
[This is an entry to the Adversarial Collaboration Contest by flame7926 and a_reader.]
[Content note: suicide, depression, transphobia, self-harm]
Transgender childhood transition is a hotly debated topic, with extensive media coverage devoted to it in recent years. (pro: BBC, The Lancet and The New York Times ; contra: The Cut, New Statesman and The Globe and Mail). We see plenty of stories of transgender children (or gender dysphoric children and gender nonconforming children), both in the media and in the blogosphere. As early as 2 or 3, defying the expectations of their family, those children show a persistent and insistent preference for many things associated with the other sex: little boys want long hair and love dresses, Barbie dolls, Disney princesses and mermaids; little girls, instead, dislike stereotypically feminine activities and prefer rough and tumble play, refuse to wear dresses and insist to have their hair shorter and shorter.
Sometimes, from the very beginning, the toddler corrects the parents: “I’m a boy /girl!”, but more frequently cross-gender behavior is more prevalent. This is only sometimes followed with the child expressing preferences that would be termed gender dysphoria. The child (born and currently living as a as one sex) says to their parents something like “God made a mistake” or “something went wrong in Mommy’s tummy” because he should have been a girl, not a boy (or the other way around). The worried parents search information on the internet and seek out the advice of an expert. There, they usually find one or both of these contradicting opinions:
Gender-affirming approach
Listen to your child – he/she knows best his/her gender. Let your child be his/her true self. It’s your responsibility as a parent to support your child in all stages of his/her transition: social transition now, puberty blockers at the beginning of puberty, cross-sex hormones in adolescence, surgery at 18. To oppose it is child abuse. Transphobia costs lives: 41% of transgenders attempt suicide. Do you prefer a happy daughter or a dead son?
Or:
Therapeutic approach
Your child is just confused. He/she is too young to understand gender and to take such important decision. 80% of gender nonconforming children desist. You, as a parent, have the responsibility to correct his/her wrong behavior. If you tolerate it, gender dysphoria will be reinforced by repetition and persist to adulthood. To encourage your child’s delusion is child abuse. Transgenders individuals face lifelong struggle and often suffer from poor mental health: 41% of transgenders attempt suicide. Do you really want that for your son, when he could instead come to accept the body he was born with?
The first approach is promoted by transgender activists, the second by the conservative media, but both are supported by some experts. The “Gender-affirming approach” is supported by the Dutch team from the Gender Clinic at VU Medical Centre, Amsterdam, who elaborated the typical transition treatment for minors, with puberty blockers at 12 and cross-sex hormones at 16, and, in the US, by Kristina Olson and others from the TransYouth Project. The “Therapeutic approach” is supported by Kenneth Zucker and his team from the Gender Identity Service at Centre for Addiction and Mental Health, Toronto, and, in the US, by Paul McHugh at Johns Hopkins University School of Medicine. There are also experts such as Debra Soh, once a gender nonconforming girl herself, that advise parents to wait and see until adolescence, because in many cases gender dysphoria desists spontaneously, without intervention.
Who to believe when the experts disagree? Let’s see the evidence.
What is Gender Dysphoria/Gender Identity Disorder?
Children labeled transgender are usually diagnosed with Gender Dysphoria (as per the DSM-V), previously known as Gender Identity Disorder (in DSM-III through DSM-IV-TR). DSM refers to the Diagnostic and Statistical Manual of Mental Disorders published by the American Psychiatric Association – DSM-III was published in 1980, with a revision in 1987, DSM-IV published in 1994, with a revision in 2000, and DSM-V coming out in 2013.
According to the APA as per DSM-V, “gender nonconformity is not in itself a mental disorder. The critical element of gender dysphoria is the presence of clinically significant distress associated with the condition”. Both Gender Identity Disorder and Gender Dysphoria include a desire to be or insistence that they are a gender that does not match their biological sex. This desire has to be strong and persistent and is usually accompanied by a preference for clothing of the opposite gender, cross-gender toys, games, and stereotypical activities, as well as the assumption of cross-gender roles in play. It may be accompanied by a discomfort or dislike of their current sexual anatomy and a desire for the sexual anatomy of the opposite sex. GID was said to “cause clinically significant distress or impairment in social, occupational, or other important areas of functioning”, while GD is merely “associated with” similar distress or impairments.
Gender and Sex Difference
Transgender refers to an individual gender identity that doesn’t correspond to the sex or gender they were born with, while gender dysphoria is a psychiatric diagnosis that refers discomfort with one’s physical or assigned gender. Individuals can have or previously have had gender dysphoria without identifying as transgender, while the most (but not all) transgender individuals should fall under the gender dysphoric label according to experts.
Based on the balance of the evidence, both social transitioning and puberty blockers should be approached with caution. There is moderate evidence that social transitioning improves mental health outcomes, and from a perspective concerned with validation of trans-identities it is important. But there are few studies on the long-term effects of social transitioning on rates of persistence and desistence (the number of children who remain gender dysphoric as they age).1 Similarly, puberty blockers may have negative physical health consequences, including an effect on bone-density, though a positive effect on mental health. Still, these choices should be made by families in consultation with experts. Individuals should develop a position on the topic with full awareness of the evidence and taking into consideration their preexisting biases and exposure to social norms on the topic.
Gender Identity Disorder and Gender Dysphoria in Youth
Gender dysphoria in youth is uncommon, with estimated prevalence of around 1%. Acceptance of transgender individuals is relatively low, with 30% of Americans saying they hold somewhat unfavorable or very unfavorable views of transgender individuals. 41% of parents also would be either “very” or “somewhat” upset if their child was transgender. Due to the lack of acceptance of gender dysphoric behavior and identities, it is possible that many gender dysphoric youth go unaccounted for. Gender dysphoria also doesn’t have a perfect overlap with being transgender, as some children feel uncomfortable with the gender that corresponds to their biological sex but don’t necessarily identify as the other gender.
According to Zucker et al. (1993), in a gender identity interview for children, when asked if they are a boy/girl, most (79 out of 85 gender nonconforming children) respond with their biological sex and not the other gender. Yet 30 out of 85 say they sometimes feel more like a boy than a girl (or reverse). Gender dysphoria is associated with feelings that their biological sex is not correct but is not perfectly correlated with such feelings.
According to the APA, treatment options for gender dysphoria include, “counseling, cross-sex hormones, puberty suppression and gender reassignment surgery.”
Desistence
Desisting is the term used to refer to children and youth who previously expressed gender nonconformity (as defined by the gender dysphoria/gender identity disorder diagnosis within various editions of the DSM manual) and are no longer gender dysphoric.
Brief disclaimer – Desistence is a fraught term and has been used to “denote the cessation of offensive or antisocial behavior“. It is difficult to extract the term from its historical context of use in which a transgender life was deemed a less preferred outcome. Yet it is relevant to the discussion and is the term used in papers which study the topic and thus we will use it here, aware of its potentially problematic implications.
The existence of desisting as a concept is debated by some who say that it diminishes the validity of transgender youth identities by painting dysphoric gender feelings as a choice or a phase that one may grow out of – while others claim flawed methodologies in studies purporting high numbers of desisting youth. (Julia Serano, Temple Newhook et al. (2018)). Yet it remains hard to deny that some fraction of individuals who previously expressed these feelings as youth do not anymore as adults.
Desistence matters because any recommendation for gender dysphoric youth, whether it be social transitioning, puberty blockers, or other treatment, may affect those who end up desisting from their dysphoria as well as those for whom the dysphoria persists.
Additionally, papers such as Temple Newhook et al. (2018) and Olson (2015) argue against the narrative of transgender childhood desistance (including the commonly cited figure that 80% of children desist), claiming methodological errors in the original studies. They argue that these studies (including Steensma et al. (2011 and 2013), Drummond et al. (2008), and Wallien and Cohen-Kettenis (2008) – all discussed below) conflate gender non-conforming children and truly gender dysphoric and transgender children. While most of these studies include samples that have both threshold (GD or GID diagnosis) and subthreshold children, the results are separable by diagnosis. These papers additionally critique the Steensma et al. and Wallien and Cohen-Kettenis studies for including non-respondents among desisters, but this is again separable in data analysis.
