actual(t)/Confirmed(t) and 1/Pr(test positive|infected).
One thing I haven’t seen mentioned is that our overcrowded jails and prisons must be absolutely ripe for the virus to spread. Committing any crime that sends you to jail could be a death sentence, and there is no real way to mitigate the risk. What happens when all hell breaks loose and half the inmates need medical care?
Public Defender Twitter has been screaming about this for over a month. Many prisons don’t even have soap.
Radley Balko has tales of prosecutors threatening people to plea bargain to avoid being put in jails where coronavirus will spread.
What are the problems with a plan to isolate old people and have, say, the under 50’s keep working(with masks and no touching). Specifically what I am looking for is, would a population of just 0-50 still overload the medical infrastructure, what is the rate of severe symptoms that would lead to death if not treated broken down by age group(I feel like I saw this somewhere but I can’t find it), If the system does get overloaded do we ever get substantial child deaths, or are we headed for Miri?
Silly speculation on a personal level, should I stay in China ( I have housing) or should I return to the US? The obvious answer to me is to stay put, but if things get WAY worse, I don’t want to be stuck in a mad max world where I don’t speak the language/can’t read signs or labels.
My guess is that we’ll transition to that plan pretty quickly, because it is way more feasible over the long-term. Many of them would go out anyway, but I think it’s their right to decide on that. A major issue would be that many older people live with younger family members, and if they return to work/school in a busy society, there’s a lot of risk, but I don’t think a long lockdown is sustainable. I don’t think child deaths would pile up, but if enough adults get sick, even under 50, it could be a problem. We probably have to wait for more data on this.
@Spookykou
China has the big advantage that they actually produce things.
China has the practicality and brute force to make a lot of things work. That’s a reason to stay put.
But China has the practicality and brute force to make a lot of things work by bringing down the hammer on you if some bureaucrat decides it’s best. That’s a reason to get out.
I will give a perspective of one older person. I am 72 next month and have “chronic congestive heart failure” which currently has little effect on my life. I think we are all taking this death thing too seriously. We are all going to die. I’m for letting people take care of themselves. We should just educate and then let everyone determine what is best for them. I will be more careful on social distancing; I will wash my hands more; and consider face masks when available. I do not think the world should stop for me. If I choose not to keep myself safe, it is my choice. Shutting down our lives over some one or two percent death risk is crazy. I figure my risk is over 10% of death. If they want to put me on a ventilator I will refuse because, AIU, only 20 or 30 percent are alive a year later anyway.
We will always be alive and never experience death. We will be alive at every moment of our existence so forget the future and live while you are alive..
It makes perfect sense that celebrities (and politicians) would be infected disproportionately — their job is basically to rub shoulders with people, and the disease is most concentrated in large urban areas with international exposure, which are exactly the kind of place we’d expect celebrities to hang out. When they’re not on their private islands, at least.
My experience with celebrities suggests this is not necessarily true. At least, their rate of exposure to other people tends to occupy two extremes. High exposure to random people when engaging in promotional activity, media tours etc. But when on private time (a family vacation, for example) they tend to be very good at avoiding contact with other people. They can be fiercely protective of their privacy and “me time.” Especially A-listers.
Politicians, of course, are a different story.
I’d like to know when things will return to normal, defined as “I can go out dancing”. The answer to that is – we don’t know yet. So the next level question is – when will we have a good idea of when things will return to normal?
Like I said above, the answer could very well be “never”; moderated by “never, unless you take certain precautions first”, by analogy with the AIDS epidemic.
This feels wrong to me. Things will get normal in stages over a year or two, maybe. But at some point, there will be treatments, and vaccines, and herd immunity. I think we’re unclear how exactly this compares with the Spanish Flu, but it’s in the ballpark. Dances were canceled for the Spanish Flu. But then for decades, people danced without too much concern. We will get back there. My guess is that dancing will be back with essentially the same precautions as always (e.g. probably wash your hands between dancing and eating) somewhere between 4 months and 2 years from now.
Yeah I really don’t get “never”. Vaccines and treatments will eventually exist, and if they don’t, well, herd immunity will protect the 99% the virus doesn’t kill.
Why will herd immunity protect us and why do we think there will be a vaccine? There are vaccines for non-human coronavirus strains, but there are no vaccines for human coronavirus strains, despite SARS and MERS being rather serious. Obviously we will try very hard, but some things are just not feasible.
Certain virus strains can reinfect some people even if they have already been exposed. The adaptive immune system is not a fool-proof system. Given that a 1-5% infection rate of this disease can severely burden a local healthcare system, we will have to remain vigilant.
Oh, and even if you fix THIS human coronavirus strains, we have had 3 different coronavirus strains leap to humans in the last 20 years, varying in intensity from “oh crap, that’s bad, we’re lucky this isn’t that infectious” to “holy hell, this is the worst thing since Hitler.” There is a huge coronavirus reservoir and various strains will continue to species-jump to humans. This is not a minor shut-down, this needs to be a major wake-up call that gets us to rethink how our institutions respond to pandemics and how we personally treat our cleanliness.
This is not a minor shut-down, this needs to be a major wake-up call
This is how we should always respond to diseases. “We don’t know how bad things are going to get, but this is our chance to test all our systems and find out what we’re doing wrong, because there is always another bug waiting somewhere.”
@A Definite Beta Guy, people were actively working on a SARS vaccine until it was mooted by the disease getting wiped out. They un-mothballed that work to get a head start on the nCOV vaccine.
“Why will herd immunity protect us and why do we think there will be a vaccine?”
If a contagion has an R0 of 2.5, then in a continuously mixing population, there is a steady state where 60% of people are immune, and the number of people who get the disease every year is 60% of the new non-immune population (which might be 60% of the number of births, or of a larger number, if, for instance, some fraction of the immune population loses immunity per year). Furthermore, the only other steady state is eradication, and every state converges to one of these two states.
A steady state where 6% of the population contracts the virus every year is not so bad – it’s worse than flu season, but we can still sort of live with it, especially since the distribution of infections in this steady state will be biased towards the young.
And if we take some precautions by changing habits around hand-washing and the like, we might reduce R0 from 2.5 to 2, and change the steady state from 60% immunity to 50% immunity, which reduces a steady state of 6% of the population per year to 5% of the population per year.
Canceling all dancing would only be needed if we had an extremely contagious disease or an extremely devastating one.
If you live in a competent place that eliminates the disease, you can go out dancing soon. For example, you can go dancing in China today (though not Wuhan), if you don’t have a fever (which they check at the door).
You can get a different view of the COVID-19 situation by analyzing it on the level of infected communities in addition to that of individuals. Simple models suggest that for COVID-19 to be eliminated, it is not necessary to impose measures such as those in China and South Korea all over the world at once, but rather only in areas with active spreading.
The sooner such measures are imposed, the shorter the duration they must remain in place. If infected areas (including areas that become infected/re-infected in the future) are quick enough to act, the number of actively infected areas (and thus the number of areas in which such measures are required) will exponentially decrease over time.
See my working paper https://tinyurl.com/woesfdx for details.
On a side note, I am of the opinion that the Seattle outbreak demonstrates once and for all that China was on the ball.
The first case (nobody knew SARS-2 existed back then) has been traced by some researchers (SCMP) to mid-November.
The docs in Wuhan picked up on SARS-2 at around Christmastime, 5-6 weeks later (that’s the whistleblower), in the middle of flu season (never easy to pick up a new bug in that overload). One week of local government ass-covering later (which also includes the time to write the reports, do the studies, nail down the details, etc.), the WHO had a full report.
The local government cost everyone at most one week of time, and probably less.
It took “until” Jan 14 for sequencing and confirmation that COVID-19 was human-to-human. Yes, before mid-Jan, a man would have bet 50-50 that it was a purely zoonotic illness. I’ve been following this more-or-less closely. On Jan 21, the first test kits rolled out, and by Jan 24, the Central Government was sure there were a thousand test+ve cases in Wuhan. They locked the whole city down, and the province soon after that, buying the world (I would guess) about four weeks of serious prep time. In the middle of the Chinese equivalent of the Christmas holiday season. Twenty-eight days from first warning to execute.
The Seattle outbreak spread undetected between mid-January and late February. Another 6-week gap between occult spread and detection by medical authorities, even with at least strategic warning that COVID-19 existed (some sources go so far as to declare that Jan 1 in Wuhan was March 1 in Seattle). After that, even with a clear understanding of the pathogen, the US government took another two weeks of foot dragging to implement a massive response, and is only now, approximately 2-3 weeks after the start of the outbreak in Seattle, looking like it’s getting its act together.
Neither the US response, nor the European response, despite strategic warning, prep time, and technical intelligence, was substantially faster or more effective than the Chinese one. While yes, a more competent provincial government might have bought a few days to a week… on the whole, the system worked as well as any other. The Koreans and Japanese, on the other hand, appear to have been very fast, and leveraged warning and test kits for all it was worth.
https://bedford.io/blog/ncov-cryptic-transmission/
Looking at the graph of trying to “tune” the number of cases, does it fail if the populace knows that you are doing? “Yes, go out and get infected now. . . . No, no, too fast!” All of a sudden your cases are moving too fast for you to keep up with and you’ve accidentally overshot.
There was a Twitter thread about the dangers of randos 3d printing medical equipment, because the randos haven’t taken the steps necessary to make sure their products are not bioreactive. I can’t find it now, though.
Found it!
https://twitter.com/rahaeli/status/1239442013025697793
Also found that guy’s Wiki page. Yeah, the bit of plastic may give off some fumes. No responsible manufacturer would include such in a medical product. But which is better… breathing a bit of plastic fumes, or not breathing at all? The latter is known to lead to death in an extremely high percentage of cases.
> I’m usually pretty harsh on Bay Area governments here. So I want to give credit where credit is due: they’ve reacted to the coronavirus epidemic with a level of swiftness and ferocity they usually reserve for attempts to build new housing.
Did you mean “ferocity they usually reserve for blocking attempts to build new housing” instead?
You’ve got the parallelism wrong here. He’s saying they rapidly react to attempts to build new housing (by blocking it).
It was a few hours later, and may be the only good thing that Twitter outrage mobs ever accomplished.
Question: Is it true that US hospitals are not using chloroquine to treat COVID-19? And if so, why? I mean, chloroquine may not be approved for COVID-19 here, but it is approved, so they should just be able to prescribe it off-label, right?
“Question: Is it true that US hospitals are not using chloroquine to treat COVID-19?”
Some are. Lots of intensivists the world over are throwing all kinds of shit at it. There’s no easy way to track at the moment and US hospitals are not a single entity.
Data so far suggests it might be useful as more of a prophylatic in the early stages. There’s some studies ongoing there. Could be useful or it might not be.
Huge supply issues already manifesting – was talking to a Rheumatologist yesterday who is worried some of his Lupus and RA patients aren’t going to be able to get any soon.
Addit to this: As I commented further up, the study that came out of France on this is very problematic.
It may still work as there is a plausible biological mechanism which might help in prophylaxis or very early in disease but IMO it’s unlikely it’s going to be an effective treatment for critical patients.
Hopefully we get some more randomised and blinded studies in critical patients soon because I suspect a lot of the early treatment data we get is going to be absolute rubbish, given people are throwing whatever they can find in the cupboard at this.
So as a side effect of the various lockdowns, social distancing, staying-at-home initiatives, we can see what it would take to get that climate change reduction.
CO2 and other emissions levels falling due to shutdowns in production and people not travelling around, stories linked here and here.
What do you think – is this a good example of how drastically economies would have to change in order to get the sort of change to avert or reduce global climate change?
Absolutely not. With smart decision making I estimate it would take 20% of this level of shutdown.
RE: masks – I felt bad because my wife and I each have a 2-pack, purchased back in late January when I was supposed to be going to China & South Korea. Then I see the article recommending to donate if you have in excess of 2 WEEK’S WORTH. I’m even bad at hoarding!
Hi, asking for a friend who is much more unfortunate than me and currently does not have health insurance.
I remember someone, perhaps a regular with a bluish avatar contributing in some… open thread? About how they were able to cut through a bunch of health insurance premiums in the states and get a comparatively reasonably priced experience. Parts of the advice I remember involve being frank with the billing department up front that you are not covered by insurance (even if you are) and being very insistent.
I’ve tried googling this, but in general I get around 10 SSC posts with 500< comments and most of the keywords in the body of the post rather than the comments. Even if you don't know the exact post, any meta search strategy help is appreciated.
this comment, via this search engine
Thank you so very much!
However things play out, it looks likely that the economic fallout from the pandemic will be bad enough that the resulting recession will need an Official Name, like the Great Depression or the Great Recession. If things get worse than 2008, then the Greater Recession would be an obvious candidate (or, god forbid, the Greater Depression). However, I would like to propose an alternative: “Great Recession 2: Economic Flugaloo.”
Edit: Okay, it is a hashtag now. Come on folks, let’s get this meme’s R0 up until it overtakes SARS-CoV-2 infections!
In case anyone doesn’t get the reference, it’s a snowclone based on the title of the movie “Breakin’ 2: Electric Boogaloo,” which I first heard of via a silly Family Guy gag many years ago, and have spotted in the wild a few times since.
How do we quantify if it’s a recession or a depression?
There’s no concrete definition. Recession is generally recognized as 2 consecutive quarters of negative GDP growth. Depression is just a “prolonged” recession, but there’s an ill-defined length of time, some as short as 18 months, others think it has to be 2+ years. Most recessions are so short the topic doesn’t really come up.
I would like to humbly propose “The Great Eclipse” because of the qabbalistic similarities between eclipses and coronas.
Been wondering about a lot of the same things—thank you for addressing these issues. Ioannidis’ remarks and the responses mostly seem to be kind of missing the point. He’s obviously right that our data is far from adequate in drawing solid conclusions about many things—the disease is new, countries are on different timelines, testing at different rates, and people aren’t diagnosed for some time after they are exposed. Is there any doubt the ratios are skewed right now? We can’t meaningfully assess the impact with any precision. But we’re also not going to get that data for some time, and the risks are high, so we are realistically going to have to take our best guess. We should of course acknowledge that we don’t know exactly how things will play out and are doing our best as we go along. He’s right it may not work. He’s right it could be a fiasco. He’s right there are serious costs to the shutdown, especially over the long term, that may not be worth it. This may be a mistake. We can’t ignore any of these things. But we simply aren’t going to have the particular data that would tell us that for some time. So we are going to need another basis for decision-making. That would seem to be the logical conclusion of his piece, but instead he acts like we can simply press pause, since we can’t at until we have “at minimum,” highly detailed data. Critics are making it sound like he advocated doing nothing, but that doesn’t seem to be the case–he seems to be avoiding reality altogether, and most of his critics are doing the same, like there are no logistical concerns about a two-year quarantine. They’re right data won’t save us–nothing will “save” us. But we will have to make decisions anyway.
At least some manufacturers of ventilators do ramp up production.
FYI your anonymous reader’s bus study was retracted: https://www.inkstonenews.com/health/medical-journal-retracts-study-how-far-coronavirus-can-spread-through-droplets/article/3074449
Although the South China Morning Post article, which at one point had a retraction notice, seems to have removed the notice (unless what I found was a different article.)
So I have no idea whether the authors of this study currently believe it’s accurate, and if not, why not.
It annoys me to no end that there is no reason given for the retraction. And you are absolutely right that the SCMP article used to have a retraction notice.
Your link sadly only lists the following criticism of the study: None of the people sitting immediately next to the index patient got sick. However, this was also the case in the well studied transmission of SARS on an airplane https://www.nejm.org/doi/full/10.1056/nejmoa031349, so this cannot count as conclusive proof that the study did not meet standards.
Robin Hanson addresses an important question: Can enough other countries around the world reproduce the success of China, South Korea, Taiwan, and Singapore in using testing, surveillance, and quarantines to stop the epidemic in its tracks, while permitting some reasonable continuation of economic activity? He is skeptical:
Do You Feel Lucky, Punk?
Um, no. China was primed and ready when the first case was detected late December.
After H1N1, they put in place a raft of measures to suppress such outbreaks and then, when any planned strategy failed, adapted quickly. That’s why WHO called them ‘nimble.’
Their response was probably the finest peacetime example of government competence in history, given its scale and speed.
When this is over, China will have the lowest Covid-19 death rate of any major country–and the world will notice.
Well, apart from the two or three weeks that local government covered up the outbreak anyway. At least once the government finally did act, they did so decisively and effectively.
Re: herd immunity.
The criticisms of the British plan of achieving herd immunity by letting the virus burn through the young population do not address one question:
For herd immunity to work, it seems necessary that the immune people are distributed randomly. But this is not the case here. Once the coocooning is lifted, a few of the elderly will catch it and then it will spread in their sub-population, because most of their contacts will in fact not be immune.
The ‘negative fifty thousand deaths’ idea seems…uh…kinda sociopathic? Is there anyone who actually thinks ‘this virus is actually a good thing because the economic damage it does causes reduced CO2 emissions?’ Even the author of the linked piece doesn’t endorse that – they say (emphasis mine):
If there are people who seriously endorse the idea that the coronavirus is a net good due to reduced emissions, I’m interested to hear what other similar views they have. Perhaps we ought to be grateful to banks for their role in causing the 2008 recession? I hear that led to reduced economic activity, with presumably a commensurate reduction in CO2 emissions.
I don’t think anyone pivots towards “this virus is a good thing.” The reduction in pollution – and subsequent lives saved – is just a fact. Sometimes it is helpful to let those factually true, but borderline-sociopathic, thoughts marinate in your brain and think about how they affect your world view.
For myself, it reminds me that “progress” across the globe comes at a cost (PM2.5 pollution) and maybe in less chaotic times, I should be more supportive of efforts to provide cleaner energy even if it involves state-sponsored meddling in markets.
The calculations don’t completely take into account the lives lost as a result of the economic impacts caused by those same quarantine actions.
There are plenty of confounders and areas of diminishing returns, but it’s not unreasonable that “as GDP per capita increases by 1%, predicted life expectancy increases by 5.737 years.”
It’s like stating abortions reduce the crime ration because of all the future criminals not born, without also accounting for all the inventors, etc… not born.
So some of the effect is real (working from home!), but others are likely very much net negative (reduced business activity across entire industries!).
The anti-ibuprofen recommendation has already been walked back by the WHO.
This article originally said avoid, now it says “updated – don’t avoid”.
Also, does anyone know why people aren’t talking about N95 respirator sterilization and reuse? I have found papers examining a variety of techniques including UV, Salt Water Supersaturation and Autoclave. I wrote a twitter thread with links to those papers. .
I’m seeing reports of hospitals manufacturing their own masks so it seems like sterilization ought to come before that. If that research looks good can we signal boost it?
My local hospital has developed a method for sterilising FFP2 masks (which I think are equivalent to N95?). Apparently after a certain number of times through the process the masks are deformed enough that fit is compromised.
Here’s a (probably) stupid question:
why not quarantine used masks in individual plastic bags for the 3-5 days the virus seems so survive on surfaces and then reuse? Nurses could have 7 respirators each labeled 1-7, for each day of the week, stored in a ziplock
Why would this not work, what am I missing?
The virus might die, but I imagine you’d get bacterial and mold growth on the mask, which you don’t want either. Literally fumigating the masks (with chlorine dioxide or hydrogen peroxide vapor) might work (if it didn’t destroy the mask), but I don’t know if hospitals have the equipment.
UV baths?
In the standard case you want to switch between each patient. Because you want to ensure that you don’t spread anything from one patient to another. Hospital-acquired infections are a disturbingly high source of mortality.
So does this mean Turchin was right?
WHO is ok with Ibuprofen again: https://twitter.com/WHO/status/1240409217997189128
Is stockpiling a positive-sum game if it’s done early (given that it drives up demand)? I mean I already did it so I am already an asshole if it isn’t, but if you tell me at least I will know for next time.
It certainly means you don’t have to participate in the crazy buying spree.
My house is slowly working through its stores, combined with infrequent shopping trips. We assume the markets (supermarkets, not stocks) will calm down pretty soon.
Last Friday night, I panicked when I went to the store as normal and saw huge crowds and many staples sold out. Then I went back on Saturday and almost everything was restocked and there was only a normal amount of customers. I haven’t been back since, since I’m still working my way through my supplies, but I am confident that stores will still mostly be in stock. I don’t know why everyone rushed the stores specifically last Friday though (my guess was the announcement of school closings).
I am intuitively in favor of Zeno’s stockpiling rule: feel free to stock up on staples you might be worried about needing, as long as you are taking no more than half of what’s now on the shelves. Taking more than half (including taking the last unit available) should be reserved for those who have a genuinely desperate and time-sensitive need. This gives plenty of room for prosocial demand signals to the stores but reduces the number of people genuinely deprived of that last container of wipes, TP etc you could have left them. I doubt this is optimal on any relevant metric but it “feels right” in a way I struggle to articulate.
In a world where we didn’t have this big social angst about surge pricing even in situations where the underlying item clearly has become more valuable, companies who make products that occasionally surge in value would stockpile them in giant warehouses somewhere where land and electricity are cheap. And then we would better ride out situations like this, where demand suddenly is far greater than production capacity.
Alas, we cannot have that, because people hate surge pricing (for reasons that, as an economist, I find unhelpful – preferences are like the Rocky Mountains, so they say, they just are – but better social norms are possible!). And thus, a company that does what I propose will only ever lose money, so they don’t do it.
Given all of that, is stock-piling pro-social? I think providing one isn’t extreme about it (i.e. buy a supply for a few weeks or a month, not 3 years), then yes. You are cutting down the number of times you will need to go to the shops, and grocery shopping is going to be one of the main limitations on successful social distancing in the weeks ahead. This is especially true if you do it weeks ahead (e.g. I did something like this 3 weeks ago, in anticipation) because you are providing an early signal to the stores/producers that demand is going to increase.
I also intuitively support salvorhardin’s “don’t take more than half, or the last of anything” rule. Of course, it fails if everyone else is just a jerk who takes it all in one go, but “is my utility from a marginal unit of this higher than the counterfactual person’s utility from their first unit of this” is a pretty good guide.
I’m very sure it’s a positive-sum game if done early; I even tend to be in favour done late (as long as you don’t buy out all of some life-saving item) because buying more = fewer trips, which is part of the whole social-distancing thing.
For some interesting stuff on ventilators and how to bodge them, see
https://panvent.blogspot.com/
The Pandemic Ventilator Project
This blog documents our attempt to construct a ventilator design for use in a Flu Pandemic that can be made from readily available materials at the last minute. Hopefully, the situation never arrives where this device will need to be used for a pandemic. But just in case… The Post below is the most recent. See the right side panel for other posts. This Blog was started on Feb 22, 2007
Needless to say, one of these could really hurt anyone it’s attached to. If trying it at home remember to mount a scratch monkey.
Ventilators and how to *what* them?? Remember to mount a *what*??
Please, please avoid the use of regional slang terms, especially now, given that the things you’re communicating seem to be important, and you’re talking to a diverse audience with different linguistic backgrounds and different levels of English mastery. Please use simple, common words. I have no idea what your comment says, and I’d like to know.
I looked it up, and “bodge” is something like “clumsy, inelegant mock-up of something” while “scratch monkey” is part of a hacker proverb–basically he’s saying “here’s how to make a makeshift ventilator, but be really careful using it.”
Since important people are trying to murder us, it is important to signal that we are not talking to important people.
They are?
Well, you are one of today’s 10000. And not the new coronavirus cases, the fun one where you first stumble across a reference that “everybody knows”.
The Scratch monkey story would be an internet meme today, except that it’s so old it predates the internet, supposedly having happened in 1979. It originally circulated as part of the Jargon file: http://catb.org/jargon/html/S/scratch-monkey.html is the canonical copy, though https://edp.org/monkey.htm is a little more complete (or embellished).
The reference basically means to be very sure you don’t actually have someone hooked up to your equipment while doing hardware troubleshooting.
On scratch monkeys, exactly. I suppose I have just grown old.
A version of the actual story is here: https://edp.org/monkey.htm
No idea how accurate it is.
I thought “bodge” was a fairly standard word — hack, jury rig, tweak, engage in bricolage.
By the way, if you like pictures, there is an instructable:
https://www.instructables.com/id/The-Pandemic-Ventilator/
“Bodge” I think is UK English only.
I had not only never heard the scratch monkey story, I didn’t know what a scratch space was.
Bodge is interesting because (as different dictionaries will tell you, usually only picking one nuance) it can either have the nuance “mess up ” or “do a poor but serviceable, for now, job”. I think the nuance of the two is completely different – one hints at failure, one at a qualified success. I didn’t know about the “create/repair poorly” definition, only the “mess up” definition, so I read the original message as being about ways you could make some fatal error creating masks, rather than making poor-quality ones.
@zakamutt, the article did not discuss masks, which fail in a relatively safe way, but mechanical ventilators, which if actualy tested, could easily kill someone who might otherwise live. I suspect the legal consequences could be almost as dire.
I did not want to put to glossy a spin on this activity, hence “bodge”.
Why is Africa so unaffected? 17 deaths in all of Africa as of today? What’s going on?
Optimistically, perhaps the hot climate in Africa is preventing the spread of the virus.
Pessimistically, perhaps there are so many daily deaths in Africa, and/or the state of medical testing is so poor, that the coronavirus is simply going unnoticed.
Maybe the susceptible people died young.
Shoot from the hip guess: less integrated/globalized -> fewer opportunities for the virus to enter local populations.
Razib Khan has put up some relevant posts recently:
COVID-19 And Its Weather Dependency
Blood Group A At Greater Risk From COVID-19 (Maybe) (Maybe regional variation in prevalence of different blood types plays a role?)
COVID-19 And The SARS-CoV-2 Pandemic, How Bad Will It Get?
Interesting tidbit from the third link:
Anecdotally I’ve seen the proposition that population density and “way of life” can explain a lot of the numbers. China, Italy, NYC in the states…very dense, lots of public transportation. Still very low case load in lower density areas.
But maybe I just want to believe this seeing as I live in the suburbs?
The outlier of this theory is India. 1,200+ people per square mile and currently sitting at 200 cases.
This seems very likely true. Think about situations by how many people they come in contact with, and how many hard surfaces they touch in common (where they could be spreading germs). An open plan office has nothing on a crowded subway carriage. This would predict that the US would be hit less hard / less rapidly than Europe. And it would predict that NYC would be more vulnerable / allow more rapid spread than the rest of the US. That’s two pretty clean predictions that are looking pretty accurate at the moment.
Unfortunately, I think the answer to that is that it just hasn’t really reached us yet. We’re up to 240 in South Africa now, and up to a few days ago all the cases were people who’d returned from holidays, mostly in Europe, or their close contacts. Other, less wealthy, sub-Saharan African countries have fewer citizens taking skiing holidays in Italy and have correspondingly fewer cases, but I have a horrible idea that’s going to change soon. I really hope I’m wrong and there is some kind of climatic or even genetic protective factor, but I think it’s simply that it’s taken longest to reach us because of fewer flights and returning tourists.
Early news reports I saw said lots of African countries knew they couldn’t cope and worked really hard on screening to keep it out.
That may not end up working but it may buy them time.
It’s surprising to me that I haven’t heard anybody talking about how good this lockdown is for the environment. Air quality is way up, traffic is way down. Working to sustain the work from home culture after the virus threat ends is probably the best chance in a generation to reduce co2 emissions.
It’s briefly mentioned in this post when he talks about the negative net deaths (counting lives saved from air pollution)
I’ve seen people talk about this, including clear canals in Venice.
https://www.housebeautiful.com/lifestyle/a31705362/venice-clean-water-coronavirus/
Fish! Swans!
The swans are a lie. And the dolphins. And possibly the fish.
The canals are somewhat cleaner, though.
https://www.nationalgeographic.com/animals/2020/03/coronavirus-pandemic-fake-animal-viral-social-media-posts/?fbclid=IwAR3M4ztCLZDgfTKzUzmN2fp_R3mPXojrgnV-REAaE3Xici_YxwYE1uLsjHY
Hey, stupid question:
Is there a website that allows regular people to write up a bet and make it?
I’ve gotten into arguments with a number of internet blowhards, and I’d like to be able to challenge them to put their money where their mouth is on certain things.
Sites like Metaculus and LongBets are kind of in the neighborhood, but not exactly what I’m looking for.
Any suggestions?
Maybe PredictionBook? Its main usecase is for logging individual predictions, but it’s freeform enough that it could probably be used for this. FYI, the reason there aren’t better betting sites is basically that gambling is illegal; I don’t know a ton of detail, but just from talking to friends who work in this space, regulatory issues are a major blocker. Hope that helps!!
Two of the most important questions right now seem to be:
1/ how much test capacity / trailing daily diagnoses do we need to start easing lockdown?
2/ how fast are we ramping up testing capacity? Best data I’ve seen thus far shows 7k to 75k in a week (source)
I am optimistic lock down will only last about 4 weeks (the sooner we start the sooner we can end) followed by another 6-8+ weeks of extensive testing, depending on how outbreaks in other countries are developing. Italy is almost 2 weeks into their lockdown and daily cases haven’t subsided yet, so this may lean optimistic.
Honorary third is perhaps 3/ when will a serological test confirming immunity be released? If we could mark citizens as immune, we could greatly increase our speed of social/economic recovery.
Here’s Politico’s page which pulls from those covidtracking.com testing numbers, but plots them on a graph and breaks them down visually by state: https://www.politico.com/interactives/2020/coronavirus-testing-by-state-chart-of-new-cases/
thanks!
I share your optimism about how quickly testing is ramping.
The site you mentioned, also here for some details is obviously a non-trivial undercount, because it has issues getting negatives from a bunch of states regularly or at all. And even when states are good at reporting data, they themselves may not have good data on the number of tests done by private labs. And trying to get “tests per day” from their time series is a bit hindered by the fact that a lot of the updating from states is lumpy – e.g. CA didn’t update negatives for multiple days, and then gave a one off update. It’s still useful as a lower bound.
An alternate estimate is here, which relies on statistical adjustment of the data provided by the CDC. If private labs continue to ramp more rapidly than public labs (which had approval from the CDC / FDA to operate sooner), this will probably also give an underestimate. And as a “statistical” method – it should be able to pick up negatives better, but it comes with various other caveats. It gives a somewhat higher number, which is sort of reassuring that two very different methods can give not super different answers.
Either way, it looks like testing is ramping rapidly.
Writing from six days in the future – Italy’s new cases stopped increasing a few days ago, so something like 14-17 days from heavy lockdown to a cap in the growth of detected cases.
Has anyone else actually read the “ravenous wild monkeys” link?
Was it translated by a human? I expect machine translation to be better than that.
Nice catch. It looks like the text is copied from other sources and then manually reworded using synonyms:
“hundreds of hungry monkeys fighting one another over a single banana” (Source) becomes
“HUNDREDS of monkeys in Thailand had been noticed combating over a unmarried banana”
“They looked more like wild dogs than monkeys” (Source) becomes
“They seemed extra like wild canines than monkeys”
(Note that my links don’t necessarily go to the first/original source, but at least to an early source with better wording.)
Why manual? It may just be a bot that translates a lot of articles for the ad revenue.
Good point, I shouldn’t have said manual. I meant blindly/clunkily, don’t know why “manual” came to mind.
My point was that I don’t think it is a result of Thai -> English translation, but instead English -> English “translation” (rewording). But you’re right that it’s very possibly, perhaps even likely, automated.
The reason I don’t think it is Thai -> English is that there doesn’t seem to be a Thai word that means both “unmarried” and “single” (in the sense of sole/one, e.g. “a single banana”).
Other possibilities are English -> other language -> English, or Thai -> other language -> English, or just Other language -> English. But any of these possibilities absolutely could be automated.
Aren’t some drugs used in psychiatry anti-inflammatory?
We won’t have vaccines by September (probably, we just might) but we’ll definitely have drug cocktails that can dramatically increase survival rates.
We already have a recipe that’s probably quite effective and possibly even a cure, but we don’t have the supply chain worked out. (kaletra + tamiflu + plaquenil + remdesivir, with remdesivir not yet certified).
What’s your evidence for the “probably quite effective” claim? I’ve seen a bunch of stories that say that at least the individual components of that recipe either failed trials or haven’t been adequately tried yet. Is there better evidence for the whole combination working?
The French are saying plaquenil (hydroxychloroquine) is effective, but they would, since they make it:
https://www.connexionfrance.com/French-news/French-researcher-in-Marseille-posts-successful-Covid-19-coronavirus-drug-trial-results
Is someone else saying it doesn’t work?
It’s only Plaquenil if it comes from the Plaquenil region of France. Otherwise it’s just Sparkling Hydroxychloroquine.
I would be extremely leery of exiting antiviral ‘cures’ at this stage
For instance, from your post, Tamiflu absolutely does not work against coronaviruses. There’s even debate about whether it actually does anything clinically meaningful for influenza at this stage.
Lopinavir / Ritonavir has a couple of human trials saying it doesn’t work for nCov2. Probably more ongoing.
Remdesivir there’s no real good data yet in humans. We’ll probably get some out of China in the next couple of weeks. I think there’s a huge amount of problems with these early studies though.
Hydroxychloroquinine seems, this early, to be well supported as a prophylactic therapy. Less so as an actual acute treatment. Given the long incubation and asymptomatic early stages this is problematic but I think we can narrow down effective regiemes soon. There’s some prophylaxis trials already up in the US. It won’t be a good ‘cure’ IMO.
However one of the big issues with just smashing this virus with all your antivirals and seeing what sticks is the combined side effect profile. A significant number of the deaths from this virus are proposed to result from acute cardiomyopathy secondary to myocarditis. And you’re seeing a lot of really sick patients being those with underlying cardiac issues (ie a lot of the middle to older population of the developed world). A lot of the aforementioned antivirals have cardiac side effects and are pro-arrythmic. The extent to which this is problematic isn’t really yet known but it is likely there’s some issues there.
I’m going to add an additional comment here.
I’ve just managed to find and read the French hydroxychloroquinine study.
It’s (by necessity obviously) an open label, non-randomised study with an N of 20 for the experimental arm. The measured outcome is a proxy measure not survival and the methods are a bit off.
There’s a plausible biological mechanism for it in inhibiting viral fusion but that’s only going to help with early stage or prophylaxis (Like tamiflu, which again we’re not really sure if it works). But this is such amazingly tenuous evidence to be calling it a cure.
“As of today, the US has almost 10,000 official cases. How many real cases per official case?”
How many asymptomatic or mildly symptomatic who don’t seek medical attention for every case that does?
Per this link 50-75% asymptomatic in one Italian city. Via cvdailyupdates.com and I can’t vouch for the reliability of the source.
I’m pretty skeptical of this, as the numbers provided works out to a 3% positive rate in a sample of 3000. I can easily see a false positive rate being as high as 3%, explaining the apparently high rate of asymptomatic infections. Without frequent PCR testing or serological testing there’d be no way to distinguish a false positive followed by a true negative from a recovery.
Didn’t they get 0.3% positive on the retest? If the 3% were just false positives, they should have gotten 3% again on average.
Prisons and and virus. Another thing to keep track of.
The idea that it would take months to ramp up testing in the US to China/SK levels continues to boggle me. We have the WHO publicized protocols. We know labs in other countries have ramped up to hundreds of thousands (SK) or millions (CN) of tests in weeks. What on earth is going on that would keep us this slow here? Is it *still* regulatory barriers? If so, with all the emergency regulation-slashing going on around things like doctors practicing across state lines, why hasn’t the FDA already just said that any testing protocol already widely used in other advanced countries is ipso facto approved here? Or is there some material shortage, or some other substantive barrier?