Temple Newhook et al. (2018) continue to point out that many of the children involved in the studies, (at the Amsterdam and Toronto clinics) were enrolled in programs to reduce likelihood of GD persistence, or at least not supported socially in expressing their identities – and that these were in and of themselves interventions which could affect results. Yet as Zucker (2018) contends, there is no neutral way to approach transgender youth – everything may affect persistence and desistence rates.
We acknowledge these criticisms of the body of research on gender dysphoric desistance, which, while weakening the strength of the evidence, does not invalidate it. Some children who express a range of desires that can be seen as comprising a transgender identity (up to and including identifying as the other gender) do not continue to hold this identity as they pass through puberty.
Many of these individuals who do not continue to feel gender dysphoria do identify as homosexual or bisexual. According to one study, half of the boys in the desisting sample were homosexual or bisexual, while 24% of a total sample of gender dysphoric youth (both threshold and subthreshold) were bisexual or homosexual in behavior.
Desistence Statistics
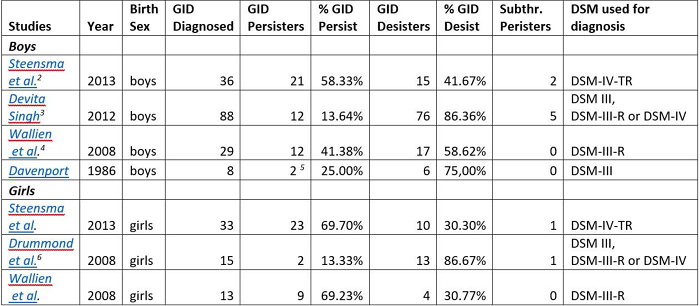
Statistical evidence supports the case that somewhere close to or above 50% of children with GID or GD diagnoses subsequently desist and do not express these feelings past puberty. To respond to criticisms of these studies, we differentiate between those diagnosed with GID or GD (see table above) and those who express gender-nonconforming behaviors but are subthreshold according to the diagnosis. All studies found at least 30-40% of diagnosed children desist, with the percentage as low as 30% in natal girls and 41% in natal boys in the Dutch studies (not counting non-responders), but as high as 75-86% in an unpublished thesis (Singh 2012) and 2 small studies (Drummond et al. 2008, Davenport 1986).
Steensma et al. included a sample of 80 youths formerly diagnosed with GID as children at the Amsterdam gender clinic. Of these formerly GID children, 58.3% persisted of (biological) males persisted past childhood, excluding both non-responses and responses by parents. 69.3% of females persisted past childhood. If non-responses are included (and Steensma et al. make an argument that they should count as desisters since the clinic in question is the only gender and sexual identity clinic in the Netherlands), then 48.5% of males persisted and 62.2% of females persisted.
While the most cautious estimate of desistance figures from this data is 41.7% of males and 30.7% of females, this is still a substantial number of children who previously had exhibited full GID traits who ceased to at some point before adulthood.
Wallien and Cohen-Kettenis (2008) examined a sample of 77 children, with 58 of them formerly GID and 19 subthreshold. 21 of these children persisted and 33 desisted, with 23 non-responses. If only GID children are included, then 50% of the individual male respondents persisted and 50% desisted, while for females 75% persisted and 25% desisted. If parental responses are included as well then the desisting percentages are 59% for males and 41% for females.
This study adds to the body of evidence that a not insignificant number of children with full GID diagnoses who respond to the questionnaire do desist from these feelings at a later point.
Drummond et al. (2008) examined 25 gender non-conforming girls, including 15 girls with GID diagnoses and 10 that were subthreshold. At follow-up (mean age of 23.24 years), three of them still had gender dysphoria. Two of these were from the fifteen girls with a GID diagnosis, giving a desistance rate of 86.6%. Singh’s unpublished thesis (2012) echoes these results, with 76 out of 88 formerly GID participants at follow up having desisted, for a rate of 86.4%.
Though Drummond et al.’s small sample size and the unpublished nature of Singh’s work provide limitations for the interpretability of these two studies, the low percentage of persisters among their results do provide some force to their evidence.
Some additional studies from before 2000 yield similar results with small (less than 20) sample sizes, including Davenport (1986), Zuger (1978), and Lebowitz (1972). While the applicability of these studies is diminished because of the length of time that has passed since their creation and the changes in understanding of gender and sexuality since then, they do still provide some evidence that children’s gender identities change as they age.
Overall, it is clear that at least 25% of children with GID diagnoses desisted, and probably closer to/upwards of 50%. These are not insubstantial numbers of children who previously experience a great deal of distress at their natal sex and do not anymore.
Qualitative research also provides important information about desisters, and particularly on differentiating factors between those who will desist from their gender dysphoria from those who will persist in it and/or eventually undergo sex-reassignment treatment. This research indicates that children who persist generally have stronger gender dysphoric feelings to begin with, including a stronger aversion to their physical anatomy and more insistent they were the other sex as opposed to only wishing they were. For example, “The persisters explicitly indicated they felt they were the other sex, [while] the desisters indicated that they identified as a girlish boy or a boyish girl who only wished they were the other sex”.
Puberty additionally proved decisive for both desisters and persisters, as it was the time when their gender dysphoric feelings either weakened or intensified. Singh (2012) adds that differences in DSM criteria for children as opposed to adolescents and adults for GID/GD may lead to diagnoses of some children who are not what would be considered gender dysphoric in adulthood. Wallien and Cohen-Kettenis additionally differentiate persisters from desisters by their GIIC and GIQC scores (two questionnaires about gender non-conforming behavior and identity) with persisters on average having significantly higher scores according to these measures.
Yet, neither the strength of cross-gender feelings nor a GID/GD diagnosis are perfect indicators of whether individuals will later identify as transgender or not, as even some subthreshold children persist and are transgender (8.7% of males and 4.2% of females, according to Steensma et al. (2013)). Thus, some differentiating factors are identified such as the strength of gender dysphoria, a gender dysphoria diagnosis, and actual feelings of being the other sex rather than simply wishing one is, but for the most part it is difficult to tell which children will continue feeling gender dysphoric as they pass through puberty into adulthood.
Narratives of Desisting
Nonetheless, there are a wide variety of examples of children who previously expressed varying degrees of gender dysphoric feelings and do not anymore. These children range from those who simply had cross-gender preferences in toys or play to those who felt they were the other gender, and even to those who began cross-sex hormones.
Some children express feelings of gender dysphoria when very young and the strength of these feelings lessen as they grow older. One such case is C.J., who used to draw himself as a girl. He played with dolls and liked “pink, purple and princesses”. At 4, he said he was going to be a woman when he grew up. At 6, he asked his parents to call him Rebecca and “her” (but after a while renounced, not feeling comfortable). Some professionals advised his mother to transition him socially, but the mother trusted her “mom guts” more. Now, at 11, C.J. writes “I feel like I’m a different type of boy. But I’m a boy for sure.” and when a friend transitioned he said he “couldn’t imagine being a girl every day“. “I do remember wanting to be a girl if I think about it really hard,” he adds, “but I don’t want to be a girl anymore”. Although still visibly gender nonconforming – or gender creative, as his mother prefers to say – the child grew into a more fluid identity in a way in which he became more accepting of the gender that corresponds with his natal sex.