Also curious, and wondering what do these tests look like?
Fortunately, testing is now ramping very rapidly. Which is why the number of detected cases in the US has also shot up in recent days. Here are two different approaches to measuring testing.
The first is basically just a manual count of tests from each of the states, summed together. Main problems – under-reporting of negatives, under-reporting from private labs (again should only affect negatives but particularly severely), big lumpy updates (e.g. CA didn’t update negatives for multiple days, and then gave a one off update) mess up the time series.
The second is an estimate based on various adjustments of the data that the CDC releases. But the CDC data is slow, and keeps being revised up over time, so they have to do various things to adjust for that (basically predict adjustments to today’s numbers based on how much yesterday’s (and prior) numbers were adjusted up by etc). So it requires more statistical guesswork, but should better capture negatives.
Whichever you trust more, it looks like the US is already getting to South Korea’s rate of testing (I think – without checking – it got to about 25k per day). Obviously still lower in per capita terms but expanding rapidly.
We debated the same topic with my wife recently, about situation in Slovakia. Our conclusion was that the local politicians can’t understand the difference between “a coronavirus test” (as a complete product, sold in a shop) and “coronavirus testing” (as a process that is done inside a lab).
An analogy to use with laypeople is as if someone looked into hypermarkets and counted all the pancake dough products, and concluded “this is the maximum number of pancakes our country can cook in short term”. Which completely ignores the possibility of people making their pancakes out of flour and eggs.
So the politicians are probably asking their advisors “how many tests we can buy”, the advisors go to some medical supermarkets or whatever, and report “there are N tests currently sold”. Which the politician interprets as “we can only test N people”.
Instead they should talk with researchers, who would be like “detect a presence of X? sounds like PCR to me. yeah, that’s what we do every day. oh, you mean an RNA virus? that is RT-PCR, and yes, it is a known thing too” and they could probably test an order of magnitude more samples in the lab. (They just don’t have the time and resources to make it into a supermarket product, and get through all the bureaucracy.)
Also, there is this nice trick that if the probability of some people being sick is really low, you can mix their samples together, and test the result for the presence of coronavirus. A negative outcome means that by doing 1 test you have tested 64 people to be negative. (More people than that, the samples get too diluted for this method to be reliable.) This allows you to test even more people.
Another problem is how often should we re-test people. Just because today you were tested negative, it doesn’t say anything about tomorrow… But the original problem of testing everyone once, I believe is doable.
It’s also important to understand exactly how lab testing works.
You don’t just look at a swab under a microscope – doing that at the resolution required to identify a virus by sight would take massive amounts of time, not to mention a truly prodigal talent (imagine a Where’s Waldo where Waldo is a single pixel of a very specific color and the canvas is on the order of 5000×5000 pixels of random 16-bit color noise). Photo recognition software still has trouble telling crosswalks from not-crosswalks, if current CAPTCHAs are any indication, so you can’t just stick it in a Waldo-finding machine either.
Instead, you mix the swab with very specific chemicals, which behave in a known way in the presence of the virus – pretty analogous to the classic pregnancy test (chemicals turn blue = pregnant).
“Tests” is shorthand for “testing kits”, each of which contains a certain amount of the various chemicals required to test for a particular virus. A simple-to-understand version is to imagine, say, three chemicals – if the first turns blue, the second fizzes, and the third turns clear, then you know it’s the virus you’re looking for, but only under this exact combination. In the case of covid, it’s specific chemicals that will glow under UV light in the presence of covid, but you need each of the chemicals, since by themselves some might either not glow, or glow in the presence of non-covid micro-organisms.
I guess a broader analogy would be 3D printers (lab testing machines) and the 3D printer filament (testing kits). You use the same machine to test for covid that you use for various other viruses, and once you have one your lab’s pretty much set in that regard – but you also need the specific kit, which is consumed in the process of running the test.
(Also – and this might be the same as what you were saying – a “kit” might contain enough of each chemical to run multiple tests, depending on manufacturer and the test in question – and, furthermore, the term itself may be used as shorthand. Adding one “MediCo® Testing Kit™” to your cart at Amazon-but-for-Hospitals might mean you can then run 100 tests, and then your hospital’s PR person might announce this as “we have secured 100 testing kits”. Really the only time you can be absolutely sure is if it’s in phrasing like “we have enough testing kits to test x people” – assuming someone else in the information chain wasn’t confused by Testing Kits / Tests)
I saw an article that said Italy is underreporting deaths, because they’re not testing fatalities at nursing homes. This is a concern I have here in the States. Given the limited availability of tests and our admin’s stated preference for skewing numbers downwards, what are the chances we’re going to bury a bunch of suspicious fatalities without testing them for COVID-19?
I have no idea on misreporting in general, but at least for the very specific misreporting of deaths in nursing homes, the first 20-something deaths in Washington state were all at the same nursing home, so… that’s a thing that we know…
Re Celebrities and politicians getting it, here’s an eyeball calculation to confirm the intuition:
Assume people are a randome graph with mostly-uniform degree, except for Celebrities, who are a subset with a significantly higher degree. A level-1 model would just give celebrities a higher R0 (since they know more people, each celebrity is likely to be infected/infect by more people). A more complicated model might have two R0 values – one for when the celebrities cell might first get infected from the general population (already higher than baseline R0), and then a second, even higher one for celebrities infecting each other.
Either way, the important thing is that the R0 is the base of the exponent, which means celebrities will get infected exponentially faster, rather than just linearly. This implies (a) it’s basically impossible to stop all celebrities and politicians from getting it, and much faster than the rest of us, and (b) we should emphasize quarantining them off from normal people – their cell is already lost, but their ability to infect the rest of us is still strong.
(It’s also indirect evidence that Coronachan is less deadly than might seem – presumably most of congress either already has it or will soon, and most of them aren’t obviously sick).
Writing now from six days in the future – it looks like at least Ben McAdams and Mario Diaz-Balart were likely already infected by the day you were writing, and Rand Paul may have been as well. I think it’s very likely that several more of them have it as I write. They all seem to be having a lot more symptoms now than they were a week ago. So I wouldn’t count out the virus yet in terms of its effects on Congress.
Regarding the “guidance against wearing masks”: I’ve opened a pull request for flattenthecurve.com here to remove their anti-mask section. If you have any input, please contribute to the conversation yourself if you have a GitHub account or in a thread here if you don’t.
The ventilator capacity thing appears to be false:
But it does appear from the article that the capacity itself doesn’t scale very high or necessarily very quickly.
Why are we not going all in on masks? This seems like the simplest and most practical step that we can take right now. We know that they work, contrary to what everyone was saying a few weeks ago. And even a homemade mask is 50-70% effective. I get that developing a vaccine or enough testing kits takes a long time, but it shouldn’t take that long to manufacture strips of cloths that we can wear over our faces.
Masks would have been great two weeks ago when everyone was going to work. And might still be good now for grocery store employees or others who cannot distance/isolate.
But for those of us who can, what good will they do?
Most people aren’t in total lockdown quarintine mode, so they’re still coming into contact with others. Hell, a lot of people are still going to work just like normal. And even if we all were in lockdown mode, there’s no way we can sustain that for a year until there’s a vaccine or testing kits everywhere. A mask lowers the spread rate whenever someone has to go outside.
I’m able to hole up pretty well, but I’m going to have to go out at least a little, and I’d rather have 60% protection than none.
More importantly, we can’t all do isolation forever. We’ll have to make tradeoffs between people going back to work and trying to control spread. We might make use of masks then.
(I reported this comment by accident, meant to reply)
I wonder if for most people, masks would be a risk compensation thing where they would feel safer going outside and doing things than without a mask. This additional risk might make masks a net negative for people who would otherwise stay at home. I know I felt safer riding the subway with a mask and might not have taken it if I didn’t have one. In hindsight it probably would have been better if I didn’t go at all.
Do not self medicate with Chloroquine. While it might be a good remedy, there is nothing conclusive yet, and its adverse effect are bad enough that some people were hospitalized because of it.
Can you provide a citation for that?
Unfortunately, it’s comment from French doctor on twitter, and I can’t find them again due to the ways tweeter is classified. The secondary effect are in wikipedia
Found it.
https://twitter.com/Le___Doc/status/1240606674966241280
Wikipedia has some of the possible side effects listed. My brother-in-law got the seizures, muscle damage, gastrointestinal unpleasantness, and one hell of a rash. No apparent permanent damage, thankfully, but it was pretty scary.
Isn’t this simple “privileging the hypothesis”? I personally don’t have a reason to single out Tom Hanks or Idris Elba out of all celebrities, or Iran’s vice-president out of all Iranian politicians (or perhaps even all foreign politicians). Why do we need a susceptibility factor for celebrities here?
Hanks and Elba are extremely famous. If only 1 in 3000 Americans are infected and infections are independent of each other and of fame, then the chance of at least 2 of the n most famous Americans being infected is 1-(2999/3000)^n-n/3000(2999/3000)^(n-1). You can choose your own n-venture here, but Elba and Hanks being in the n=100 most famous Americans seems easy to defend. Even for n=500 the probability is only about 1%. So something has to be explained.
I agree with the point, though Idris Elba isn’t american and primarily resides in the UK (not sure where he caught the disease), and Tom Hanks developed the disease while in australia (also not sure where he caught it). Which in some sense is trivia, but in another sense shows how atypical the exposure profile can be.
Yeah, you beat me to it. Tom Hanks was in Australia, Idris Elba is English and was “on location” when he tested positive, which suggests not US , and Kristofer Hivju lives in Norway, where he was when he tested positive.
the more interesting case is basketball players, who have all been tested, have a high positve rate but a low severity.
Low basketball severity is probably due to the players’ generally excellent physiques.
I’d guess (based on my extremely limited sports knowledge) that high-level players travel pretty often, too, which would put them at greater risk.
Idris Elba getting in your top 500 famous Americans is just what I need to recover from that top 100 British celebs list containing TWO Irishmen.
Why are we pretending that we don’t all realise that celebrities are incredibly well connected people who spend as many hours meeting, greeting, schmoozing, hob-nobbing, appearing, not to mention acting and performing, with and for a tremendous web of people as the average pleb does in his main leisure activity of sitting alone in front of a television out of coughing distance of anyone, all of which leaves them much more likely to contract an ambient virulent disease with an asymptomatic stage? Why?
Regarding Malaysia’s 900 cases, about two-thirds of those seem to be from a single cluster involving a religious group that held a four-day mass gathering in late February. Probably not the best place to look for the general behavior of the virus in warm, humid climates – but numbers going forward should be more relevant. Or numbers from other SE Asian nations.
I made my own model for estimating infections, and with the newest numbers I get 100,000 infected in the US. I posted estimates from 15 countries in the subreddit a couple of days ago:
https://www.reddit.com/r/slatestarcodex/comments/fkede9/corona_infection_estimates_for_15_countries/
Note that I estimated 7000 infected in the US (with a much simpler method) back when the official number of cases was only 175:
https://www.facebook.com/Aleksanderasd/posts/10163318638565525
If true, that’s pretty great news, since we have only ~150 deaths, which means this genuinely is only a modestly bad flu.
No, it means that you will have at least 1000 deaths over the next month, even if all spread stops today. Which it won’t. Most of the people who are infected and are going to die, haven’t died yet.
I think you are misunderstanding me. It means that the very high CFRs that we are observing in the West now are in fact far too high and getting a positive test is not nearly as bad as people may think once testing ramps up to full speed.
1000 deaths in the next month seems plausible to me for the US, to be clear.
Oh, yes my model assumes a mortality rate of about 1%. It’s pretty obvious that Italy’s apparently high CFR is an artifact of them only having identified a fraction of their total cases. There are probably more than 300,000 infected in Italy. Real mortality rate is probably lower than 1% most places.
@aleksanderpwnz
And modestly bad is probably understating it too much. 1% is still pretty serious, but it’s at the high end of the flu range. A bad flu season is at 0.21%.
@EchoChaos
I keep hearing this, but I can’t reconcile it with the situation on the ground. Do 500 Italians die every day from the flu? Are tens of thousands in the hospital with problems breathing? Do 20% of all 80-year olds die every year from the flu?
@aleksanderpwnz
Yeah, pretty much. Remember that tons of old people are dying all the time.
https://www.sciencedirect.com/science/article/pii/S1201971219303285
~25000 dead in the flu season (the number for 2016/17) comes out to about 140 a day by my calculations, assuming the flu season is 6 months.
This is worse than that, obviously. But it’s not an order of magnitude worse.
@EchoChaos: those are nation-wide figures, but the vast majority of COVID-19 cases so far are in Lombardy. The total daily death rate in the Bergamo province is up a factor of 8 from last year. And the situation in ICUs in hospitals around here is the worst it’s been since WW2.
Real mortality is probably significantly higher than 1%. It’s been 0.7% in South Korea, but most of the cases there are from a new church with mostly young members. So we can expect much higher mortality rates for countries where the cases are more even across ages.
@eric23
It’s still 1% on the Diamond Princess, and they probably had an older population than any country on the planet. (Of course, only 7 people are dead there, so the data is noisy.)
I’ve heard that studies based on South Korean data (as opposed to just dividing deaths with “confirmed cases”, which probably aren’t accurate even in SK) suggest mortality rates between 0.2% and 0.6%. I haven’t heard that the infected are much younger on average than the general population. Do you have any numbers?
@aleksanderpwnz: SK definitely has a disproportionate number of 20-somethings among their known infections. (Wikipedia has been pretty good on this stuff in my experience, and the age distribution on that page matches the other numbers I’ve seen; you can see similar numbers in graph form here.)
I haven’t checked the data on age distribution over time, but the church full of young people that accounts for most of these infections was the first big cluster, so I suspect that 20-somethings are even more disproportionately represented among infections that began early enough to have an outcome by now.
@melolontha
Thanks! That is a lot of 20-year olds.
But the percentage of cases of age +65 seems to be roughly similar to the general population; while children are strongly underrepresented. Of course, old people are more likely to be identified because they get sick; but that’s exactly the kind of sampling problem that led us to use SK data in the first place. Taken together, I still don’t see a good reason to believe the “real” mortality rate is higher than 1%, let alone “significantly higher”.
“Infected” != “Recovered”
Re: ventilation and public transit, this is actually something I’ve been reading up on for work. I have clients in travel and hospitality who are mortified by their prospects at the moment – mainly because airplane cabins, cruise ships, and trains are mostly just slightly reciculated petri dishes as is. Even on an airplane – where you are surrounded by fresh air in all directions – about 50% of the air you breathe in is generally passed through a centralized circulatory system. This means that in effect, you’re just breathing a diluted admixture of old air from throughout the cabin. Without adequate particulate filtering this can be a big issue in terms of pathogens. Covid is not thought to be fully airborne, so fortunately this actually isn’t as big an issue to this specific outbreak.
However, some are advising a long term change in paradigms for circulation in transportation. I wanted to highlight Qingyan Chen’s work here – he has been petitioning companies like Carnival to radically change their circulation systems, and it took the recent cruise ship quarantines for them to take him seriously. Some of his advice can be implemented right now at low cost – but what’s really cool are the more long-term paradigms he suggests. For airplanes, he has both devised and tested a system where each passenger has their own small circulation system in their seat. Rather than 50% new air 50% everyone else’s air, this changes the equation to 50% new air 50% your own old air (assuming you stay in your seat of course). The crazy thing is that this system is actually feasible – it’s just likely too costly to implement in the near future. Regardless it’s the direction a lot of people in travel and transit expect things to go, but few are willing to sink the time and money into to really advance it.
I’ve been hearing about hospitals and other places building UV sterilization into their air circulation systems; would it be feasible to integrate that into train and airplane systems as well?
I’ve heard that the current test can’t tell if you’ve been infected before and have now recovered. Since so many cases are mild or asymptomatic, (and re-infection appears to be uncommon), it would be important to know this, otherwise large numbers of people may think they are still susceptible when they are not.
Is this an important issue or not ?
No. If we’re getting to the point where more than a tiny percentage of the population has recovered and doesn’t know it, we’re already at being so widespread that we’ve got larger problems.
Swabs can only detect the virus so they come out negative once you’ve recovered, but blood tests can also detect antibodies. And my girlfriend (a doctor in a hospital in northern Italy) says there still are plenty of people who test negative to both.
Re: ibuprofen and aspirin – the association between antipyretics and poorer outcomes in infections has been observed in a variety of settings. The problem is protopathic bias (handy phrase I just learned), where the association of a symptomatic treatment and worse outcomes may be due to the confounding factor of a pre-established pathological process. It’s very hard to control for that kind of bias, since most of these studies are retrospective.
That said, antipyretics are largely used for patient comfort and there is little long-term physiological risk in withholding them for low- and medium-grade fevers.
To be clear, the claim is that anti-inflammatories are an issue, while other anti-pyretics such as tylenol are ok.
I read an Atlantic article about this issue yesterday that convinced me to skip the Tylenol/paracetamol/acetaminophen, as well as NSAIDs, if I develop a fever, on the theory that they might suppress my immune response and thus increase my risk of more severe symptoms.
Here’s the key passage:
Check the link for further links to primary sources. (Try opening it in a private window if you hit the paywall.)
My takeaway was that not treating the fever might make me less comfortable but would otherwise probably be harmless, whereas using Tylenol would have some nontrivial risk of harm.
Is there anything solid about to what extent diabetes is a risk factor compared to whether ill-controlled diabetes is a risk factor or more of a risk factor? Also, type 1 vs. type 2?
I have no idea, but I would hypoethesize that type 2 has worse outcomes based on the assumption that Type 2 is more often associated with obesity, which is more often associated with cardio and respiratory diseases.
The reason why I asked about anything solid– anything based on specific information on how people with COVID 19 have fared– is because I haven’t seen anything with that sort of detail. I can get uninformed speculation about fat people anywhere.