Some other children express various degrees of gender dysphoria and then unexpectedly desist during puberty. Among these people is neuroscientist Debra Soh, who as a child was strongly opposed to feminine pastimes and playmates, and even urinary positions. Yet when she reached her late teens, “the idea of appearing feminine no longer repulsed [her]“. Even the strongest feelings of dysphoria can sometimes subside: in a BBC documentary, “Transgender Kids: Who Knows Best“, a girl named Alex remembers that she “wanted to be a boy” in childhood, while her father remembers her screaming “I’m a boy! I’m a boy!” Now she feels like a regular girl and presents in a feminine manner. The change happened at 12. In rare cases, it can happen even after social transition: Susie Green, chair of the UK transgender charity Mermaids, reports a second-hand account of the son of the former Mermaids chair, who “lived as a girl for three years… [then] when he realised that he was not female, he simply changed back.” For these children, the time and changes associated with puberty seem to be a deciding factor in whether they will desist or persist with their gender dysphoria. Their feelings were lengthy and lasting, yet changed as they reached and passed through puberty.
The most unusual case is that of an Australian boy named Patrick Mitchell, who was diagnosed at 12 with gender dysphoria. According to an Australian news site, Mitchell was, “Increasingly unhappy, suffering panic attacks and verging on depression, he told [his mother] if he could not go on puberty blockers he would run away and get them himself, or kill himself.” He took puberty blockers, then switched to estrogen (prescribed to his mother, because he was too young to obtain it legally) and started to grow breasts. But at 14, he changed his mind when he began to socially transition: “Teachers at school began to refer to him as a girl which triggered Mitchell to question if he had made the right decision”. This is another instance where puberty plays a role in determining what sex an individual feels comfortable as, physically.
Overall, these narratives show that gender identity is sometimes fluid and remains fluid through adolescence. Children may at one point be adamant they are the gender of their non-natal sex, yet later identify as the gender of their natal sex. Yet this does not give us reason to doubt these children’s’ sincerity or the validity of their identities at any point – but simply recognize that they can possibly change in the future, through no choice of the child.
Mental health and Social Transitioning
One of the primary factors in favor of increased support and validation for transgender children (which can include social transitioning and agentive decision making regarding puberty blockers) is the extent of mental health issues faced by children, youth, and adolescents with gender dysphoria. This includes an elevated risk of suicide, anxiety, and depression for transgender youth and adults. Additionally, sex reassignment doesn’t alleviate all negative mental health associations of transgender identities. Yet there is also a growing body of evidence showing that increased family support and allowing social transitioning does have mental health benefits, though the strength of these is up for debate.
Rates of depressive and anxiety symptoms are elevated among the transgender community, with 51.4% of women and 48.3% of men having depressive symptoms, and 40.4% of women and 47.5% of men having anxiety symptoms [sample size 351] (Budge et al. 2013). Grossman and D’Augelli (2007) additionally found that out of 55 transgender youth (ages 15-21), 45% had suicidal ideations and 26% had a history of life-threatening behaviors. Children diagnosed with Gender Identity Disorder also had a significantly higher rate of anxiety according to reported negative emotions and skin conductance level (though not in cortisol or heart rate) – a sample which included 25 GID children and 25 age-similar controls from the Netherlands of which 36% of the GID children reached a clinical threshold for internalizing problems. Finally, Haas et al. (2014) found that out of over 6000 transgender and gender non-conforming respondents, there was a suicide attempt rate of 41% against a population average of 4.6% – and over a dozen surveys found between 25% and 43% suicide attempts among the trans community.
There is additionally evidence that sex reassignment doesn’t alleviate all negative mental health associations of transgender identities. (Dhenje et al. 2011). Out of a sample of 324 sex reassigned persons in Sweden, there were significantly higher than rates of mortality, suicide, and psychiatric morbidity among transsexual individuals than among the general population.
Social Transitioning
Social transitioning (presenting socially as the gender of your non-natal sex, including using different pronouns, dressing differently, and appearing as the opposite gender) has been proposed by some (including Olson et al. 2016 in Pediatrics) researchers and therapists as a means of addressing the gender dysphoric desires of children with gender dysphoria. Many children express a desire to be or present as the other gender. Validating these desires and allowing them to present as the gender of their non-natal sex may help them feel more comfortable in their body.
Yet others including leading childhood gender dysphoria researchers (see Zucker 2018) believe that social transitioning may increase the chance that gender dysphoric feelings persist into adulthood. Given that gender dysphoria is associated with uncomfortableness with one’s body as well as anxiety, depression and an increased rate of suicide, some posit that on the whole it would be better if children lost these feelings as they grew older. Others claim that a preference for desistence is transphobic and reminiscent of conversion camps and other psychotherapy methods that attempt to erase gay and trans identities.
There is a lack of evidence for the long-term effects of social transitioning. According to the studies on mental health though, family support and affirmation of identities can decrease the risk of mental health problems in gender dysphoric and transgender youth and adults. For example, social support and transition status decreased anxiety and depression, while transition status was negatively related with the same. Suicide attempters have reported more physical and verbal abuse from parents, while strong family relationships decreased the suicide rate (from above 50% with less contact and acceptance from family to 33% when family relationships remain strong). Olson et al. (2016) additionally found that social transitioning for children (73 sample size with two controls) led to them having typical rates of depression with only slightly elevated rates of anxiety – though these were measured through a parent proxy questionnaire. A similar study on trans children using age-similar and sibling controls found that when socially transitioned, they had normal rates of depression and only slightly elevated rates of anxiety – which differs from results found with non-socially transitioned trans youth.
There is no evidence yet that social transitioning increases the rate that gender dysphoria persists or desists.
Children are often the driving force behind social transitions, though the extent to which the possibility of social transition is considered in the first place is affected by family support and media exposure is debatable. For example, one mom reports that, “when he was six and asked us to call him by a girl’s name and use female pronouns.” An eight-year-old child took the initiative and, “sent an email to everyone at her primary school saying she was a girl trapped inside a boy’s body. After that, she started going to school dressed as a girl.”
Even as young as kindergarten, children are expressing desires that they are the other gender and would like to be identified as such. One parent tells a story of their child lining up for class: “That morning, they’d divided the kindergartners into two lines, boys and girls – and Coy had lined up with the girls. “You’re a boy,” the teacher had corrected. Coy had sobbed for the rest of the day. Even my teacher doesn’t know I’m a girl!” he wailed.” A three-year-old child expressed the idea that they, “[were] supposed to be born a girl, but [were] born a boy instead“. This child subsequently wanted to switch pronouns and change their name around a year later. These narratives support the idea that children do know and can express their desires regarding social transitioning (though these desires may change later).
There is additionally some evidence that social transitioning can serve as a tool to differentiate individuals on the strength of their cross-gender identity. For instance, one anecdotal account from a mother indicates that a child has expressed transgender desires and decided to socially transition and was supported in this decision, but didn’t feel comfortable as the opposite gender and transitioned back.
One argument against social transition is that some children find it difficult to transition back to presenting as the gender corresponding to their natal sex. Though this varies based on the individual situation (see desistance narratives for examples of children who had minimal issue transitioning back), Steensma et al. (2011) found that some girls, who were almost (but not even entirely) living as boys in their childhood years, experienced great trouble when they wanted to return to the female gender role”.
Overall, the evidence concerning social transition is mixed, with medium sized positive mental health effects present, but unknown consequences on the child’s future gender identity and dysphoric feelings as well as possible difficulty transitioning back.
Social Constructions of Gender and Samoa
Evidence of better outcomes for those with larger amounts of social support may indicate that mental health problems (primarily anxiety, depression, and increased risk of suicide) associated with transgender and gender dysphoric individuals are more due to society’s treatment of transgender individuals than due to gender dysphoria itself.
For an example of this theory in action we turn to Samoan culture, where a cross-gender identity (termed fa’afafine) is accepted and treated as normative. This study (Vasey and Bartlett 2007) examined whether Samoans with cross-gender identity (Fa’afafine) experience the same distress about gender identity that individuals in Western locales do. Fa’afafine are men who generally present as feminine and are almost exclusively sexually attracted to other men. The authors say that, “Most self-identify as fa’afafine, not as men. A minority self-identify as women”. They do not identify as gay or homosexual even though they almost exclusively are sexually attracted to other men.
The study examined 53 fa’afafine adults and 51 controls from similar Samoan contexts about their childhood behavior. It asked them whether they recalled, “(1) a strong and persistent cross-gender identification in childhood; (2) a sense of inappropriateness in the male-typical gender role; (3) a discomfort with their sex; or (4) distress associated with any of the above.” Most fa’afafine remember engaging in female-typical behaviors as children and no distress related to this behavior. Many believed they were girls as children and also don’t remember any distress about these feelings. They do remember negative feelings toward male roles and typical male activity as children, while some had negative feelings towards their genitals as children.
According to the authors of the study, we can assume many of children would have had GID as defined by DSM-IV-TR. Yet, these individuals do not remember distress about expressions of cross-gender identity. A small number do remember distress with their genitals. Similarly, fa’afafine do not report higher rates of bullying or victimization due to physical aggression.
This study of another cultural context provides evidence that transgender identity is a cultural-context dependent phenomenon, and that distress (and associated mental health problems) faced by transgender individuals are related to their treatment within society rather than to gender-atypical behavior and identity itself.
Puberty Blockers
Puberty blockers are another aspect of the youth gender transition process which is hotly debated. Adolescents are traditionally prescribed puberty blockers to limit them from going through puberty as their natal sex, as this can make it more difficult to physically transition to the other sex. It can additionally be traumatic for those who undergo puberty while strongly gender dysphoric.
There is some evidence that puberty blockers influence bones in negative ways. One study found that puberty blockers (GnRHa) led to statistically significant decreases in bone turnover during the time period in which they were applied. Another study indicates that bone mineral density is decreased significantly in both transwomen and transmen between the start of GnRHa application and age 22. The study concluded that “either attainment of peak bone mass has been delayed or peak bone mass itself is attenuated“. Clemons et al. (1993) additionally examined the effects of puberty blockers in non-trans instances and concludes they are safe and effective, after which puberty resumes normally. Yet they also point out potential problems regarding bone mineralization. Hruz et al., in a socially conservative publication, also posit risks of increased testicular cancer, obesity, memory loss, height decreases, and androgynous appearances. Overall there do appear to be risks to puberty blockers, and it is up to families to make the best decisions for themselves based on the potential consequences of adopting and not adopting blockers.
Additionally, if puberty is blocked, it cannot be used as a “diagnostic tool”, as Green refers to it. According to some researchers, (Steensma et al. 2011, Zucker 2018, narrative accounts of desistance) puberty is the stage at which many formerly dysphoric youth desist and begin expressing a gender identity in line with their biological sex. Yet others would push back against the use of puberty as a diagnostic tool due to the trauma it can cause to transgender individuals forced to go through puberty as their natal sex.
Narratives of puberty describe traumatic experiences for youth who experience gender dysphoria. If one feels their biological sex is wrong and they should have the opposite physical sex characteristics, those characteristics becoming more prominent can be extremely difficult. Coupled with the additional social pressures during puberty to conform to the gender that matches one’s biological sex, puberty can be difficult and scary for transgender individuals.
For instance, a mother reported her son named Patrick was, “Increasingly unhappy, suffering panic attacks and verging on depression, he told her if he could not go on puberty blockers he would run away and get them himself, or kill himself.” Another mom recalls that her child, Jackie, was “incredibly depressed” when she started puberty. The daughter was happy in elementary school, after social transitioning at 8, but “everything fell to pieces” when she started puberty, making six suicide attempts between the ages of eleven and fifteen. She overdosed and self-harmed with razor blades to distract from her changing body before being prescribed puberty blockers.
Steensma et al.’s (2011) qualitative study reports that, upon reaching puberty, “these anticipated or actual physical changes were often agonizing and highly distressful,” while, “at the beginning of puberty, the aversion towards their bodies intensified immensely, resulting in insecurity and social withdrawal”.
These psychological consequences of commencing puberty as a gender dysphoric child or youth must be weighed against any potential health effects when deciding about puberty blockers. A 2010 study of those placed on puberty blockers also indicates positive mental health effects of puberty blockers. From a T0 at the beginning of puberty blockers to a T1 around three years later, depressive symptoms significantly decreased, while scores on the internalizing problems also significantly decreased (from 29.6% to 11.1%). Trans boys did show still elevated levels of internalizing and externalizing problems but decreases from their previous rates. Overall, “Adolescents showed fewer behavioral and emotional problems, reported fewer depressive symptoms, feelings of anxiety and anger remained stable, and their general functioning improved.”
One other aspect of this study is that out of a sample of 70 individuals, none desisted, and all continued to receive treatment for gender dysphoria. This could possibly indicate that puberty blockers decrease the chance that an individual’s gender dysphoric feelings will go away, though it could also indicate that only those with strong feelings take puberty blockers in the first place.
Overall, puberty blockers appear to have some positive mental health effects due to their prevention of the physical experience of puberty among transgender youth, but may have physical health consequences including on bone growth.
Conclusion
On Desistence – The body of research on gender dysphoric youth indicates that many of these youths are no longer gender dysphoric upon reaching and progressing through puberty. It is possible that the youths that “desisted” either were not transgender in the first place or were pressured to disassociate from their transgender identity. Yet there are enough anecdotal accounts and extended studies regarding desisting youth to provide reasonable evidence that at least some, and likely a sizable fraction of individuals who express desires to be the gender opposite their natal sex or affirm that they are the opposite gender in childhood do not feel the same way at a later point in life.
On Determining Desistence – There is a lack of agreement between sources on whether gender dysphoric youth who will persist and desist can be differentiated from each other. On the whole, the evidence indicates there is a correlation between the strength of transgender expression (identifying as the other gender rather than simply expressing cross-gender behavior) and persistence, yet the correlation isn’t perfect. Some children who express a strong desire that they are the other gender desist, while some children with subthreshold gender dysphoria diagnoses persist through puberty.
On Social Transitioning – Social transitioning has positive mental health effects, but unknown effects on whether children will persist or desist. Social transitioning is put forward as one of the primary ways to support transgender children and is shown to reduce the rates of internalizing problems and anxiety among gender dysphoric youth. These children do still show elevated rates of anxiety. Additionally, some children who socially transition later do not feel gender dysphoric anymore and decide to not present as the opposite gender any longer. There is no evidence examining the rate at which individuals who socially transition retain their gender dysphoric feelings and transgender identities.
On Puberty Blockers – Puberty blockers, though reportedly safe, may have unintended medical consequences based on a review of studies. Studies show effects on bone growth and density. Yet other studies show positive mental health effects relative to transgender individuals who undergo puberty as their birth sex, as puberty is a time when living as a transgender individual can be particularly traumatic. It is unknown if placing individuals on puberty blockers affects the rate at which that population of individuals retains their gender dysphoria.
Notes
-
This does not indicate a preference for desistence of gender dysphoric youth, but merely indicates that these types of long-term effects are something policy makers, medical experts, and trans advocates may wish to consider. ↩
-
Dutch study. The numbers don’t include nonresponders. ↩
-
Ph.D. thesis, University of Toronto. ↩
-
Dutch study. The numbers don’t include nonresponders. ↩
-
1 “Transsexual” and 1 “Homosexual, cross dresses”
-
Canadian study, University of Toronto. ↩
















Great article.
I was surprised that it didn’t discuss hormonal therapy. When I think of the potential dangers of “transitioning”, this is on the top of my list. Social transitioning is, of course, also a huge decision, but it doesn’t really have medical effects, and is reversible. Hormonal therapy and surgery radically changes your body, makes you sterile, and is in general dangerous. The article discussed puberty blockers, which is usually a preamble to hormonal therapy and surgery. Whether or not puberty blockers cause lower bone density seems like a smaller issue than the effects of the following hormone therapy.