Has Bach responded to the claim his math is wrong? Interested in hearing if there is a refutation, or if he agrees
Well, I can respond: Bach’s conclusions (that we need to contain the virus, not just slow it a few months) are not sensitive to details like the use of a normal distribution or the choice of parameters. Also, Bach had already pointed out these shortcomings in the article itself, and it has now been updated with links to people who have done more careful analyses.
Why do the details not matter? Isnt it the entire point of his objection?
I’m not clear on your question.
Bach argues that drastic (a la Hubei) intervention is necessary to prevent the healthcare system from being overwhelmed. He supports this with some hasty back-of-the-envelope calculations.
The critique argues that some of the details of this hasty calculation are wrong (which is true, and was admitted by Bach). The critique does not suggest that the conclusion would change if those details were fixed.
I contend that the end conclusion — drastic intervention is necessary — is not sensitive to changing these details. I base my contention on my intuitive understanding of how the calculation was performed, but I don’t know how to communicate this intuition effectively. I realize this basis may not be satisfying, but Bach links to better, proper calculations for people who want that instead.
As far as I can tell, there is no disagreement between me, Bach, or the critique of Bach.
this is a terrible argument then. he gives details to an argument to a support a conclusion, and then says the details ate irrelevant to the conclusion?
my understanding was he was claiming flattening the curve wouldnt be effective enough, because the peak of a normal distribution does not fall enough in a reasonable time frame. If his math is wrong, and the peak does fall, I would think that invalidates his argument. (i dont know that his math is wrong, im just saying its pretty relevant to the rest of his argument if it is)
I’ll try to be more clear: Bach does a simple calculation using a Gaussian curve, and reaches some conclusion. The critique says that a slightly different curve would be more realistic. However, repeating the calculation with a slightly different curve — or even a hugely different curve — gives the same conclusion. So, the choice of *which* curve doesn’t matter for the conclusion that Bach reaches.
You can repeat Bach’s argument in a few lines with no curves at all. He estimates that in an uncontained epidemic 10.8m people in the US will need a ventilator for 4 weeks each. As the US has 170k ventilators, this is 4.9 years of the US’s full ventilator capacity. So either (1) most people who need a ventilator will not get one and die or (2) massive intervention will cause many fewer than 10.8m people to need a ventilator (i.e., the epidemic will be contained).
I hope it is obvious that tweaking Bach’s argument by adjusting the numbers a little or slightly shifting the exact curve used does not change the essential conclusion.
it sounds like you are saying the normal distribution he uses is a close enough approximation to a logistic distribution. that is all i was going for. so the objection that an exponential growth has a much smaller peak is not true?
Yes, a normal distribution is a close enough approximation to the true curve (which is unknown). I don’t know what you mean by exponential growth has a smaller peak, but I don’t think it pertains.
the peak is the whole argument. the ‘math is wrong’ argument was the logistic curve has a smaller peak and could stay under hospital capacity if flattened. but it sounds like that is incorrect, the peaks are about the same
I find nostalgebraists gaussian-is-not-exponential objection very strange. Of course they are different. Exponential models the early phase of growth while gaussian models the whole lifecycle of growth – plateauing – subsiding. Of course there is no reason why the curve would be exactly gaussian – it’s just a convenient example of a curve that goes up and then down. An exponential doesn’t look like that *at all* and that’s the point. Over the lifetime of an outbreak the number of active case *will not*, *can not* follow an exponential. Don’t believe me? Check out the graph from China – it starts out vaguely exponential but the entire curve much more resembles a gaussian.
And btw. a gaussian *can* be approximated by exponential and more importantly the graph of the number of cases *can* be approximated by a gaussian (even in the early explosive phase). Just look at the chinese active cases graph in log scale. It looks like a straight line at first but over a few weeks it’s starting to bend and resembles an inverted parabola more. You know what curve is an inverted parabola in log scale? That’s right e^{-x^2}.
i dont know how the normal distribution compares to the logistic distribution on. the metrics you mention, but these seem like anecdotal answers to a strictly mathematical question
Yes, of course the overall curve should look bell-shaped. My argument was specifically against the Gaussian, as opposed to a bell-shaped curve with exponential tails such as the PDF of the logistic distribution.
That is, it’s perfectly possible to have a curve which looks very much like e^x on its left side, looks very much like e^(-x) on its right side, and has a peak in the middle. This is what we want: exponential growth at first (it’s an epidemic) and a bell shape overall. The logistic distribution’s PDF is such a curve. So is the curve you get from any simple dynamic model of an epidemic, as seen for example in one of the various web demos that have popped up lately due to Covid-19.
But the Gaussian is (somewhat famously!) not such a curve. For more, read about thin-tailed and heavy-tailed distributions — this page is a decent short explanation.
Fair enough. I misunderstood your objection.
Still, my intuition was that asymptotic behaviour doesn’t matter and anything vaguely bell-shaped would lead to the same conclusion.
That’s not quite true. I understand that you can have a curve so thin-tailed, with a peak so high that it would make nonsense of the calculation (~0 cases 99% of the time and 100m cases 1% of the time). If Bach tried to map a stretch of gaussian from something like -50 to +50 to a 1 year period – that’s what would happen. I just glanced at the pictures and assumed that was not the case. I assumed he picked gaussian as a convenient example of ‘something vaguely bell shaped’ with the understanding that the exact details don’t matter. Perhaps he should have used a triangular curve or better yet a rectangle as the best case scenario.
I have no opinion about the overall conclusions of both posts.
why do the tails matter? isnt it just the peak that matters?
FWIW, I don’t think this is what that post argued. No one, including Bach, is imagining some special “flat curve” scenario that makes the growth non-exponential without actually stopping it. The “flat curve” scenarios are exponential too. What matters is how much each scenario exceeds hospital capacity, and for how long.
Bach contends, instead, that the gap between US hospital capacity and default “no flattening” projected peaks is vast, and that hospitals will still be vastly overloaded in any “flattening” scenario unless the flattening is unrealistically extreme.
As you noted in the OP (thanks!), I think his argument is wrong; see also my comment here, where I spell out more clearly a key point I unfortunately left implicit in my tumblr post.
OK, but you should explicitly retract your first two bullet points from your post, the only points that Scott understood. They are technically correct, ie, substantially false. They are dangerous and delusional.
Does bounded exponential growth give a logistic distribution? if so, is his math that wrong? i am seeing online they are good aproximations of one another
If R is around 1, that has its own characteristics. R=1.01 would keep growing in principle, but the growth would be very slow, and over a period of a year or so (over which time the value would likely change) would not differ all that much from R=0.99.
so…. yes? no?
Given how much we don’t know – does anyone have a good source for credible folks who are doing their best to track and update on these questions specifically as new data comes in:
1) How long is this going to last?
2) How many people are going to die?
I don’t know about (2), but isn’t the answer to (1) basically, “forever” ? Eventually, everyone who is especially vulnerable to COVID-19 will die (either of COVID-19, or just of regular old age), and the rest will develop herd immunity; however, the virus will still be present in the population, just like the flu.
This is an interesting point. Do current models take into account that many (not saying most or even large minority, but at least some) of the deaths would have happened in the next few months anyway, and certainly even more of the hospitalizations would have occurred anyway?
I’m not saying, of course, that we should do anything specific with this info or just let people die anyway.
I don’t want to downplay the seriousness of this at all, but I did register slight irony at one of the earlier death announcements out of Italy. It said the average age of death was 81, which is higher than most countries’ life expectancy (though not Italy’s, I don’t believe). Obviously we don’t want anyone dying earlier than they have to, but it’s still weird that an average age of death for *all* the deaths would be lower in a lot of places than the average age of death for COVID-19.
That’s what the Imperial College people are saying, but I don’t believe it because a) they don’t make any attempt at model validation, b) they make some crazy assumptions, and c) they are seemingly telling me that Singapore, Hong Kong, Taiwan, and indeed Mainland China can’t exist, so I’m not sure why I should believe them.
I think (c) is a bit too strong. Obviously countries can exist; but it’s possible that human society (at least, the technologically advanced kind) will be semi-permanently transformed by the coronavirus, in the same way as it’s been semi-permanently transformed by AIDS.
The Imperial College paper (pdf) doesn’t have a lot to say about Chinese/South-Korean style suppression, but does mention it. Indeed, they even discuss it in the Summary:
Later in the paper they imply that the US/UK probably have too many cases already for this approach to be viable:
Of course, but they never argue why we can’t keep up radical measures for long enough to get the case number down to a point where measures in this style can pick up the rest. Or rather, they get that for free by assuming that we start lock-downs only on April 20 (!). That’s just… hard to take seriously.
The paragraph you quoted also continues like this:
Yeah. Except their analysis just presumes that we are not in Korea. I’m not impressed.
Now, I do see reasons to be pessimistic here, namely the fact that Western governments’ ability to mount a Korean-style response even after two months of quarantines is doubtful. But that’s a different story altogether.
“I’ll break your legs if you insist on going out,
I’ll wreck your teeth if you challenge me”
God damn, China. That’s basically a rap battle line.
I have been sick for the past two weeks. I was talking to somebody, and they pointed out that the disease progression I described is a very strong match with a confirmed-positive, mild case that they were reading about the other day.
I’m not really interested in playing armchair medic here to ask if you all think I caught COVID or not. I’m more interested in asking: what do I do with this information? What actions do I take. Some questions:
1) Given the way that the US has gone with testing, and given that I have had very mild symptoms (that I have since recovered from), the chance of me getting tested is near-zero. Further, if I’ve already recovered, a swab test will run negative anyway, and I’d need an antibody test. Any idea how I would go about getting this? I don’t mind paying out of pocket, if I have to.
2) I have worried for almost two months now that this would be like the angel of death washing over our country, and I have prepared accordingly. However, if I actually caught COVID and recovered, then this dramatically reduces my estimate of the risk posed to me personally (as I am presumably immune to future infection, at least in the short term). Assuming that testing is unavailable to me for, say, the next month, how would I go about getting enough certainty that I am immune from further COVID infection?
3) Out of an abundance of pro-social caution, I’m going to assume this was COVID and self-quarantine accordingly. I have already infected one other person (I infected her before I started showing symptoms, I promise I’ve been responsible), and I don’t want to spread it if I had it. How long should I self-quarantine after recovering, before I am definitely not contagious anymore?
Did you notify everyone you were around in the week or two before getting sick?
Yes. Fortunately, because I have been paranoid about this disease since the end of January, I can count on one hand the number of people who I had been around.
Of those people, four did not get sick, and one did get sick. The day I got sick I didn’t really think much of it but by day 3 I was in full on panic mode and reached out to everyone, just in case. None of them took it seriously, as my symptoms didn’t really match.
A week later, as more information came out and it started to sound like mild cases did match my symptoms, I reached out _again_ to let everyone know that I believed I had caught COVID.
I am in a similar situation to you.I am betting on “no chance ever” for #1 and “can’t say” for #2 since we heard conflicting reports of people in China being reinfected.
#3 especially irritates me, because my instructions were to wait at least 3 days after the fever and cough passed. But what if I never had fever and cough?! So I am going to wait until I feel fine, just 100% great in every way, and then give it 3 days. Since I can work remotely, this isn’t a huge burden. But the lack of clear direction here is annoying.
> #3 especially irritates me, because my instructions were to wait at least 3 days after the fever and cough passed. But what if I never had fever and cough?! So I am going to wait until I feel fine, just 100% great in every way, and then give it 3 days.
On Sunday night I heard an interview with a confirmed-positive mild case in new york and he described my symptoms almost exactly.
So yesterday, I called my clinic’s COVID hotline and talked to a nurse. She told me “two weeks from the end of symptoms”, _just to be cautious_, although she was open about the fact that that was probably unnecessary and if I could, great, but if I couldn’t, not the end of the world.
One other thing she told me, so, all my symptoms are gone but I still have phlegm in my throat and occasionally (~1x/day) cough it up. She says that’s a normal lingering effect from illness, it does _not_ mean I am still sick, it might last for a month or two, but don’t worry about it. She said it does not mean I’m still contagious.
Interestingly, she took the reinfection rumours seriously, and told me that even if I had recovered from COVID, I should not assume that I’m immune. She said I _probably_ am, but there’s enough uncertainty around how this works that reinfection may be possible.
Re (1), she told me that she didn’t know when _or even if_ their clinic will ever get antibody tests. She agreed that there wasn’t much point to do a swab at this point, as it would likely read negative, but she also was frank and said look, we don’t have very many tests in Texas, you’re low priority, you probably couldn’t get one even if you needed it.
Did you lose your sense of smell?
Since your in lockdown, realistically what percentage of people are staying home instead of working outside the house? Obviously the staff of hospitals are needed, and they need electricity, I doubt that the power plants have access to public transportation so you need gas stations, and I doubt people have even three weeks of food stored so you need grocery stores, and you need the trucks to bring the food, and I’m guessing that the police are still out and about, and the ambulances, I would assume that the 911 call center equipment can’t be accessed remotely from home, and, and, and.
What percentage of the population can realistically be locked down?
Yes, I understand that people who have to leave the house should not go other places, just home and work, the question is to try and understand a bit better how effective a lockdown is compared to the other social distancing directives.
Phone companies estimate that every day in the past week around 40% of cellphones in Milan moved by more than 400 meters.
Nice. That’s better than I expected. I’m having trouble figuring out who exactly could be in lockdown without hindering the response other than waitstaff bartenders and movie theaters.
Thank you.
Stores that aren’t grocery stores – I’m pretty sure the mall is shut down, presumably the department stores are as well, and the hobby stores, and. I haven’t called my local plant nursery – I got everything I really needed, or substitutes for it, in a rush right before quarantine – but I would guess they are shut down. [Edit: Google thinks they aren’t, but it isn’t always accurate.] Churches. A lot of people who do white-collar jobs and can work from home. (In the Bay Area, “programmers” is a big group.)
I don’t know what normal people do for entertainment, but I don’t think it can be just movie theaters. Cirque du Soleil canceled its run; I’m pretty sure opera, plays, etc. will be doing so as well. All my hobbies have shut down – so the people who, whether professionally or as volunteers, would be running fifteen kinds of dancing or medieval tournaments or amateur choirs are staying home instead. The musicians who would be giving concerts or playing for dancing, aren’t.
I think grocery stores are a pretty small subset of stores, in general. And of course any restaurants that can’t do carry-out, are shut down.
I called one of the local nurseries a few days ago and they said they were still open.
I was shocked to discover that construction work is still ongoing at the big construction sites in my neighborhood. I assumed the shelter in place order would force them to pause work.
Update: It turns out that construction of housing, public works, and medical facilities is exempted under the order. So I guess that explains that.
What can USians most productively do to convince our federal and state governments to
— ramp up testing asap to at least the South Korean level, including testing for all symptomatic folks and substantial samples of the asymptomatic general population
— give us real data on how that rampup process is going?
Call our reps? Write actual on paper letters which of course by the time they arrive will be referring to terrible out of date info? Something else?
“Chronobiologist” sounds like an awesome title. Like you’re a time-traveling 12 Monkeys biologist who goes back in time to stop the pandemic before it starts.
Daring chronobiologist goes back in time to stop coronavirus, introduces dangerous future space bug to which 21st-century humans have no immunity.
Ha, we don’t know what the chronobiologist went back to stop when she introduced the Coronavirus.
Coronavirus, more like Chronoravirus amirite?
(Probably Aliens™ or something.)
It’s the much more dull job where you lock up people in a room for a week and open the door and the person is convinced it’s seven hours earlier because without external time indicators, he was cycling on a 25-hour day. (The average, actually.)
What’s the best available info on P(death | put on ventilator)? I’ve seen pretty high numbers thrown around, implying that while being put on a ventilator improves your chances of survival, in the event that you’re sick enough to need one you have a substantial chance of dying even if ventilated. Which, if true, limits the potential positive impact of increasing the ventilator supply.
I’d say you have to take into account how burnt out or overtaxed the staff is. Ventilators need to be constantly monitored and adjusted, along with their patients, to give them good odds. Some of the terrible odds we’re seeing are probably rooted in there not being enough man-hours to give each patient proper attention. It makes a big difference.
Fair. But if there’s no realistic way to get enough man-hours to make, say, 10x our current ventilator supply effective, that is also a limitation on the potential positive impact of having 10x as many ventilators, no?
Hard to say without knowing more than I do about ventilators; all I know is that I’m supposed to learn mechanical ventilation this summer and it’s supposed to be one of the hardest subjects in our program. However, the American Association of Respiratory Care does have a crash-course module in ventilator management to bust out when/if they unload their national stockpile (which isn’t all that big compared to the needs of this disaster).
This is me talking out my back end here, but it’s conceivable that you could cross-train a critical mass of other healthcare personnel in the most basic modes of vent management, some routine maintenance like suction, etc. and give them a list of things to watch out for, and let them get to work under an RT’s supervision. It’d be suboptimal, but perhaps better than having worn out RTs juggling forty vents in person.
But, again, IDK.
Although Malaysia might have a fairly high number of cases (900 at the time of writing) it sure does have a low death rate (0.2% – 2 deaths at the time of writing).
Cooler Japan has 924 cases and 29 deaths (3.1% death rate).
Could be that virus is much less severe in warm countries.
Also, California has 16 deaths to 870 confirmed cases (1.8% death rate) whilst cooler Washington state has 68 deaths to 1,187 cases (5.7% death rate).
Wouldn’t explain why Germany (averge temp March 0.3°C) has lower death rates than Spain (8°C) and Italy (8.7°C).
No, it does not explain that. But 8°C and 8.7°C is still pretty chilly compared to Malaysia’s 33°C.
For Chinese provinces with more than 200 cases there is pretty strong correlation between latitude and death rate (excludes Hubei):
link text
That’s not a particularly strong correlation. Also I think the northern provinces of China tend to be poorer.