I’m also not convinced by the Fa’afafine argument. Apart from the specious claim that this is a different “gender” in any meaningful sense (although the article is careful and calls it a “cross-gender identity”), it is to be expected that Fa’afafine don’t experience the same amount of mental problems as Western transsexuals do. I believe fa’afafine are selected by their parents (?), and would therefore have a base rate of mental problems similar to the general population. Westerners who identify as transsexuals tend to have a range of mental problems, not all of which are likely to be caused by society’s rejection of their gender identity.
But overall, again, great article!
Thank you.
We didn’t mention hormonal therapy because we concentrated on childhood.
The fa’afafine are not selected arbitrarily by their parents. They are former feminine boys:
Source: the paper mentioned in the collaboration:
What Can the Samoan “Fa’afafine” Teach Us about the Western Concept of Gender Identity Disorder in Childhood?
Thanks, that clarifies things for me!
Note that the fa’afafine are estimated to make up 1-5% of the male population; much higher than the rate of transgender people in the West, and in fact closer to the rate of homoesexuals in the West. Also note that homosexual intercourse is a crime in Samoa.
It therefore seems incredibly likely that the kind of people that end up as transgender in the West, is only a small fraction of the people that end up as fa’afafine in Samoa. It further seems likely that many of the fa’afafine would simply identify as homosexuals in the West. Either way, it would be surprising if the base rate of mental illness was as high among the fa’afafine as among Western transsexuals.
It seems to me, that if that 80/20 percent figure is accurate, then the best thing to do would be to concentrate on coming up with good tests to distinguish the 20% from the 80%, and encourage the 80% to continue behaving as they wish for as long as they like, but to hold off on performing any permanent alterations to their physiology until they are more absolutely certain, and to do everything we possibly can to help the 20% correct their horrible birth defect of having been born in the wrong body.
I don’t see why it has to be one or the other, all the way.
ETA: It obviously doesn’t matter what the ratio is. 80/20, 50/50, 20/80, the important bit is to identify the people who truly will be happier transitioning, and providing them with that treatment option, and separating out the people who will be happier overall if they don’t transition, and suggesting that they don’t.
I have to preface this first with: I am 100% serious in this comment. I’m not trying to be funny, nor offer some modern Modest Proposal.
Children should be allowed to transition as early as they like. Mental illness is *highly* heritable. So children transitioning is a really effective form of negative eugenics with the added benefit that it’s something the ‘patient’ says they want. It really is the perfect solution. I only wish the % of transgender people who decide to transition were higher.
It probably would be, maybe as much as 1%, if other people weren’t so set on making their lives so difficult and making treatment so expensive/hard to obtain that it’s out of reach of many who would otherwise seek it out.
What percentage of people actually currently ends up producing genetic offspring? Would it really lead to population failure?
Even if we make totally crazy suppositions, the worst case scenario is that the Amish fill to expand the empty space.
It’s insane that this is even up for debate. Giving kids permanent life-altering drugs because of random whims is child abuse, full stop. If you had castrated me because of some stupid shit I said when I was five, I would want you prosecuted. All it’s going to take is a couple regretful transgendered kids suing their parents to put a stop to all of this.
It’s not that complicated. Leave it to psychologists to avoid seeing reality at all costs. I mean, where do Goth kids come from? Are you born a goth? No? So how does your kid become goth? Obviously, by encountering other goths.
This is just as bad as heinous practices like foot-binding and head-wrapping. History will not look kindly on our civilization for this.
It really isn’t like that, and no child gets castrated at age 5.
http://www.youtube.com/watch?v=YNvTFH0uHHU
For those who are genuinely trans from a young age it really does feel like they have all the wrong parts and are forced to live the wrong life.
Nobody genuinely is a goth, that’s always just an affectation, and way of expressing themselves and pushing boundaries, but transsexualism is a real physical difference in brain formation, and attempting to ignore or suppress it in the long term leads to many far worse psychological/emotional difficulties.
Random whims? Jesus what a load of transphobic garbage. “Leave it to medical professionals to not validate my bigotry”.
… Did we seriously start an article on gender by citing McHugh as an expert? Is anyone reviewing these things before they go up?
We mentioned various experts, from the most favorable to the most opposed. Paul McHugh is a psychiatrist and a psychiatry professor.
https://en.wikipedia.org/wiki/Paul_R._McHugh
And Dr. Oz is an expert on medicine – a legitimately gifted heart surgeon. That lends absolutely no credence to his bizarre ramblings on dietary supplements. McHugh is a psychiatrist who, to my knowledge, has never published anything on gender dysphoria. He hasn’t been active in psychiatry for decades. His views are no longer anywhere near the mainstream, and most recently he got his 15 minutes of fame by lying about the results of a Swedish study into transgender morbidity. Citing him as an expert on gender is entirely unreasonable and a sign that at least one of the participants is badly misinformed – and that that misinformation has not been addressed. Citing him as an expert on the subject now is basically indefensible. Perhaps the better analogy is less “Mehmet Oz” and more “Andrew Wakefield”.
As with all entries, props on putting a ton of work in and producing a neat final product.
As of reading this entry, I was torn between it and the vaccine one as my pick for winner. On the one hand, this entry tackles a more difficult and contentious (I think?) issue, and it seems more exhaustively researched. On the other hand, I really appreciated how the vaccine entry hashed out the nature of the disagreement, tried to paint a picture of what the various positions depend on, and made clear how the collaborators’ viewpoints changed. This one is very much in the just-the-facts style of a “literature review”. That’s worthwhile, of course, but to me it doesn’t really get to the stuff that’s most valuable in adversarial collaboration.
After writing that out… I think the education entry is actually better than this one along the “just the research, don’t look at us for substantive conclusions” axis. So for me it’s between that and the vaccines entry, which admittedly has its flaws content-wise, but aligns better structurally with what I think an adversarial collaboration should be.
They presumably have never been given GnRH agonists, as that’s a technique that’s only recently been used for this purpose, and presumably the chances of having a form of vaginoplasty were pretty remote in poor communities and the surgical techniques are pretty recent, but some form of castration has been widely practised for the gender-divergent community in many different societies.
https://www.npr.org/sections/parallels/2014/04/18/304548675/a-journey-of-pain-and-beauty-on-becoming-transgender-in-india
https://en.wikipedia.org/wiki/Two-spirit
There are stories of people riding bare-back for days in order to crush the testicles.
Castration clearly amounts to low-tech hormonal intervention, or at least achieves some of the same ends.
Presumably castration is considered a ‘last resort’ irreversible treatment by western medicine, while GnRH agonists are supposed to be pretty harmless and cross-sex HRT can be ceased and reversed albeit with substantial permanent side-effects which might require surgery to fix-up as best possible. Castration leads to total-sterility and probably also sexual-dysfunction, I guess.
Regarding the Samoa case, do Fa’afafine people typically undergo surgery or hormone therapy? It sounds like they don’t, which, if they’re actually “happy”, would seem to suggest that either
1) These people are actually fundamentally different than people with GID/GD in the West, or
2) People with GID/GD can be perfectly OK without hormonal/surgical intervention, as long as they’re sufficiently accepted socially
No?
Are there differing rates of MtF and FtM GD? My subjective impression is that MtF is more common, but that could just be an artifact of social media. If there are differing rates, is there a proposed explanation?
Yes, there are more boys than girls referred to clinics for gender nonconforming behavior – but that may be because society is more tolerant to gender nonconformity in girls (tomboys).
The arguments go that:
For) Anyone who thinks that they might be ‘trans’ probably is, and it should be up to them what they want to do with their own bodies, regarding their fertility, bone density, and future sexual capacity. Therefore a couple of sessions with an informed-consent practitioner should be all that is required to go over the issues involved and the medical establishment shouldn’t treat it like a pathological condition that has to be minimised.
Against) Nobody is ‘trans’, the whole concept is flawed based on nebulous feelings and not material science, and therefore such psychologically deluded people should not be given any bio-medical treatments, by anyone. Anyone that has actually transitioned was just being enabled and very likely now regrets it but is too scared to admit it.
I think both these positions – Anyone who ever thinks vs. Nobody – are rather extreme.
Isn’t this really a semantic argument where “Desistance” is used instead of “Type 1 Error”?
For some odd reason the terms “Type 1 Error” and “Type 2 Error” don’t seem to pop up much, if at all. Those terms are nowhere in this thread, for example.
But isn’t that all this is? Most of these folks seem to agree (I think) that trans status is mostly genetic. In that case:
1) Some people are trans.
2) The current test (the decision by which we classify a youth as ‘trans’ or ‘not trans’ is subject to error.
3) If it classifies a not-trans person as “trans”, that’s Type 1 error and the person is thereby subjected to inappropriate treatment.
4) If it classifies a trans person as “not trans,” that’s Type 2 Error and the person is denied appropriate treatment.
This all seems to be a strange semantic game. Nobody can credibly argue that the test for trans status is 100% accurate w/r/t classifications. So why all the arguments about “desistance” rather than simply acknowledging that there’s some error?
So when someone said
That is a test failure suggesting we are testing too early.
Those are diagnosises of Gender Dysphoria / Gender Identity Disorder in Childhood, not of being trans forever. If a little girl screams “I’m a boy! I’m a boy!” (besides wanting her hair short and other boyish things), that child has GD/GID now, regardless of how she/he will change or not 10 years later.
I don’t agree. Probably genes have some influence, but they can’t be decisive factor – otherwise cases like this wouldn’t be possible:
How Identical Twin Boys Became Brother and Sister: One Family s Courageous Transgender Story
Then perhaps it’s a Type I Error of diagnosing future GD/GID?
The trouble is that puberty blockers and gender surgery basically make you trans forever (nearly 100% of puberty blocker users continue to transition), regardless of whether your GD/GID would have self resolved during/after puberty. You can’t say “we have no Type I Errors in that group” because blocking puberty and pumping you full of gendered hormones is pretty effective at making you feel like that gender regardless of what your “natural” gender would be.
Isn’t that what the famous David Reimer case actually disproved?
He was surgically castrated, which would have blocked puberty, told that he was a girl all his life, and treated with female hormones, and yet his forced gender reassignment still didn’t ‘take’, and he reverted to presenting as male as soon as he was told the truth.
It isn’t something that can be imposed on you, even with social transition and hormones, it comes out of deep within the subconscious.
To be specific, we know that it couldn’t be imposed on David Reimer. We have no idea whether it’s been imposed on other people, because they would be indistinguishable from people who would have been unhappy apart from transitioning.
Note that I said nearly 100%. I’m basically answering the claims that “almost nobody desists after going on puberty blockers, therefore Type I errors are very rare”. This was an argument raised earlier to dispute / counter the claims of 30%+ desistence.
I remember just one case of a kid who desisted after taking puberty blockers: an Australian named Patrick Mitchell. But he wasn’t on puberty blockers when he desisted, he was on estrogen.
He was diagnosed with GD at 12 and started puberty blockers (was depressed and suicidal before), but because he was growing too tall, his mother, afraid he won’t pass, thought to give him estrogen prescribed to her (because he was too young to be prescribed sex change hormones). He took estrogen for a while, started to grow breasts, but unexpectedly, at 14, announced he no more wanted to be a girl.
I suppose it was maybe because, then, he wasn’t taking anything to stop testosterone production, so his own testosterone had more impact than the estrogen.
Reimer never got hormones. When he reached the age of puberty, and was to get hormones, there had to be an explanation. His mother broke down and told him the truth, at which point he said “I’m not crazy! I really am a boy!” and totally refused any cooperation with the gender-change progrsm.
Most of the sources I’ve seen say that David Reimer was actually started on cross-gender HRT during puberty,
though mostly against his expressed wishes.
https://embryo.asu.edu/pages/david-reimer-and-john-money-gender-reassignment-controversy-johnjoan-case
It’s covered in much more detail in the book ‘As Nature Made Him: The Boy Who Was Raised A Girl’
https://www.amazon.co.uk/gp/product/B00AXXUB2G/
He was given the estradiol pills from the age of 12, his parents making sure he actually swallowed them, and they didn’t finally tell him the truth about his birth until he was 15.
It seems pretty clear to me that error is expensive, no matter what type. If someone is trans and you deny them treatment, they’ll be miserable and it will be much more difficult for them to transition. If someone is not trans and you give them treatment, they’ll be miserable and you’ll need to try to reverse a transition. The cost of error is HUGE compared with the cost of diagnosis, right?
So with that in mind, I am surprised that there are people who appear to want to avoid relatively minor diagnostic harms like “talk to someone for ten hours and answer some intrusive questions”
In any case, I think that traditional error issues make a good starting point. No matter what we do, there are going to be some kids who are misdiagnosed on either side. Can’t we talk about the relative costs and odds ratios and try to aim for an appropriate one?
The pro-trans folks seem to be stuck in the SOCIAL argument, in which only the views of the oppressed matter. (For example, in the social pro-trans argument you ignore a lot of low-level distributed costs. So you would never even consider the aggregate social cost of every cis individual relearning pronouns, because it is overridden by issues of social justice and oppression.)
But in the SCIENTIFIC argument you absolutely need to consider the cost and frequency of both Type 1 and Type 2 error; you can’t just ignore one of them because of oppression.
Do you count as Type II errors only those who visited gender clinics as children/teens but then ‘desisted’. Coz from a glance around the various trans forums and support groups there seem to be far far more that were never given that opportunity at that kind of an age, even if we had insisted. (Socially it was much tougher and there were far fewer resources available in the 1990s or earlier), and are only coming to grips with it all in their late twenties or thirties or later.
Catch someone at age 17-25 and they may very well claim to have put all that ‘weird trans stuff’ that they felt at a younger age behind them. Catch the same person again at 32 and they may give you a very different story.
Ages 28-31 seem to be a very tough time for a lot of us, too many opportunities already lost, too little remaining to look forward to, too many ties to whatever lives we have managed to establish be it relationships/marriages or career paths.
I am using “trans” as the diagnosis, since cis is much more common as a default.
Someone who is diagnosed as trans and who turns out to be cis is Type 1 error. Someone who is diagnosed as cis and who turns out to be trans is Type 2 error.
I don’t think “visiting a gender clinic” is an issue, since that is probably the appropriate place to do the testing (though I may be wrong.) Nor am I including short-term, reversible, use of hormone blockers: those seem to be the medical equivalent of “take some antibiotics while we figure out what you have”.
An example of a Type 1 error would be someone who actually begins any kind of major transition to the opposite sex (i.e. a biological male taking estrogen and testosterone blockers) who then reverses it (stopping hormones), etc.
Right now, we have what appears to be a fairly inaccurate test (self-diagnosis) which seems to be inclined towards a fair bit of Type 1 error. Balancing that, we also have a fairly high bar to test entry, unless you happen to have ultra-woke parents and live in Northampton or Provincetown.
Making it worse, we also lack a full spectrum of options. Not every non-conforming kid is trans! Some of them are probably butch lesbians, or femme gay guys, or straight crossdressers, or bisexual, or whatever. Some of them have body or self-image issues which aren’t caused by being trans. And so on.
ETA: Of the three highly-nonconforming high school age kids I who pop to mind, all in my local community, the ones who are declared as trans seem to be having an easier time than the one who is not. Both FTM seem to be going swimmingly, and according to my kids, nobody cares. There are a bunch of gay kids, too many to count, including many of their friends; nobody cares at all these days.
But the boy who occasionally shows up in full drag is having a much harder time of it.
Socially, in my community: if you were considering drag versus telling everyone you were trans, you might lean towards the latter.
Trans status is only one of many potential diagnoses. So self-diagnosis as trans, especially by a pubescent kid, seems to be a necessary but not sufficient criteria. If we had a more accurate test, it would lead to less terror of taking your kids in and hopefully would lower the bar for test entry.
In truth, it’s hard to come up with any plan which would simultaneously work for 11 year olds and 40 year olds. I am focusing mostly on how to treat kids going forward; it isn’t that I ignore the plight of older transfolk, but they are a hard group to address.