Because they’re Germans? It’s pretty clear Italy dropped the ball, and as far as I can tell Spain also reacted pretty late.
Also, like TheMarch said, the effect may happen starting with higher temperatures.
One of many stories I could tell about life in Germany:
We have an obligatory meeting of research group with the fire safety official from central administration. After a long recital of useless information, we are given the opportunity for questions.
Head of research group: The ground floor exit below us is locked at and cannot be used after 18:00. If there is a fire after 18:00, and someone is still in the office, the only way to escape is by jumping ten or fifteen meters out the window.
Fire safety official: Hmm. Yes. That’s a problem. I’ll look into it.
We didn’t hear from him for the rest of the academic year, and fortunately I got a new job the following year.
But, well, at least you had a meeting with the safety official… Not sure how normal that is around the world. (here it most definitely isn’t, but we’re not a good yardstick)
Well, now I work at a university in Russia, where the bureaucracy is formally similar to that in Germany. Every time I sign a new contract, I have to go visit the fire safety office and listen to the same damned speech I listened to last time. The difference though is that the fire escapes in our buildings actually work.
Moral of this story: Germany has a good a reputation, Russia a bad reputation, and reality for both is somewhere in between.
Never been to Romania (?), so not entitled to an opinion, but if Romanians are anything like Russians, then they probably underestimate their country and overestimate other European countries.
@The Big Red Scary
Yep. I don’t know how they do it in universities here, but for small companies you basically have to pay a fire safety consultant and a security consultant, each makes a plan, fills out a bunch of paperwork and then always, just always, say: you need a fire extinguisher in each room and an alarm system. It’ll be insert outrageous amount for the advice.
Basically just a form of rent seeking.
> Moral of this story: Germany has a good a reputation, Russia a bad reputation, and reality for both is somewhere in between.
I take it you have not heard about the 2018 Kemerovo Fire. Or the Lame Horse fire.
Yes, Kemerovo was an enormous tragedy, compounded by criminal negligence, which my very weak claims (Germany is over-rated, Russia under-rated) take into account. Note that these weak claims are about a country compared to its reputation, not about one country compared to another, and were meant to illustrate a general point.
I will hazard one comparison between countries, however: Germany is low variance (uniformly not so bad) and Russia is high variance (pretty good in some places, such as Moscow, and pretty bad in others, such as in some less functional provinces). In particular, I expect Germany to handle the epidemic not particularly well, nor particularly poorly, and for the response to not vary so much from region to region, whereas I would expect some parts of Russia to handle the epidemic quite well, and others quite poorly.
Here’s a study of temperature and humidity on coronavirus survival on surfaces.
https://aem.asm.org/content/76/9/2712
Malaysia’s rise in cases is much more recent and currently has a doubling time of about 3.5 days. It takes a while for people to die. Expect a jump in deaths over the next week.
Japan, meanwhile, has always had a very slow growth rate, currently a doubling time of about a week. Hence, while they have the same number of diagnosed cases, they’ve been in this much longer – and therefore, people have had time to die.
Seattle is a known death rate outlier because one of the earliest mass infection sites was a nursing home. Just about the worst possible location in terms of death rates. Adjusted for age of those infected, it’s closer to everywhere else.
At this stage, temperature speculation is near useless.
You have to adjust for testing rates (and not only that, question is each countries testing process different and how that affects positive tests and recorded deaths). We’re early in the curve so comparing death rates, even adjusting for case numbers, is fraught. What’s the health system and hospital response like, is the triage different in each hospital/state/country? Are they reporting even?
We might be able to tease out a large scale effect in about 2 years or so. Not now.
I was under the impression that the market responds to demand for necessary goods more efficiently than the government. There’s a ton of demand out there for ventilators so this problem should solve itself shortly.
But that’s the question, right? Is there actually demand, or are hospitals not putting in purchase orders for ventilators yet?
Efficiently for individual actors, not for society at large. That’s one of the commons issues we still need a state for.
A factory may look at the current market and think thoughts like this: I need 6 months to build a new production line, at a very large cost – most likely on credit. If the pandemic resolves itself before I recoup my costs, I end up with debt and a market filled to the brim with ventilators because everybody ramped up production. It’s not an easy decision to make.
A government can say: “We’ll bear the risks ourselves, here’s the money for the production line. You don’ have to pay it back if you don’t end up making a profit. In exchange, don’t skin us with high prices if the market goes that way”. This way the company makes a hefty profit, no risk and ends up with a production line built. The profit is because they have the expertise to build a much needed product, and bearing the risk is the society’s cost for a very valuable service (many many lives saved).
In any case, medium term the ventilator market is pretty sure to crash.
Perhaps, but there may be external issues. What if the factories that make ventilators are already running at capacity?
Then the only option is to spin up additional factory lines to make more ventilators.
Building a factory is non-trivial in terms of cost, materials, and time, so there may very well be a lag.
The market can’t be much smarter than collective demand. Apparently for hospitals and medical supply distributors, buying *options* on mask production or other medical supplies ahead of time was not a thing?
According to one article [1], last time around, the one American mask maker nearly went bankrupt after demand abruptly stopped after SARS. The machines apparently have a four month lead time to install (though I imagine that has changed lately). Nobody thought about paying someone to install them and keep them mothballed?
My conclusion is that markets are much like every other human institution: they don’t work unless some smart people make them work.
[1] https://www.npr.org/sections/health-shots/2020/03/05/811387424/face-masks-not-enough-are-made-in-america-to-deal-with-coronavirus
Where is Hoover when we need him?
I have been waiting for someone to actually post it. 🙂
It seems like markets aren’t that great for addressing urgent crises and disasters, right?
Like markets are good at dealing with demand over time, but in a situation where hospitals don’t have extra cash to buy technology that will only be needed in a hundred-year-flood kind of situation, I can’t envision how market forces work there.
Like if the people standing on their rooftops during Hurricane Katrina needed to wait on the market to make them extra life rafts, they’d be in trouble.
I’ve been watching things here with an eye on how the market is doing. So far it seems the timeline look like this:
– short term speculators do small stuff like buying masks cheap and sell them high
– government does useful stuff – much faster than the market.
– bigger players have a few weeks of delay – not sure if that’s because they wait a bit before committing resources, or because what they do takes some time to get running. But when they start, they Get Shit Done. Here a cosmetics company announced it’s starting to produce hand gel, many textile companies are making masks and a private hospital started offering coronavirus tests at about $80. Not sure if that’s a coincidence or not, but the day after they did this the numbers of “tests done” doubled.
Yeah, I was thinking a similar thing about insurance companies. Insurance companies are great for spreading risk when you can’t afford the consequences of something going wrong but they can. But as soon as large numbers of people want to claim at the same time, insurance companies are useless.
Or even food. Free choice of whatever you want in the supermarket works really well in normal times, when any one person deciding to buy a weirdly large amount of something doesn’t have much impact, but as soon as a large number of people start buying a bit more than they need it’s queues, stampedes, and empty shelves. I’m not saying we need to see rationing, but rationing wouldn’t have this problem.
Insurance companies can handle large numbers of people making claims at the same time, through re-insurance (which allows them to break up correlated risks). They can’t handle a literal global pandemic, because there’s nowhere to spread the risk. Governments can handle it with helicopter money… but that’s literally just spreading the burden to everyone. The market can “handle” actual shortages by raising the price (when not prevented), the government can “handle” them by rationing, but if there’s a shortage (not in the strict economic sense) neither can make everyone get what they need.
Spreading the burden to everybody is what you need to do, though, if you want to avoid unnecessary deaths. Similarly with shortages. Markets raising prices leads to the poor having none while the rich have a surplus. Rationing means everybody survives at a reduced standard of living.
(Ok, sure, there’s some level of “shortage” where people don’t survive even with rationing, but for any level short of that, rationing works better than letting prices rise.)
except that rationing inhibits new sources.
Sure, rationing inhibits new sources. But we don’t actually need new sources of toilet paper (or most of the other shortages in this case). We just need time for a sudden demand shock (everyone moving from a one month supply of toilet paper sitting at home to a two month supply sitting at home) to percolate through the system, while the factories making toilet paper at the same rate people are using it just keep cranking away.
And for the medical supplies, we likely only have excess need for one year. A year of command economy in medical machines can fix that, and all it inhibits in terms of supply is the kind of factories that would sit largely idle during ordinary times and hope to make major profits during a crisis like this, which would necessarily be less well-informed (because they had to plan in advance) than a government acting quickly in the moment of crisis.
“Partying is looking for death”
“Those who go out for gatherings are shameless people”
“Stay in and don’t wander around,
You have AC, television, and wifi as your friends”
I may need to reconsider my anti-CCP stance.
I think most of these were put up by local government. Might not be reflective of the central party.
A lot of the banners are poetic, which the translations completely gloss over. Take this couplet:
口罩还是呼吸机
您老看着二选一
A mask or a breathing machine.
Looking at the two, choose one.
For whatever reason, I find this direct, borderline-ungrammatical translation much preferable to the article’s
A surgical mask or a breathing tube,
It’s your call
The banner Scott calls out is also rhymed lines of 7 characters.
The article’s translation somehow feels like it is suffused with ancient wisdom. I see a lot of translations of Chinese that are like that. I am guessing this is just translation style and the original wouldn’t sound full of ancient wisdom to Chinese speakers. But what do I know?
The odds favor guessing that the original reflected ancient wisdom.
It’s normal for politicians to open or illustrate speeches on mundane subjects with poetry or quotes from the classics.
Most Chinese ‘quotes’ we read in our MSM have been stripped of their context and sinisterized for our protection.
It’s just the stilted translations that make them seem quaint and yet wise. Part of the syndrome by which you can make any nugget of homely wisdom more evocative by prepending “Confucius say”.
Yeah, my initial thoughts upon hearing the UK strategy (note – I know nothing about medicine) was “that sounds crazy to me, but I’m kinda glad someone is trying something different – this will give us more data about what works and what doesn’t.”
Their pivot to “we will do what everyone else is doing” is slightly disappointing, in the sense that “everyone in the world do the same thing” seems like a poor strategy when there is still so much uncertainty regarding what the best thing to do actually is.
Suppression will clearly work in the short term. It’s too bad we have no way to get data about better long term strategies, but the UK government was staring down the barrel of 6-digit death figures over the next few months. They had to avoid that, now, and get to the medium term later.
For Iran the point wasn’t just the politician, so. It was also that all over the middle east, the first known Covid-19 cases were Iranian travellers. Maybe it is possible that they all got infected at air ports, but if the government of an country claims there is no local community infection, while you have several dozened infected travellers from said country, something is off.
Yeah. Hollywood actors have massively elevated risk. Iranian politicians are in Iran, and the official statistics from Iran are garbage.
The Our World In Data tools are gorgeous, but for the past week or so, their US numbers have been off from the ones the JHU dashboard shows. I think the reason is that Our World In Data is just using the numbers WHO reports, and JHU is supplementing those with state and local reports.
The difference has gotten to be rather large. Right now, WHO says the US has 3536 cases and 58 deaths, CDC says there are 7038 cases and 97 deaths, and JHU says 9415 cases and 150 deaths. Some of this is surely a difference in update times, but it’s still making it very hard to draw conclusions.
Wow, I didn’t know there was such a discrepancy in death numbers. But surely that must just be a time lag? It’s very hard to wrongly report someone dead…
It seems like deaths might take an extra day to update, but the number of cases seems to be in sync.
As of the time I’m posting this, Our World In Data shows 9,415 cases and 150 deaths for March 19 (which matches what you say JHU showed).
For March 20, they have 14,250 cases but still 150 deaths. JHU shows 14,250 cases and 205 deaths.
So I think data for yesterday and before should all be reliable, it’s just today’s data that might not be updated yet (at least for deaths).
Re: bag-masks, those are generally used during codes as an emergency measure. They’re better than nothing, certainly, but not nearly as good as ventilators. I’m a first-year respiratory student, and I was just about to learn how to run this junk when the disaster hit and now I’ll probably be out of school for at least a month (bah!). But basically, individual lungs have distinct properties (volume, compliance, etc.) which the bag can’t accommodate. If you’re going to be designing and mass-producing a bag-squeezing machine, you might as well just make a ventilator, which is, essentially, a clever computerized bag-squeezing machine. With some handy features like the ability to suction the patient without breaking the sterile circuit.
Even properly ventilated patients don’t have great odds of surviving this beast; if you just have a dumb squeezy machine, you’ll face such diminishing returns as to not be worth it IMO. A human can at least tell if he’s bagging effectively, notice when something is drastically wrong, etc.
Yeah, bag-mask venting is probably better than nothing if you’re out of ventilators, but it’s effectively a very inefficient version of a type of ventilator that is more typically used in neurologically devastated patients with healthy lungs.
Your school seems like exactly the one that should keep going. Maybe rearrange the curriculum a bit.
Two of the three instructors are working respiratory therapists. They’ll probably be needed on the front lines, and hospitals might be leery about doing clinicals while the sky is falling.
For right now, they’re just switching us to online classes only–including clinicals, which rather puzzles me. We’ll see how it falls out.
Every time I read about medical training it amazes me. This feels like something similar to the discussion a while back about how residents often don’t have time for lunch or to go to the bathroom, and I wonder how it got to that state. Hearing that somebody who has been in training to be a specialty that we expect to be desperately short of soon has had their training slowed down or maybe stopped rather than expedited makes me kick-the-cat angry. Like, the very first reaction to the leadership of your school should have been, “How can we cut the training down to get people who can operate ventilators out in the workforce, and how many people can we squeeze into that training starting tomorrow?”
The military learned long ago that you have to bite the bullet and take people off the line to train others. This was often seen in WWII pilot training where really good pilots were assigned back to the States to become instructor pilots. Often, these pilots didn’t even want to do that! They didn’t want to go ride herd on a bunch of trainees! But it ended up that one of the keys to US efficiency in the war was to do this compared to the “fly ’til you die” approach often practiced by the Axis powers, which meant they couldn’t pass on knowledge of how to succeed to new pilots.
We’re going to have to accept that we’ll have some respiratory technicians not in the hospital treating patients because they’re busy making more respiratory techs.
I seem to recall reading that one of the medium-term implications of the Battle of Britain was that the Germans had transferred many of their Luftwaffe flight instructors to combat assignments, expecting the war to be decided before enough new trainees could graduate to outweigh the value of putting more experienced pilots in the air immediately.
As it happened, they lost not just the cadets who now couldn’t be trained, but also a lot of experienced pilots including the former flight instructors. The Luftwaffe likely still would have been ground down by the combined industrial might of the US, Britain, and Soviet Union, but they probably would have been able to make more of a fight of it in 1941-43ish had they kept the flight training pipeline going in 1940.
Hopefully no one gets kick-the-CatCube angry!
It’s long been one of my theories that medical training in the US is harder than it needs to be. It’s probably not just because we’re keeping too many doctors on the front lines, either. I remember Scott talking about Irish doctors having identical performance to US doctors, while spending less time in university (along with the consequent tuition and other costs).
Then I think of the downsides of life of a doctor – the long hours, the malpractice suits, the grueling training process, the patients lost – and I wonder if the pay, the status, and the happiness of saving lives is worth enough to keep pulling more in, or if young people are scared away, who otherwise might increase the supply of health services. Is medical school still full? Is it worth looking for ways to ease up on the requirements?
Neither here nor there, but avoid using the phrase “respiratory tech” around any actual respiratory therapists. A respiratory tech is a now largely defunct position, and refers to the guy who fixes the machines but doesn’t help patients. And a lot of RTs have a chip on their shoulder about being overlooked all the time.
Anyway, I can accept that it’s really hard to tell someone “yeah, your grandma died in this pandemic because our RT was busy teaching some first-year students who won’t be able to function as RTs themselves for another year.” Especially since my lab instructor is a supervisor at the hospital. There are other things that are less easy to accept, like the push to make RT a four-year degree for dick-waving reasons I don’t understand. Gotta stay level with nursing, even if all the RTs say they learn almost all of their practical skills on the job.
As for getting us into the workforce faster, if it gets bad enough I suspect a lot of bureaucratic barriers will get torched in a hurry. For the moment, however, making any changes to RT certification involves coordination between state law, federal law, and three different governing bodies. Lately I’ve mused that perhaps disasters are like forest fires, burning out accumulated social detritus to allow new growth. But I’m grumpy right now.
Paul, the only difference between European doctors and American doctors is 3 years of undergrad. Yes, it’s entirely unnecessary, but it’s small compared to all the other examples in this thread.
@theredsheep
My apologies; I didn’t notice the usage in your post and didn’t know about the distinction.
The thing is that I don’t know you’d have to tell anybody that; this isn’t the kind of thing that you can trace to a specific person who would have lived or died based on this decision. I’m assuming that we’re talking a few percentage of respiratory therapists as instructors, and not, like, 20% of the current working ones. We’re trading off a slightly higher death rate now for a vastly reduced death rate later.
And I don’t think that it’d be advisable to try to do a full respiratory therapist* trainup right now. They shouldn’t have you doing telework or learning over the internet. They should have students like you, theredsheep, getting intensive training on ventilators and then getting kicked out to hospitals to run ventilators. It’s time for the kittens to go catch rats. I fully acknowledge that this isn’t ideal, and that you’ll have to be brought back to complete your course of study later, but there’s a whole hell of a lot going on right now that’s not ideal.
Tangentially relevant to this, I admit to continuing astonishment at how a bunch of agencies can’t seem to let go of their normal operations in an obvious emergency. What reminded me of this is your discussion about how your school is going to keep trying to run their normal course of study at a reduced rate to get you fully certified for your job using normal standards. The FDA and CDC seem to be doing the same “clinging to normal.”
This astonishes me as somebody who works for the federal government. At the risk of doxxing myself, I have a story about this: back in September, we had a sill blow out on one of our navigation locks. Normally, when we let a contract we have a very long lead time. Right now, if I want to have a contract awarded by the end of the fiscal year (September 30th) I need to have the completed package to our contracting office by May 1st.