Great review, thank you guys.
One thing I would like to see is something differentiating the experience of both prepubescently and not for natal men and women.
From an uneducated place, I would think that a natal man who goes through puberty would have a hard time passing as a woman (tall, broad, etc), while a natal woman might have it easier, post surgery. That fits with our conceptions of beauty as well –feminine features on a man are much more accepted than masculine ones on a woman.
How does this play out in the real world? If it’s tougher in one direction than the other, that shifts how you should weigh the risks as a parent
Afaik the early-onset transwomen (the cases discussed here, where dysphoria started in early childhood) passed quite well even when they didn’t use puberty blockers from childhood. See for example Blaire White, a controversial Youtuber, who according to her Wikipedia page transitioned and began taking hormones only at 20 – would you have guessed she was born a man?
J. Michael Bailey, in The Man Who Would Be Queen, says that those early-onset boys transition only if they know they will look good as women, otherwise they prefer to live as gay men, but I think that maybe both the feminity/masculinisation of the body and of the brain depend somewhat on the same sex hormones.
I may be late to the party, but I’m continually shocked that these studies include second-hand account testimony from parents regarding their children’s psychological symptoms as reliable data. Is this normal in psychology/psychiatry? What other fields do this kind of evidence collecting? Maybe I don’t know enough about child psychology, but this seems deeply flawed, methodologically.
Particularly given the hindsight bias – we have a lot of parents of trans children saying years afterwards “oh I remember when my little [natal boy] insisted they should be grouped with the girls in kindergarten” but no idea how common that sort of thing is in children who never get diagnosed with dysphoria.
I was pretty surprised to read that there are basically zero examples of people who have transitioned and who regret it / want to change back, even with people doing so at a young age? To me, that’s pretty compelling evidence that young people who are intent on transitioning should be supported. If the heart of the objection is, maybe it would go away / maybe puberty would make the strong gender dysphoria go away on its own, and also maybe their bones will be less dense, then that doesn’t seem like a reason to deny someone a medical intervention.
Also, some of these comments are pretty hateful/transphobic. Trans youth is not some little boy who likes the color pink and wore a pink dress once when he was 6, so now we’re gonna chop off his johnson. Nor is being transgender some kind of fad like furbies or hula hoops that we have to stop kids from getting too carried away with, or some kind of political agenda being foisted on us by…. the wealthy and powerful queer academy… or whoever your boogeyman of choice is. I was disappointed to see a few such comments, but mostly heartened by the replies from the commentariat here.
Lastly, check out pop star Kim Petras (nee Tim Petras), who underwent exactly these treatments at a young age in Germany (she is sometimes billed as the ‘youngest person ever to transition’ and such, which is almost surely not literally true, but she did get started when she was very young). In addition to catchy music, there are some interviews with her and her family about her youth & transition that I thought put a pretty human face on something that can be pretty abstract if you don’t personally know anyone who is trans.
On the first point, doesn’t the discussion of Steensma et al. in the article regarding issues with “great trouble” among some people in returning to their original gender identities rebut the idea that regretted “transitions” are negligible? I’m forgetting the part of the article you’re referring to but just anecdotally, if one Googles “regret transitioning” one finds plenty of apparent examples.
That’s hardly the only impact. Puberty blockers and hormone treatment will also cause sterility, and state of the art gender reassignment surgery still rarely leaves you fully functional.
And while you hate for bigots to make your decision for you, the prejudice and other negative social impacts of being trans are not to be taken lightly. Plus, even non-transphobes might be uncomfortable or unwilling to be in long term sexual relationships with trans persons given the sterility and dysfunction issues.
It seems like there’s a lot of negatives that ought to make transition a last resort. All told “desisting” seems like an objectively better/less invasive outcome, if it truly clears the dysphoria, and it shouldn’t be considered transphobic to note that. Anymore than it is prejudice against the disabled to avoid amputation except as a last resort.
I don’t really think sterility is a big deal. There are plenty of non-trans people who can reproduce in their place (and plenty who could but choose not to, for a large number of reasons). Not being able to have sex in the same way as everyone else is a bigger deal, even than bone density — I’ll agree — but I feel like also they understand that and accept that consequence? I mean it’s pretty fundamental to the nature of their identity.
The kind of medical side effects that would give me pause would be things like cross-sex hormones having a 5% chance of causing some sort of invariably-fatal endocrine cancer within 20 years. It sounds like basically nobody has found any real non-sexual health consequences of transitioning, which I honestly find pretty surprising. The overtly sexual (reproductive, intercourse, etc) consequences seem built into the concept and are choices that people should be free to make. And who knows what state of the art will be in 10-20 years; biotechnology is ever advancing.
Is it relevant whether or not there is a biological basis for trans identity? Weren’t there some posts on here showing that MRIs produce different results in trans brains? And there seems (perhaps only anecdotally?) to be some sort of genetic component where it’s more common for siblings to be trans (e.g. the Wachowskis). I think, similar to homosexuality, if you view it as a choice whether or not to be trans, then that leads you to a more cautious conclusion about who, if anyone, should transition, and to what extent, and if you view it as a more profound personal truth with biological roots, then it’s really simply a choice of whether and how to express that identity, and what level of support that expression deserves from your fellow man.
To follow up on your last paragraph, would it be an objectively better outcome if a gay man just decided to stop being gay? Certainly less risk of certain infectious diseases, less discrimination. And hey, for some people it is just a phase. I would have a hard time accepting that position is not being homophobic.
And let’s not pretend that the debate about the level of support we provide to trans persons occurs in a vacuum. You’re right that it is harder to be trans in large part because people are jerks to them. Bigots *are* making their decisions for them, and that’s something we change in part by being supportive of trans people’s decisions and their ability to make them.
I agree generally with your last paragraph, but I’m not sure that it provides clear guidance (is anyone arguing that hormone blockers and surgery should be a first resort?). The examples of young children that have expressed a trans gender identity since they could talk and have socially transitioned who are terrified of puberty and threatening (and in some cases, actually inflicting) self-harm – is that not a last resort scenario? How many suicide attempts should we require?
I think most reasonable people would agree that medical transitioning technology is pretty serious and should be gatekept – the question is how difficult to pass through that gatekeeping should be. If 0.5% of the population identifies sufficiently strongly to go in therapy, socially transition, and to seek graduated access to medical transitioning – what proportion should be kept out because they don’t want it bad enough, or aren’t dysmorphic enough? Based on the risks that this collaboration has uncovered, it doesn’t seem like any additional gatekeeping is justified. If you’re willing to come out as trans and put your body through all of that, with all of the stigma and infertility and expense and difficulty finding romantic partners and the like — isn’t that more of a deterrent to making the wrong decision than anything that anyone else could come up with and impose?
“I don’t really think sterility is a big deal. There are plenty of non-trans people who can reproduce in their place”
That’s not how most people see it, and you can see why. Throughout evolutionary history those who wanted to allow others to reproduce in their place were quite able to do so. (Though I should note it’s probably what I’ll end up doing.)
“Not being able to have sex in the same way as everyone else is a bigger deal, even than bone density — I’ll agree — but I feel like also they understand that and accept that consequence? I mean it’s pretty fundamental to the nature of their identity.”
Pre-pubescent children aren’t going to understand it, no. And of the teenagers and adults, I’m sure many of them, surrounded by the culture of wokeness, take it all at face value without understanding how few people are actually willing to date someone who’s transgender, even if they loudly proclaim their willingness to use the right pronoun.
Largely because transitioning is a relatively new thing, and the population that does transition is a very small subpopulation with significant comorbidities. Yet I think what little direct evidence there is shows your claim to be unlikely, and our theoretical priors shouldn’t be weak. Almost all drugs have side effects, and slowing or delaying typical physical (and by obvious extension likely cognitive) development is an extreme intervention.