We awarded the first of four contracts to fix that lock the 5th of September, the night the sill blew out–this one was to set the stoplogs to dewater the lock, since we “value engineered” out the crane that would allow us to do this ourselves when we built the lock–and the following three were to erect scaffolding, demolish the old sill, and construct the new sill on the 6th, the 7th, and the 10th, respectively. I worked on the demolition contract all day Friday and Saturday afternoon to get it awarded the 6th, and had a design ready for the construction contract on Sunday (it took a few days of negotiation before award on Tuesday the 10th).
Note that this is a lot less than 5 months! Everybody hates bureaucracy, but let’s consider why these types of timelines exist. It doesn’t take our contracting office the 5 months to review and put their stuff together; it’s only a couple of weeks of straight work, but they can’t guarantee straight work on a normal basis. They have to hop between projects like the rest of us. So 5 months is lined out so they can handle everything coming in with a routine level of effort. But why does all of the review they need to do exist? Because they need to ensure that a lot of things are in place: we have to have appropriations properly lined up, which takes back and forth with the money folks to make sure everything is square; they have to have a review from our lawyer, and she has to also have time to look things over; everybody has to have eyes on things to make sure that none of us are corruptly steering contracts to people giving us kickbacks, and this is much easier when things are moving like a slow river instead of rushing rapids. Stepping back further, we spend a lot of time working on designs to avoid making design errors that cost the Government money on contract modifications.
But note that if you’re willing to focus on one thing, exclusively, and aren’t going to be so fussed about drowning oversights and mistakes in a bucket of money, you can accomplish most of these goals without the huge timeline and bureaucratic box-checking! My boss fully accepted that everything that wasn’t that lock on my plate was going to burn to the ground. Normally it takes a few weeks to get our chief of Engineering and Construction to approve a design once us worker bees had it completed; she was waiting in her office on Sunday for us to get it done so she could approve it right then. The attorney was ready to review the completed contract that day as well.
As far as the concerns about contract corruption, there were enough eyes focused on this such that it was unlikely for that to occur here. You can’t keep that kind of focus on a single project on a normal basis, but this wasn’t normal.
And for the design timeline being long and beating everything to death to avoid mistakes? I made a mistake. It turns out that the design I pushed out on Sunday failed to consider several things. We didn’t notice this until after the reinforcement had been fabricated, so we probably raked about $30,000 of rebar (and $30,000 of taxpayer money!) into the trash once I had a new, workable design. But taking weeks to do a design with tows of barges waiting and the crews laid off was absolutely a bigger concern.
Similarly, during construction we expedited reviews. Normally, when the Contractor submits things to the engineering staff for reviews, we have 30 days to turn them around. Like the reviews above, it’s not that it takes 30 days to do the review, it’s just that that’s a good timeline for our Construction office to package them up and for us engineers to work it in to our other responsibilities.
Here, I was standing on the floor of the lock reviewing rebar drawings at one point. That’s a crushingly inefficient use of a structural engineer’s time, but from a wider perspective it’s still more efficient than tugboats with 20% of all the wheat produced in the US tied up at the dock.
Cycling back to my point: it’s absolutely possible for a US Government bureaucracy to do away with detailed procedures in an emergency, so long as you can come up with ways to mitigate the things the procedures are intended to guard against, which you usually can–or decide that the monetary losses those procedures guard against can be eaten.
This isn’t even something that I look to the White House about. I mean, better leadership on the President’s part could have helped to break logjams earlier, maybe, but I don’t understand why the permanent civil service can’t make these logical leaps without the intervention of the politicians. I think they’re the ones who really fucked the dog, here.
* I keep typing “respiratory technician” despite never having heard of operating ventilators as a separate discipline before all this went down; I don’t know why it’s sticking in my head! I apologize if I make that mistake again.
Hey, nobody’s heard of us. RT’s been a thing since maybe the ’60s or ’70s, while nursing’s been around since … the Crimean War, I think? Which is why all the news reports are frowning about whether they have enough nurses to run all those vents. But I’ve been in the program for less than a year, too short a time to really get a chip on my shoulder about it, so you’re fine.
Anyway, I live in Bay County, FL, which got hit by a Cat 5 hurricane in 2018. Both of our hospitals are still recovering, and a high proportion of the respiratory staff are traveling temps. Even if all was well, most hospitals short-staff RT because there aren’t any hard rules about how many you have to have per so many beds, like there are with nursing. This often leads to nursing being assigned some of our minor duties, with admittedly suboptimal results because they don’t really know lungs. So when/if we get hit, it’s going to hurt, and those two seasoned RTs will be missed on the front lines, NGL.
Some cybercriminals are doing their part by not targeting health institutions during the pandemic.
Attacking health institutions at any time is attempted mass murder.
About the manual respirator… Why in God’s name would we need a volunteer? “This motion needs to be repeated exactly for a very long time” is a solved problem. You use a motor. Furthermore, this design looks like it can be modified with little difficulty. Disconnect the mouthpiece from the pump, install three or four meters of plastic tubing, do this a dozen times, and line the pumps up between two boards that are connected to one piston that you plug into the wall. I’m sure there are problems, but they will be a hell of lot cheaper to solve than using 24 man hours a day per patient.
Motors need to be shipped, installed in machines by specialized workers, break unexpectedly, and must be paid for. People can walk, need only to be told “squeeze this” and can begin working, are much less likely to stop without telling someone first, and our culture is much more in to people volunteering their labor than companies volunteering their pallets of motors.
The manual bags (or mechanized versions) are not what people need when they have the specific kind of very bad lung thing that results from COVID-19.
Just moving air in & out at low pressure is not enough. Just oxygen (like through a nose tube) is not enough. Apparently people need specific, finely adjustable, higher pressure ventilation in addition to oxygen.
This is because parts of the lung are getting damaged & collapsing on tiny and medium scales such that they cannot absorb oxygen or get rid of CO2 effectively.
I’ve been writing a simple language explanation / ELI5 about this (also in comment above):
https://docs.google.com/document/d/1CPAYurZ0LUcaivoqh5J79EWqDySDj53ZIVL9LO57bw8/edit?usp=sharing
Wanting to share this so people can understand what we know so far. That way, people can:
– Focus efforts on interventions that will be more effective (more ICU ventilators & training) without wasting time on ineffective interventions
– Focus research on adjacent unknown areas that might unlock better treatments
Have also made this diagram w/interventions arranged by leverage:
https://docs.google.com/presentation/d/10_yi03HNlYqcDURcWXg_iG8dkJFPyvFtb5_M0lDc02I/edit?usp=sharing
Highest leverage to least:
PREVENT INFECTION
– (Develop vaccine)
– Buy time through social distancing, lockdowns, etc
– Get info via vastly scaling up testing
– More PPE for healthcare workers
IMPROVE SURVIVAL
– (Develop treatment / cure – antivirals etc)
– More ICU ventilator capacity
Lower leverage doesn’t mean not important — it just means you would have to push vastly harder on that one to make a big difference in outcomes.
Items in parentheses are ones that are in research stage
If you put a motor in it, you have created a medical device, and the FDA will probably take a year to approve it (actually, they won’t approve it at all, because it isn’t perfect).
(Anyone who thinks US regulators will get out of the way just because millions of lives are at stake hasn’t been paying much attention to the progress of the epidemic so far)
>(Anyone who thinks US regulators will get out of the way just because millions of lives are at stake hasn’t been paying much attention to the progress of the epidemic so far)
Besides allowing the first vaccine trial to skip animals and go right to humans? Or numerous states enacting emergency orders to relax medical regulations, including the one Scott mentioned in this post about prescribing medication with only a video call?
I guess none of that counts when you’ve got a bone to pick tho.
Out of the loop on the paracetamol: what does Scott supposedly know? WHAT IS HE NOT TELLING US?
Paracetamol == acetaminophen == Tylenol.
Acetaminophen and paracetamol are the same.
Liver toxicity, I think.
It must be a subtle reference to the meme in which a photograph of Jacob Rees-Mogg reclining is matched with the text “when you take three paracetamol instead of the recommended two.”
Bolding mine.
Tylenol, acetaminophen, and paracetamol are three words for the same drug, and Scott is referring to earlier in the paragraph when he also referenced ibuprofen by its “trademark name”.
Is it really so weird that politicians and actors and such are getting it? Considering it spread initially out of China by plane and cruise travel, it makes complete sense that people who fly a lot (rich people like politicians and movie stars) would have an outsize exposure risk.
One rich businessman gets it in China and flies back to wherever. He then attends a conference and shakes 50 people’s hands and it starts spreading among that circle.
This seems entirely plausible to me.
Obviously, there’s huge numbers of uncounted cases, but I don’t think you can extrapolate that number based on important, famous people getting it.
*Edit* NVM. Am idiot. Didn’t read the next paragraph before posting.
Since the US has (I assume) many more airports per capita than most countries, why did its curve start so much later than, say, UK (which probably has a similar number of airports per capita and a similar number of flights to and from China, but a much lower population)?
In case it’s unclear, I’m not trying to be facetious or anything–I’m wondering what drives this. Or maybe my assumptions are wrong.
Comparative lack of testing in the US early on. I think a lot of people are looking at the data as if it’s normative across all areas. I don’t think the data from early on will ever be reliable enough to form any firm conclusions from when people start trying to study the outbreak patterns.
The way I’ve been thinking about it is by analogizing an epidemic to a fire. Individual activated units (bits of fuel that are currently combusting; humans that are infected) have some probabilistic chance of activating their neighbors, and some of the units move around. There are thus several phases in any region – the early phase when no units are activated; a phase in which activated units are coming in from nearby regions but aren’t spreading yet; a phase in which there are enough activated units within a region, as well as enough susceptible ones, that spread is sustained; and later a phase when there aren’t enough susceptible ones left for spread to continue.
If one tree is burning, and is giving off sparks that hit many other trees, it’ll be a matter of chance which other tree is the first one to catch fire itself. The probability of any individual tree being the second one to catch fire is going to depend on the number of sparks hitting that tree from the original one. But if there are enough trees with a few sparks and few trees with a lot of sparks, then it may still be more likely to be one of the trees with a few sparks that catches second (and that appears to be what Italy and Iran were) than that it’ll specifically be the tree with the most sparks. And given the exponential nature of local spread, whichever tree catches fire second is likely to be burning much more heavily than the trees that catch fire fifth and sixth, even if the fifth and sixth are getting a lot of sparks from the initial tree.
If we rewound to the beginning and played it again, it’s very unlikely that Italy and Iran would be the major centers of infection after China – but there are a huge number of places that it could have been, and wouldn’t necessarily be Japan or the United States or the UK, even if those are the individual places with the most flights to China.
Considering it spread initially out of China by plane and cruise travel, it makes complete sense that people who fly a lot (rich people like politicians and movie stars) would have an outsize exposure risk.
But they tend to fly in private planes, where the few passengers have more (physical) distance between them.
No, many celebrities and rich people do not travel by private jet. I’ve travelled commerical with any number of wealthy venture capitalists (San Francisco to/from New York flights are full of them), and also Megyn Kelly and her family. Only difference is they were in 1st while I was in
steerageeconomy. I once saw Yao Ming come off a commercial flight at SFO too.I once shared a Southwest flight with Ted Cruz. I was ahead of him in line because apparently consulting firms will spring for Business Select, but Congress won’t…
The risk associated with flying isn’t so much the risk of being in that one room with 300 people for six hours – you get exactly that same risk if you go to a conference for a day or attend an opera or a few sporting events. Rather, the kind of people that fly a lot are more likely to be early adopters of any disease because there are more places that a disease could originate in which they are likely to have a chance of catching it. (This is also the same reason why the kind of people that fly a lot are also more likely to be early adopters of any sort of fashion trend or food trend – Nashville hot chicken isn’t going to pop up in Oakland directly, except if it’s mediated by the kind of people that fly to both Nashville and Oakland on a regular basis.)
Re “Flattening the Curve is a Deadly Delusion”—which has since been retitled to “Don’t ‘Flatten the Curve,’ squash it!”:
The shape of the curve doesn’t actually matter at all to the point of the article, which was simple and was missed by everyone who criticized it.
The point of the article was this: moderate measures that *only* slow the spread, but don’t reduce the total number of cases, have no hope of keeping cases below hospital capacity. The only way to avoid swamping the system is to take extreme measures the get R0 < 1.
And further, all the simplified diagrams that have been going around to promote “flattening the curve” are so quantitatively inaccurate that they are misleading people as to how much capacity we have, and how strongly we need to force down the curve.
Here's Timothy Gowers making the same argument for the UK, not even using any curves or modeling, just napkin math: https://twitter.com/wtgowers/status/1239159256034750464
But any measure that slows the spread will, all else being equal, also reduce the total number of cases. To repeat material from my post: in the SIR model, some fraction of the population (s_inf) never gets infected, and this fraction is a decreasing function of R0, as shown in section 5 here.
In other words, any measure that “flattens the curve” (slows it down) will also, by default, “shrink the curve” (decrease the total number of cases). We don’t have to pick one of these and reject the other. Both Bach and Gowers assume the total number of cases is fixed and we’re just re-distributing them over time, but in practice you can’t really do the latter without changing the former.
Arguably, this is a flaw with the “flatten the curve” messaging itself. The infographics sure make it look like the total volume is being held constant and merely re-distributed in time. I think the infographics assume their audience believes something like “public health measures are to stop a disease, if the disease keeps on spreading then they didn’t work,” and they’re trying to argue “no, we can use public health measures to turn a horrible spread scenario into a much nicer spread scenario, even if the disease spreads in both.” The implication that the volume stays constant — “no shrinking, just flattening” — is unfortunate and unintended; the intended point is the more basic one that there will still be a curve despite the measures, with a similar shape including the exponential onset, and that a flatter/smaller curve of the same kind is an immense improvement, not an indication of failure.
But the soundbite-level messaging chosen to communicate this makes it sound like volume is constant. If you’re mathematically astute and you take the soundbites literally, like Bach and Gowers, you’ll conclude that “flattening it” can’t possibly be very effective and we need to “stop it” instead — ironically, the same conclusion the soundbites are trying to combat.
This is why it’s so important to have some dynamic model of disease transmission when you’re doing these calculations, even a super-simple one like the most basic SIR model. With a dynamic model, you have equations connecting all the variables and so you’ll be forced to correctly update all downstream effects when you vary their cause. In the Bach/Gowers analyses, R0 is varied and one of its effects (growth rate) is updated, yet another effect (total cases) is held constant at some widely quoted value. (Each of the widely quoted total-case estimates was itself computed from some specific R0 value! These estimates are not constants w/r/t R0, as their originators would be the first to assure you.)
It sounds like now you substantially agree with the article and are criticizing the misleading “flatten the curve” messaging more than Bach’s article. Bach isn’t assuming the number of cases is constant: he is showing that *if* you don’t reduce the number of cases (which is what comes out of the “flatten the curve” messaging), the result is disaster. Therefore, we need to reduce the number of cases — and I think you agree. Bach doesn’t go into details of what interventions should be done to reduce the number of cases: he is just stating what the goal needs to be. Of course the same interventions will work towards both goals.
In the tumblr post you critique particulars of Bach’s model (e.g., Gaussian curve, and using parameters that we don’t know exact values for) but Bach’s conclusions are only barely sensitive to these details, and the article itself already points out these shortcomings anyhow. And if you find Bach’s model oversimplified, then surely the “models” he is criticizing (which are just bell curves with no scale bars) are much worse? And Bach has now updated the article with links to people who have done more careful calculations, anyhow.
You’re right, I don’t actually disagree with your characterization of Bach. But, if this is what Bach is saying, I don’t understand what’s materially at issue.
Like, sure, if there were some weird, atypically bad intervention on the table that did only cause flattening and not shrinking, then we’d all agree that intervention would be limited in impact, and insufficient without others. But no such interventions are on the table.
In practice, “flatten the curve” as a slogan just appears to mean “yay for interventions that ‘merely slow’ the disease like social distancing!”, as contrasted with containment interventions that in principle could stop (not slow) the geographic spread. If Bach’s claim were just “shrinking the curve is the target,” then he’d advocate for any method that shrinks the curve, including the social distancing etc. that the flatteners are so keen on. But that’s not what he does: in fact he explicitly argues for containment as against “merely slowing” measures. (“It is possible to stop the virus!”, he writes.) Why, on your construal of Bach, would he have this preference?
For reference, consider this WaPo interactive simulation of an SIR model. In my experience, this is the sort of thing the “flatteners” provide to substantiate their position, and it has “flatten the curve” in the title (though perhaps chosen by editor, who knows). The text argues against containment and for social distancing, citing the simulations, in which “containment” fails at both flattening and shrinking, and “social distancing” succeeds at both.
Now, this is a stylized model with toy numbers, and maybe the conclusion isn’t right — but does model conditions under which containment would fail your/my/Bach’s goals where “merely slowing” interventions would succeed. And — as elsewhere in “flattener” discourse — it’s not comparing methods that don’t shrink with those that do. It’s arguing that a subset of methods-that-shrink is better than another subset, and calling the former subset “flattening the curve,” because that’s what the term now means in common usage.
EDIT:
I argue that this is false in the second bullet pt of my post.
Your second bullet point is not an argument, but an assertion. And it’s just flat-out wrong. The gaussian assumption is doing no work whatsoever.
Quoting from Bach’s thesis: “[Flat-curvers] mean to tell you that we can get away without severe lockdowns as we are currently observing them in China and Italy. […] These suggestions are dangerously wrong, and if implemented, will lead to incredible suffering and hardship.” Certainly minor mitigations *help*. Bach’s point is that the problem is larger than the “flat-curve” diagrams suggest, and much more mitigation is needed. Bach finds the traditional “flatten-the-curve” diagram dangerous because he believes it will lead to complacency and failing to be aggressive enough. I don’t see anywhere where he says he is against minor mitigations; he barely discusses specifics of mitigation measures at all, except that is he vehemently in favor of more.
Re. the second bullet point, you mean the part about the mass being concentrated near the peak? I don’t foresee this being a big source of error. Try using a step function (going from 0 to A to 0), which is the least concentrated peak you can make, and I’m fairly confident you’ll reach the same conclusion that merely spreading the peak is not viable. (In fact, I just ran the numbers: the peak would need to be spread over 4.9 years, which is biologically unreasonable, and even requires that no one else in the US needs a ventilator until then. The conclusion — that drastic intervention is necessary — stands unchanged.)
Whatever the true curve is, I think you will agree that it is more concentrated than a step function. It is mathematically impossible for any curve to be less peaky.
At this point I don’t understand what part, if any, of Bach’s article you find to be inaccurate, except that the shown infection curve isn’t quite the right shape. Maybe quoting the objectionable part would help?
Re. the WaPo model, I strongly dislike that article and find it misleading to the point of deceit — but that is a long digression.
Re ermsta (I don’t seem to be able to reply, maybe due to nesting depth)
Great point about the step function. That convinces me that Bach would not have drawn a different qualitative conclusion if he had used a different functional form, no matter which one. I’ve updated my post with a note about this.
On the other topics — this discussion has grown quite complicated, since there are many topics of potential dispute: Bach’s argument, his conclusions, the argument/conclusions of the “flatten the curve” diagrams, Bach’s beliefs about what the “flatten the curve” arguments say, etc. I’m only trying to critique Bach’s argument in itself.
Earlier today I edited in some clarifying material into the start of my post, so if you haven’t read that, check my post again and it may help. Since you wanted quotes, here’s the same thing I said there, but framed in response to a specific quote.
Remember, from my post, that the 40-to-70% estimate here was derived by Marc Lipsitch from an estimate of R0, combined with some informal reasoning. When a lower estimate of R0 came out, he revised this number downwards to 20-60%. So clearly this value quoted by Bach is dependent on the R0, and will nontrivially increase/decrease as the R0 increases/decreases.
But interventions like “if we wash our hands and stay at home while being sick” decrease R0. It doesn’t matter how much, for my purposes here, just that it happens. Indeed, any plausible intervention that would flatten the curve would lower R0 in the process.
So the 40%-to-70% number can’t be carried around with us, as a constant, when we compare across different intervention scenarios. If we’re considering a scenario in which the curve is flatter, then that scenario will have a different R0, and so the total number infected will be different.
But Bach does treat this number as a constant, across the flattened and non-flattened scenarios he compares. This simply cannot be a valid argument about the difference between the two scenarios: if the total number infected is accurate for one scenario, it is ipso facto not accurate for the other.
Bach doesn’t consider questions like whether some intervention will or will not flatten the curve, or will or will not lower the number of infected. This is totally orthogonal to his argument. All he argues is that if 55% infected => medical system overloaded. The part you quoted says that handwashing etc. is not good enough by itself unless it lowers the percentage infected to below 40%. I’d guess you agree with that (although maybe only vacuously).
Since Bach’s results are linear in his parameters, you can consider other scenarios besides 55% infected. I find that around 0.1% – 1% infected is when it becomes feasible that the medical system might not be overloaded. (For comparison, Hubei had ~0.1% officially.) Feel free to try 40% or 20% if you feel those scenarios are more useful to consider.
I’m not criticizing the misleading “flatten the curve” messaging, I’m criticizing articles which mistakenly assume that “flatten the curve” implies or asserts that we’ll have the same number of cases, just spread out more, rather than that slowing transmission reduces overall harm dramatically, *partially* because it reduces overloading of hospitals for any given number of cases, and *mostly* because it reduces the number of cases in total.
But it’s also significant that spreading things out *does* disproportionately improve outcomes in a number of ways, and the net result is that all the people I’ve seen arguing against “flatten the curve” have given the strong impression to casual readers that they think that flattening the curve implies actively trying to ensure that the disease doesn’t get stopped, and also that completely ending the transmission of the disease would not be a an archetypal example of “flattening the curve”.
Since there’s at least one case, there is a curve. If we lock everything down and basically end transmission, we’ll have flattened it.
So, if I’m reading this right, the reason that social distancing reduces the number of cases is simply because it reduces R0. Since R-effective is a function of R0 and the fraction of the population that is still susceptible, reducing R0 causes R-effective to drop below 1 sooner–say, maybe when 40% have been infected instead of when 70% have been infected. As soon as R-effective is less than 1, the number of new cases starts to drop, but the number of susceptible people also continues to drop. So we can gradually ease off our social distancing measures without causing cases to spike again.
Here’s the thing, though: in order for this to work (to minimize total cases), we don’t actually have to reduce R0 now, at the beginning of the exponential curve. The crucial time for lockdown measures would be shortly before the peak–specifically, at (or just before) the point where we think it would have peaked if we’d had a lockdown right from the start. All we gain by locking down early is delaying the timing of the peak a little bit. Not that this will stop me from staying home, but it does seem like we have a little time for governments to get their act together and reduce the disaster as much as possible.
If the lockdown is good enough, then it will be shortly before the peak no matter when you deploy it.
Sure, but if you do it early then when you eventually release the lockdown you’ll get a rebound in cases. The idea here would be to find a balance point where partial herd immunity plus a medium amount of social distancing (that is tolerable for the long term) is good enough to get R<1.
Why would there be a rebound? As far as I know, there’s no animal reservoir and the virus doesn’t last *that* long in the wild, so all you need to do is interrupt the chain of transmission and make sure you don’t get reinfected by travelers from other areas.
> Why would there be a rebound?
Because it lasts longer on hard surfaces than people think, people touch their faces more often than they think, it’s more contagious than people think, there’s more latent infection than people think, and a->b->c->d->e->f->g->h->i->j transmission can be quite a long time.
Florida beaches aren’t shutting down until tomorrow, last I heard. (Couldn’t easily find info on an end date, but they are only requiring restaurants to reduce seating capacity by 50%.)
> Why would there be a rebound?
How long does cv19 survive in a fridge? A freezer?
> How long does cv19 survive in a fridge? A freezer?
“Survive” is an interesting question here.
First of all, it’s IMHO an error to consider a virus alive. I know some virologists consider them alive (and some do not). I personally, having gone through the arguments, consider them life-adjacent. They’re made up of organic molecules but have no metabolism. So, in that sense, they’re like frozen meat. Got that metaphor?
It’s likely safest to assume that, like frozen meat, they do not readily break down in the refrigerator or freezer.
@deirdresm
I agree. Should have asked “How long can they retain the capacity to infect…” The answer probably is informed by the ambient humidity, not just temperature.
Isn’t the problem of waiting until shortly before the peak to use lockdown measures that by that time our healthcare systems will be swamped and there will be many excess deaths due to lack of access to care?
Yes. It would definitely be better to do a full lockdown (or intermittent full lockdown) until we can get a vaccine/treatement. But if we can’t or won’t sustain a lockdown, as seems to be the case currently, then calling for a temporary full lockdown just before what would have otherwise been the peak might be the optimal timing for minimizing total number of cases.
Actually nevermind–I looked into this using the epidemic calculator and a reduction in R0 shortly before the peak hardly helps at all. To help significantly, the lockdown has to be just about as extreme no matter when you do it.
Thanks for writing up and boosting the visibility of this argument. I agree with your analysis, both against the viability of “flatten the curve” and the use of a Gaussian to make that argument.
A few days ago I ran some simple SIR model simulations. [1] I’m in the US and following US news, so the numbers are US-based, too. (Disclaimer: I am not a professional, treat these models with reasonable skepticism.)
Even in the fairly optimistic scenario, the US peaks at 20M simultaneous cases around 300 days from now. Given all the headlines about hospitals being overwhelmed and running out of equipment *now* when there’s only ~15K confirmed cases, 20M simultaneous cases sounds catastrophic.
My big take-away from looking at the models was that the outcomes are very sensitive to tiny changes in R_0. The total number of infected is much lower if R_0 is smaller, and drastically lower if we can drive it below 1. To me, that seems like the only reasonable goal.
That said, the argument against flatten the curve is so overwhelming that that it doesn’t take a realistic model to make the case.
Let’s say the goal is to expose 70% of 300M US residents. Assume each infection lasts two weeks. That translates to ~3 billion infection-days. Even if we assume we can precisely control the rate of infection, we’re still in bad shape. We can have 8M people sick for 1 year, or 4M people sick for two years, or 16M people sick for 6 months. None of these options seem very appealing.
[1] https://www.kaggle.com/rlarocque/sir-model-us-covid-19
We can have 8M people sick for 1 year, or 4M people sick for two years, or 16M people sick for 6 months. None of these options seem very appealing.
“Go and tell David, ‘This is what the Lord says: I am giving you three options. Choose one of them for me to carry out against you.’”
So Gad went to David and said to him, “Shall there come on you three years of famine in your land? Or three months of fleeing from your enemies while they pursue you? Or three days of plague in your land? Now then, think it over and decide how I should answer the one who sent me.”
David said to Gad, “I am in deep distress. Let us fall into the hands of the Lord, for his mercy is great; but do not let me fall into human hands.”
Only if implemented indefinitely. If you’ve reached 1-1/R0, then you relax restrictions, you’ve changed R0 (not just R), and your number of cases goes up again. That’s why flattening the curve can’t work; you need to keep restrictions until you reach 1-1/R0 for an unrestricted population, or until the disease is truly extinct.
Yeah, this version of Nostalgebrist is even worse than the original. He keeps insisting that it’s important to have models, but he never bothers to think about the meanings of the numbers that these models spit out. Joscha Bach is actually modeling, whereas Nostalgebrist is using models as a credential.
The popular flatten the curve graph also has ICU capacity as being fixed. This is unlikely to be true and depending on how fast it can be expanded it could be very important as to whether flattening the curve can work.
Even increasing ICU capacity by 50% and flattening the epidemic curve to 18 months will result in ICU capacity at 166%, according to this model: https://www.healthaffairs.org/do/10.1377/hblog20200317.457910/full/
But ICU demand at 166% of capacity is still much better than at, say, 200% of capacity, right?
And where are you going to get the staff for that, given that this is a global problem?
Re: the link to reductions in death due to reductions in air pollution (due to reduced economic activity) — what about reductions in traffic injuries & fatalities due to work-from-home & shelter in place?
I imagine this will become huge as time goes on, and would love to see some math & modeling of this
This is what I thought reading that, too. I’m an IC contractor and have no choice but to keep going in to work at least some of the time, but the roads are practically abandoned. Normally, there are at least two accidents per commute leg. There has to be a drastic reduction in property damage, injuries, and deaths from vehicle collisions.
Sad thing is it didn’t take a global pandemic to achieve this. We could have just allowed people to work from home anyway.
Working from home properly requires a home office, and that’s extra hard for people with kids. I think a better compromise would be many small coworking spaces, where people can focus and/or make calls as needed.
I want to see that also including the suicides and long-term mental toll from the isolation and lack of community, support networks, and human contact.
One weird factor in traffic injuries is that the biggest factor in injuries for pedestrians is the speed of vehicles, and not the number of vehicles. In a congested city, you can easily get around on foot without getting hit (and even while hitting some cars yourself if you want to send a message to drivers who have stopped in the crosswalk). But if traffic is now free-flowing, those 45 mph speed limits on most American arterial roads mean most people who get hit will now die, in addition to meaning that drivers are more likely to hit people because they’re going faster and reaction times are thus not safe enough.
Is there any reason for suburban residents to avoid going outside for a walk/run, as long as you’re staying more than six feet away from other people at all times? This seems like a very low risk activity, but I’m not sure if there is some factor I’m failing to consider.
Nah, you’re good! The only thing you’re failing to consider is that exercise and sunshine will bolster your immune system.
I’m in an urban environment, in an apartment building, and I’m wondering if I can’t get away with the same thing if there’s few people on the streets. I’m on a somewhat busy road, but its not very busy these days, and the side streets are quite clear.
The main danger I can think of is the doorknobs/elevator buttons I need to touch to get in and out of the building. It would be fairly easy to use a napkin or whatever to prevent direct contact, but I don’t know if that’s good enough.
No expertise here and I haven’t seen much coronavirus-specific discussion of this, but I can’t see it failing provided you’re sensible. (Use a reasonably thick wad, avoid visibly wet surfaces, make sure the contaminated side doesn’t come into contact with your or your clothing or your possessions before you throw it out.) If you’re worried about napkins being too porous, you could use e.g. a combination of a napkin and some plastic or a bit of cooking foil (maybe not the foil alone, because a few layers can break easily and many layers can be inflexible).
A quick (and not coronavirus-specific) google didn’t turn up any real evidence against; the ‘debunking’ points were either dumb (‘most of the microbes on public surfaces are harmless!’) or assumed you would do it in a dumb way (‘if you put the dirty tissue in your bag or pocket, you’ll come into contact with the germs later’).
edit: this wasn’t meant as any comment on the other means of transmission, and the possible threat of e.g. standing in an empty but recently-occupied elevator — just a suggestion that doorknobs and the like shouldn’t be a problem if you take the right precautions.
I’ve been going out with two wads of napkins, one each to open all the doors with on the way in and out, that I immediately throw away. I’m definitely not directly touching anything, so I also don’t see a problem with this. Unless there can be enough of the virus lingering in the stairwell to get me sick, seems safe enough to me.
The main reason why some countries ban people from going outside seems to be that a lot of people are stupid and interpret being able to go outside as permission to interact with people closely.
It’s fine to do things on your own or with the people that you are in a bubble with (partners, housemates, live-in children and others who you are going to infect anyway if you get it or vice versa).
Personally, I go out every day. Usually motorcycle, never public transport. I shop for groceries too, while keeping away from people. I probably should wear a mask as well. And I’m pretty careful with using hand gel and separating street clothes from home stuff.
But apart from that, I think just walking around is fine.
Walked several times today because they had to be short walks.
Met a dog that, by the way it barked, was really into social distancing.
If you’re asking the question I’m sure this tip is unnecessary, but just in case the habit is strong enough to bypass your conscious mind: remember not to touch pedestrian crossing buttons directly, or at least to keep the relevant hand away from everything else and wash it well (before as well as after, for other people’s sake as well as your own).
One new piece of data I’ve seen that I think it’s important to understand is that it isn’t only older people who seems to be in some degree of danger from the virus.
https://www.washingtonpost.com/health/2020/03/19/younger-adults-are-large-percentage-coronavirus-hospitalizations-united-states-according-new-cdc-data/
38% of people hospitalized in the US are between 20 and 54 years old. There also seems to be fairly high rates of younger adults being hospitalized in France, Italy, and the Netherlands.
Though note that this is hard to measure/confounded and alternate measures show much lower estimates, e.g. http://www.arnoldkling.com/blog/an-alternative-estimate-of-hospitalization-by-age-group/
Thanks for the link.
If I’m reading it right, that research seems to assume hospitalization rates are similar to death rates? I’m not an expert but doesn’t seem right; wouldn’t you expect a young healthy person hospitalized to be more likely to survive than an older person?
I also believe the other data I linked to isn’t using testing rates at all, it’s just how many people are currently hospitalized, which seems high in several countries.
The issue here is undercount of mild or wholly asymptomatic cases. I’m guessing 4x times the published number of cases, with mild ones skewing young.
What percentage of the total population is between 20 and 54 years old?
+1
Base rates, people.
I did a quick google on this, and it looks like about 47% of the US population is between 19 and 54, and 29% of the US population is over 54.
https://www.kff.org/other/state-indicator/distribution-by-age/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
So people over 54 are being hospitalized more often then people under 54, relative to their numbers in the population, but not by nearly as large a margin as I had expected.
Note that anyone 55+ in 2020 is literally a Boomer, that demographic younger generations have claimed to hate so much for many years.
How long is the entire population going to accept no restaurants, bars, gyms, haircuts, etc. (minimum) to having to fill out a police form every time they step outside for any reason (current Italian law) and a possible 13% reduction in GDP if 62-91.2% of people requiring hospitalization are Boomers?
I predict with 80% confidence that we’ll only tolerate the initial 8 weeks.
But they’re also the parents of millennials and the grandparents of post-millennials, and surely this is the kind of crisis that will sharpen people’s focus on their loved ones, regardless of whatever group-based sneering they’ve been doing during the relatively good times.
Boomers are grandparents of millenials, you’ve skipped over Xers for some reason.
Lots of milliennials are later children of Boomers. Everyone skips over Xers, our generation is too small to matter.
‘[generation a] are the parents of [generation b]’ is never more than a rough generalisation, but Wiki gives me ranges of 1946-1964 for Boomers and 1981-1996 for Millennials. So plenty of Millennials have Boomer parents. Even the very earliest Boomer only had to be 35 to have a Millennial child, while the latest Boomer could only have a Gen X child while aged 16 or under.
Trying to be slightly more rigorous: in my country the median age of parents (at the time of giving birth) during the Millennial era looks to have increased from about 27/30 (mother/father) in 1981 to about 29/32 in 1996. So the median parent of a Millennial is a Boomer for almost the entire range.
That banner explicitly restricts itself to talking about New Year celebrations, so I don’t think you’d be sending the message you intended.
For some reason I like the idea that the Chinese government might turn its propaganda posters into seasonal merchandise for Western consumption.
Also working on a leverage points diagram for interventions around COVID-19:
https://docs.google.com/presentation/d/10_yi03HNlYqcDURcWXg_iG8dkJFPyvFtb5_M0lDc02I/edit?usp=sharing
Highest leverage to least:
PREVENT INFECTION
– (Develop vaccine)
– Buy time through social distancing, lockdowns, etc
– Get info via vastly scaling up testing
– More PPE for healthcare workers
IMPROVE SURVIVAL
– (Develop treatment / cure – antivirals etc)
– More ICU ventilator capacity
Lower leverage doesn’t mean not important — it just means you would have to push vastly harder on that one to make a big difference in outcomes.
Items in parentheses are ones that are in research stage
What’s your metric of “harder”? Social distancing requirements as severe as those in Italy, CA, etc are extraordinarily expensive and hard to sustain for extended periods in non-police-state societies. More widespread testing, OTOH, has indirect leverage in that it lets you drastically reduce the cost of social distancing by narrowing the slices of the population to whom it’s applied. So I have trouble understanding why it would be considered lower leverage overall.
I think Sarah is implicitly weighing in the time scale of effect. Social distancing/lockdowns etc are useful for reducing infections immediately. Widespread testing and contract tracing are likely to be quite useful for controlling the virus long term. However, if we’re trying to stave off disaster in the next couple of months, testing is going to be of limited utility, because we have neither the technical nor organizational infrastructure to conduct testing at an appropriate scale.
Social distancing/lockdowns work for relatively high levels of infection, while widespread testing and contract tracing only work if the virus is relatively rare.
Exactly. This is what I don’t understand about why people keep looking at increased testing as something that will help alleviate the crisis in the coming month(s). If people really are susceptible prior to coming down with symptoms, nothing short of a daily test (one that’s not qPCR based, and doesn’t take 1-3 days to get results) would be beneficial once community transmission is established – as is already the case for a number of US states.
So maybe widespread testing in Montana (12 cases to date) would be beneficial, but it’s not going to do anything for NY, CA, WA, GA, MA, IL, etc. So why is everyone acting like widespread testing is going to save us – or even help all that much to stop the spread of disease. The most it can do is tell us when things are beginning to die down and we can start to breathe easy again.
Of course, we can’t tell when/whether transmission is increasing exponentially if testing increases exponentially.
Testing is beneficial to at least the extent that any part of the contagious period occurs after symptoms are manifest. You seem to be suggesting that there is no benefit short of perfection, but since we only need to get an R0 of ~2 down to <1.0 by all measures combined, less than perfect testing can still be good enough.
Testing is, in this context, beneficial to roughly the extent that disease transmission occurs after symptoms are manifest(*). That's most of the infectious period by raw chronology, and even more so weighted by probability of transmission – there is a non-zero probability of transmission by asymptomatic carriers, but the ones who are coughing have a much higher probability of transmission.
Testing is also beneficial in that, having identified one (possibly symptomatic) case, one can then go test their associates and contacts and identify them even before they have developed symptoms. If they’re contagious, they’re testable.
For best results, test twice – once at the first possible opportunity, once more 3-4 days later. This is probably good enough, and we don’t want to let perfection be the enemy of good enough.
* plus the delay from symptoms to testing and isolation.
If there’s any path out of long term, titrated quarantine that isn’t “fuck it, let ’em die”, it will probably look like:
Places with substantial outbreaks will implement radical intervention (i.e. shelter in place) to reduce transmission, while testing and contact tracing capacity get built up. Places without substantial outbreaks will get substantial outbreaks, and then implement radical intervention, while building up testing and contract tracing capacity.
But current testing capacity is inadequate for any goal we might have, except diagnosing some fraction of sick people, and letting us know when they’re no longer sick. The testing guidelines preclude identifying symptomatic community spread, much less asymptomatic spread.
I’m down on testing as a solution in the near term because there’s been too much spread. Yes, it will help us keep R down. But the widespread presence of asymptomatic carriers seems to mean that testing capacity will have to be really really high to suppress R enough to matter. Without adequate testing capacity, the interventions left are the radical ones.
@roflc0ptic
So this goes back to the question I still can’t find a good answer to. Yes, we need tremendous amounts of testing capacity and we don’t currently have the infrastructure. But South Korea does, and used it, to excellent effect. Why can’t we get at least what they have– crucially, including enough spare testing capacity to test a sample of ordinary asymptomatic people– in the next month or two?
@John Schillling
I’m not saying there’s no point to testing. I’m saying that using it to reduce R0 like you’re talking about make sense when there are a few cases, but at a certain point those measures have very limited efficacy. Certainly what Scott said above is a heavily optimistic view of what testing can accomplish:
That (and what you’re talking about) are great for handling a handful of cases, but not thousands or tens of thousands. Especially if there’s community spread. Early on, lots of testing can allow a testing-based containment plan to function well. At this point, widespread measures are much more effective. Testing millions of people isn’t going to save us, and it’s not going to get R0 down.
Here’s the thing about testing. It also identifies part of the set of people who have had it – and recovered. (It may identify them preemptively.)
I’ve heard a little bit about people getting reinfected, but nothing that sounded unambiguously like “this could not have been a false positive on recovery.” Unless this disease is extremely unusual in a very specific way, (most) people who have had it once should be immune. If we knew who was immune, we could explicitly remove those people from lockdown, permanently, which seems as if it would be very useful. Obviously an antibody test would be better, but a positive test for the disease followed by negative tests sounds like an inferior-but-still-very-useful substitute. It doesn’t solve all the problems, but it makes them better.
Aside from “but what if most people don’t develop immunity”, which I’m currently assigning a very low probability to, what am I missing?
That’s only for the antibody test, not the WHO test.
Just a quick point re: immunity.
As mentioned, we are a little unsure about how immunity works right now with the COVID-19 virus, SARS-CoV-2, with case reports of reinfection. We also don’t know exactly how long immunity would last, but judging from the results of other types of coronaviruses (like the common cold, SARS, MERS), it would be a temporary immunity. Research on the SARS virus, which SARS-CoV-2 is ~70% genomically similar to, shows SARS specific antibodies begin declining after 6 months and become undetectable at 2-3 years. Since simple antibody counts don’t necessarily tell you if reinfection will be prevented, we also don’t know if those patients would have been immune when re-exposed.
I’ve read a few studies that also point to recovered patients having increased susceptibility to respiratory infections afterwards.
Another challenge is there are at least 2 different strains, of SARS-CoV-2, though with only slight differences. Hard to tell right now if that will have an effect on immune response too.
@Aapje: Preemptively.
Any test that identifies who has it, will identify who in a month or two will have had it and recovered – those who tested positive and then sufficiently negative.
@Sunnydestroy: Thank you. Probability estimate raised slightly, and I may want to do more research. I thought the cold issue was just that there were a lot of colds/by the time you got it again it had mutated too much for your immune system to recognize it.
There’s also a practical issue with exempting survivors from lockdown. If you do that, all the stupid people who just want to party will claim to have already gotten it and recovered.
That’s true, it needs a police-state… But what is surprising is how fast and easy democratic state slip into police-state… I live in a locked down european country, and it took about 10 days. True, it’s for the good cause, but it make you wonder how democratic modern western state are in the first place. My prior was not too much. Covid updated that to even less…
now i am scared of 3 things, in decreasing order of anxiety:
How much wealth will i have lost, once the epidemy and economical crisis have come and gone
How much my country (and the other countries i frequently visit) will get back to democracies, or more accurately, how much individual freedoms will i get back. Democracy is an easy word, and i fear it will become more and more empty
Will i survive without permanently decreased lung capacity if i get hit by the virus.
i am in good health and a few year below 50, so it may explain my priorities, but my health is not my main worry at this time.
IMO, the scorched earth partisanship of recent years and the polarization that drives it is a much bigger threat to democracy than temporary public health measures.
@Loriot
+1
In case of CV19-caused absentees, the opposite parties in the German Bundestag will have a number of their members abstain from voting, in order not to distort the powers as they were elected.
That is a strong psychological signal against panicking about power grabs and instability at the highest government levels, and easy to implement on any level of democratic governments.
Most democratic states have an ability to implement emergency measures … the important thing is switching back.
I’m writing a simple language explanation of what causes COVID-19 ARDS (the very bad lung thing) and wanting input on how to share this more widely / where it would be most useful:
https://docs.google.com/document/d/1CPAYurZ0LUcaivoqh5J79EWqDySDj53ZIVL9LO57bw8/edit?usp=sharing
A molecular biologist and lung physiologist looked over it and said “It is very good!”
Why it would be useful to read this:
– Understand why “just give more oxygen” won’t work in severe cases, and why people are needing higher pressure full-on ICU ventilators – not Ambu bags or other low tech ventilation
– Share the known factors in easy-to-understand form, so people can direct more attention to the unknown factors
> not Ambu bags or other low tech ventilation
Silly question, but are you looking at only the pressure you can get with a BVM using the mask alone, or with the bag attached to an endotracheal tube? Using a BVM with the mask alone would have trouble getting consistent good pressure. But intubated it shouldn’t be that hard. And you can attach a PEEP valve and a few other things to a BVM to do interesting things with pressure.
You might find this link interesting.
Metaculus has a lot of Coronavirus related predictions up.
all the latest news and data https://worldcoronavirus.org/
MultiState has a detailed tracker of all the official actions states and localities across the U.S. are taking: https://www.multistate.us/pages/covid-19-policy-tracker
For what it’s worth, my opinion of Triplebyte was already pretty abyssal, having taken their test three times. For those not aware, they’re basically a company that interviews programmers; if you’re a tech company, instead of screwing up your candidate filtering yourself, you pay Triplebyte to screw it up for you. Their interview process relies on 2000s-style “do you have these specific algorithms memorized?” questions. They ALSO have a section where they watch you write some code, and then give you a buggy application and ask you to fix it, but if you pass that part and fail the arbitrary memorization challenge you still fail the overall interview.
That’s all subjective – the really damning bit is that those three attempts were each about a year and a half apart, and the test process was word-for-word, byte-for-byte identical between each attempt. They didn’t even ask me to fix a different set of bugs in the test application. They’re making absolutely no effort to improve over time at literally the entire point of their company, and if someone cared enough to game their system it’d be utterly trivial and require zero programming ability.
I wish I had enough startup capital to eat their lunch.
How would you eat their lunch, and why does your plan need startup capital? (Serious question – this is a big graveyard-of-empires problem that’s eaten plenty of attempts alive.)
Presumably by starting a competitor that’s better.
Yeah, the biggest obstacle would be advertising. I could get all the technological parts of the business done single-handedly in a few months, and conduct the interviews myself to start with. Getting my company’s name in front of competent programmers looking for jobs… probably doable with heavy advertising spend. The hard part is going to be getting the kind of people who are able to make the decision to use my service to trust me.
I’d imagine that sort of thing to be HEAVILY biased towards the first company to make a serious effort at it; no-one who already knows about Triplebyte and is interested in their services is going to be looking further for an alternative; if Triplebyte does a crappy job, they’ll just conclude that outsourcing hiring is a bad idea entirely.
My current employer has so much unpaid technical debt that everything they do takes 40x as long (== 40x the cost) as it should, but they get away with it because their biggest asset isn’t the software, it’s the personal relationships between their sales and project managers and the people who actually make the decisions at their client companies.
This kind of just sounds like starting a technical recruiting firm.
Graveyard of empires, dude.
It seems reasonable for them not to take you if you’re not good at inane technical interview questions, because that means you won’t pass the interviews at the companies they refer you to.
The way it was sold to me at least is that I wouldn’t have to pass first-order filtering at the client firm. Would kinda defeat the point if they paid Triplebyte to bin candidates for them and then wasted an engineer’s time watching them do fizzbuzz anyway.
Second order filtering is just more of the same, but lengthy and grueling.
Agree with eremetic. If Company X wants to hire people who know about algorithms, and TripleByte is performing a screen on behalf of Company X, then TripleByte is going to have to ask you algorithms questions if they want to be able to predict whether you will pass Company X’s onsite–even if TripleByte privately thinks that algorithms questions are silly.
So you failed the exact same word-for-word, byte-for-byte, identical between each attempt test three times?
That’s the really damning bit.
As one of the remote interviewers: What you describe here just ain’t so. It is absolutely not necessary to do well at, or even not-badly-at, the “what things do you happen to know” section to “pass” the interview. I have done hundreds of interviews and I don’t always know what will count as a pass, but I’ve definitely seen people do well on the practical section and awfully on the question-and-answer and be considered passes, and vice versa.
I did have a lot of concerns about all the people going in to the office much later than seemed safe to me, but I also note that none of the people I talked to thought it was all that concerning at the time. (Which just makes me think *everyone* is crazy, we’ve been staying at home and effectively locked down since a couple weeks ago, despite the first case in our county being yesterday.)
A friend suggested I interview via triplebyte so I did. For some reason, I got tracked into backend, which was weird given that wasn’t my specialty. I’ll admit that I have always been a nervous interviewer and get easily thrown (plus having ADHD really doesn’t help interviewing) and find it hard to recover from that, and video interviews seem to be worse.
So after that, we got me sorted into an iOS interview, which was an even stranger interview. I was asked zero iOS questions so far as I can recall, though I was asked about some stuff about Swift and ObjC. I was however asked things like:
* details about HTTP protocols
* details about OSI layers (below the application layer). Hey, I like the 7-layer burrito, please serve one so I can use it to fuel app development.
* bloom filters, dude, I’m not writing cloud software.
It was that last question that made me realize that, even if I hadn’t been thrown early on in the interview process, I wouldn’t proceed with Triplebyte.
What was even weirder is that even after they sent me the “Dude, nope” email, they continued to send me lists of open positions with company names unredacted. Which I could then go apply for directly with said companies. That was when I realized they were just not worth bothering with.
Correction
From the linked article:
(emphasis added)
That is, they threatened to sue, but Fracassi ignored their threat. That was several days ago, they haven’t sued yet, and his life-saving printing has been very well publicized. Given that, I’m optimistic that they won’t sue at all. In any event, it’s incorrect to say that he’s currently being sued.
Thanks, fixed.
They might not have threatened, even:
https://www.theverge.com/2020/3/17/21184308/coronavirus-italy-medical-3d-print-valves-treatments
and:
The company threatened to sue them for correctly describing the threat as a threat, so they retracted their true statement that the company had threatened them in the first place.
That is some terrible spin you’re trying to put on. Saying something is illegal is not a threat.
What’s the easiest way to calibrate a sublingual thermometer? I’ve been checking my temperature twice a day, but i’m worried that my thermometer is off.
Have another thermometer that supports the range from freezing temperature to boiling. Calibrate this one, by holding into a) boiling water and an ice/water mix. Then compare with your electronic thermometer, if necessary write a table of equivalence readings. Should not be too far off for home use.
All I have is a meat thermometer, which (according to its calibration certificate) isn’t appropriate for human body temperatures. However, I do have an immersion circulator, which can be set to 97.9 F. That should work.
Your meat thermometer’s linearity will likely be fucked around human body temps, especially if it’s a bimetallic design. I would only trust it if you can create a calibration curve with a resolution of 1 degree or less.
I think a lot of digital thermometers have a range rather than the exact precise temperature. I think ours is +/- 0.5 degrees.
I’ve noticed that the inside of my eyelids and the inside of my throat both feel unusually warm when I have a fever. My own breath feels unusually warm in my throat and mouth when I have a fever. This usually starts with temps around 99 degrees, but only when the temperature is due to illness. When my body temps rise naturally for healthy (non-illness-related) reasons, I don’t notice any unusual warmth.
For the boiling point calibration to work, you need to know the boiling point of water at your altitude. It’s not going to be 100°C anywhere but at sea level. Also, a thermometer with such a wide temp range is not necessarily precise enough at the relatively narrow range of human body temps.
Your’re right. Also, the water/ice must pure, no salts or sugars. Still, if OP is stuck with nothing else -? What precision in the body temperature range can be assumed with this method? A rough estimation? ±1°C? ±0.2°C?
https://en.wikipedia.org/wiki/High-altitude_cooking
“For every 500-foot (150 m) increase in elevation, water’s boiling point is lowered by approximately 0.5 °C. At 8,000 feet (2,400 m) in elevation, water boils at just 92 °C (198 °F)”
So you should be able to look up your local elevation and convert. If you know your elevation to within 100 feet, that’s 0.1 C, probably within the accuracy range of a medical thermometer + normal human body noise.
And if you correct for weather (hPa) you can add a tiny improvement.
For what it’s worth, bp can easily vary by 1-2°C due to normal barometric pressure variations as well.
It doesn’t matter if the thermometer is off as long as it is consistent. You should average your temps and then normalize to 98.2 degrees. The look for temp consistently more than 1.8 degrees too high.
That assumes my initial measurements aren’t already in a fevered state.
Different people also have different baseline temperatures, so…
If it’s the electronic type, a good tip is to keep it in even after it beeps. It should keep measuring. Stop when you take it out and the temperature stops increasing. Or just keep it for 2-3 minutes, doubt it needs longer. (5 for a mercury one)
Be advised that your temperature can change significantly throughout the day, so you should always take your readings at the same time each day.
And not right after exercise.
Some nifty interactive visualizations on Covid:
http://gabgoh.github.io/COVID/index.html
https://alhill.shinyapps.io/COVID19seir/
https://meltingasphalt.com/interactive/outbreak/
And a visualization I made: https://www.reddit.com/r/dataisbeautiful/comments/fkrzw0/oc_covid19_vs_smallpox_epidemic_behavior_based_on/
One of mine http://hamishtodd1.github.io/interactiveEpidemeology/index.html
I’ve updated my tracker to allow you to choose if you want use the log scale on the y-axis or not. I’ve also enabled scaling rates of confirmed cases and deaths by state population. The latter option shows distinctly how much of an outlier Washington State is right now.
https://mavery.shinyapps.io/sars-cov-2-usa-by-state/
https://meltingasphalt.com/interactive/outbreak/
I played with this one. And the weird thing is, I couldn’t really change the death rate much on the last simulation by reducing the number of contacts and travel radius.
Default: 15 enc/day, travel radius 15, transmission rate 0.4: 6% dead
Cut to 6 enc/day, travel radius 6/day, transmission rate 0.38: 6% dead
A transmission rate of 0.3 means 5% dead.