Anyways, what little do we know? Leuprolide acetate was known to probably decrease bone density from its usage in treating other diseases. I’m not sure if the effect is long term reversible. Likely not a big deal in our modern environment, but may show up as more injuries when older. I’m not sure how the effect of physically transitioning on bone density shows up for MtF and FtM though. I would naively expect that MtF treatment would decrease bone density but FtM treatment would increase bone density.
More significantly, puberty blockers may affect cognitive function. Sample size of 1, but a 10 point drop in Weschler scale IQ is not a normal part of development and is large. It’s the opposite direction IQ normally goes with age. It’s possible the subject of the study is abnormal or will have an increase in IQ later if the IQ drop is somehow transient and recoverable or cognitive development resumes. But maybe not.
Another study on executive functioning shows no difference in executive functioning across subjects (as measured by a game) but has a 15 point difference in IQ between untreated and suppressed MtoF although only an insignificant 3 point difference in FtoM. I apologize if you can’t access the article. The abstract is deceiving with regards to my point, because IQ was not the primary target of the study. The study used measured IQ as a covariate in analyzing MRIs taken while subjects played a game meant to test executive functioning. It’s remarkable how little comment the authors make on the IQ differences though. The IQ differences are almost certainly more meaningful than the differences or lack thereof in fMRIs during a single task. Especially since their method for choosing subjects excluded any gender dysphoric individuals not “functioning within the normal range”.
Unfortunately (or maybe forunately depending on what the effects are), sample sizes of any study I’ve found studying a relationship between puberty blocking and cognitive development, IQ, etc. are small. It shouldn’t be hard in theory to do much larger studies, but I’m not finding them. And the effect of comobordities shouldn’t be ignored.
It should be kept in mind that it may turn out that transitioning MtF has relatively significant side effects but not FtM or vice versa.
For adults that makes sense, but children are terrible at making decisions. On top of that young children (age 12) don’t even have a clue about mating or romance.
These are some fair points; I’d note in rebuttal
1) The N=1 study on the Brazilian young woman was on someone who was already pretty low-IQ to begin with.
2) My brief read of the other study doesn’t seem to me to arrive at the conclusion you’d like it to?
3) I’m all for strong priors and whatever, but the tenor of these responses all seem to be “this is unnatural and wrong and therefore there must be more problems that we just haven’t found yet”. We have some evidence of what the consequences of transitioning, including starting at a young age, age, and the weight of the evidence so far is, not so bad. My question to you is, how many more years of studies and evidence would it take to convince you that this intervention is low-risk/basically harmless (e.g. bone density, not much else of much probability)? What would it take, given your ‘strong priors’? Some of the posters here (and in the subreddit) seem to be foreclosed to that possibility, and so there’s really no point in debating it with them.
(1) A drop from 80 to 70 is probably more damaging than a drop from 100 to 90. This makes things worse, not better. 70 is the cutoff where the supreme court of the US thinks the death penalty becomes cruel and unusual. Going from 80 to 70 is awful. Especially given that normally, IQ would increase with age.
(2) The words the authors use are deceiving, and the abstract especially so. I already specifically mentioned this above because I knew that if someone just skimmed the authors words they wouldn’t understand.
To elaborate, the authors conclude execute functioning is “unaffected” despite enormous IQ drops in MtF on suppression drugs compared to those not on suppressing drugs. They conclude this via MRI scans during a relatively simple task that isn’t nearly as well validated a construct as IQ. And they include IQ as a covariate when making these comparisons, which if I’m not misunderstanding means they’re partly saying there are not significant additional changes after controlling for IQ. You should also keep in mind that in the tables the standard deviation in IQ is not the error in the mean. The error in the mean in the table is roughly 1/3 of the standard deviation. Look at their actual IQ tables if you can.
(3) People have barely been looking for problems yet so it’s important to take prior knowledge and what evidence we have seriously. “Unnatural” isn’t wrong, but our technology is not up to the task being asked of it. “Unnatural” doesn’t have to be taken seriously as a moral argument (I for one, don’t care about unnaturalness in a moral sense; I thank medicine I won’t die naturally of malaria or TB), but the risk of drastic interventions should be taken seriously as an argument in terms of changing biological development. We just aren’t that good at controlling development yet.
We’re using drugs off label in a completely experimental way during a crucial growth phase and just sort of crossing our fingers that nothing goes too wrong. There haven’t been anything like the sort of trials a drug would undergo for FDA approval. The only people who would normally argue for doing something this risky with drugs would be hardcore libertarians. And even then they’d probably have a different calculus for 12 year old children. That a lot of progressives suddenly are gung-ho for probably risky off-label uses and say it’s obviously safe despite evidence to the contrary is… interesting.
You say not so bad. I say a 50% risk of a 10 or 15 point drop in IQ is pretty bad. Just roughly guessing. The best estimate is a bigger risk for MtF and a smaller risk for FtM. Opinions may differ on the severity of this change, and I’d rather not get dragged into argument about why IQ and cognitive function matter. But if I have to, I will.
I could be completely convinced that the intervention is almost harmless (other than sterility and sexual function changes) by a longitudinal study (over a decade or two) with a randomized control group that doesn’t undergo puberty suppression and a randomized treatment group that does, with a multitude of physical and cognitive measurement taken in both groups and shown to have no significant difference or beneficial differences in favor of puberty suppression. I could be convinced that there was less risk (low enough perhaps) by a similar shorter study with the two groups (say over two years) that wasn’t perhaps perfectly controlled, but made some effort to handle confounders.
It’s also likely of course, that a different treatment could have less or less severe side effects. It’s not like a ton of strong controlled research went into developing the best possible transition treatment. But to know what’s best, you have to do studies comparing various treatments to control groups. Maybe you start out on animal models to find candidate treatments. Although generalization will be… weak. And it’s not going to work out well if you don’t admit up front that you can likely do better. I would expect trans people to have a strong interest in this.
(New Point) What I find interesting is no one has shown me a study on the effects pubertal suppression on the suicide rate in trans teens. So one of the biggest arguments I’ve been told in favor of a drastic medical procedure is anecdotal.
@quanta413 :
IQ doesn’t normally increase with age. Problem-solving capacity normally increases with age, but IQ is calculated depending on age – same answers mean a different IQ if you are 10 or 20. Anyway, that Brazilian trans girl is just a data point. The second study you mentioned also has small samples: “(suppressed MFs, n = 8) with untreated MFs (n = 10)”. It’s not enough for a conclusion – it may be just random noise – but I think the hypothesis should be investigated by researchers.
@a reader
Thanks for the correction about IQ with age. I got mixed up.
My goal was to press back against the claim that we had no evidence of harm despite study. When it’s really more like we have little evidence because we haven’t looked much yet, but what little evidence we have suggests harm for MtF at least.
I already mentioned the small sample size in the very first post where I linked
but we’ve got nothing else but that and priors. I’ve been unable to find a larger study. A small sample size of a well validated measurement like IQ is still better evidence than a lot of the rest of what we’ve got which boils down to anecdote and morality.
Like I said above, it wouldn’t be that hard for properly collected evidence to persuade me either way. A single long term longitudinal randomized study would be very strong evidence and is the only sane thing to do for a treatment that is meant to permanently alter development.
I wouldn’t be surprised if MtF or FtM transition protocols had different results or had to be adjusted differently. Actually, I’d be surprised if they didn’t. But these things shouldn’t be figured out by clinicians and patients guessing based upon how they feel. That’s a recipe for failure. They need to at least do large epidemiological type studies. And the research needs to be transparent enough to be trustworthy.
quanta413 , I’m afraid you may be right that puberty blockers may decrease intelligence. It seemed to have happened also when they were used for precocious puberty, IQ decreased with about 7 points, according to 2 studies:
Psychological assessments before and after treatment of early puberty in adopted children
Commentary: Cognitive, Emotional, and Psychosocial Functioning of Girls Treated with Pharmacological Puberty Blockage for Idiopathic Central Precocious Puberty
(I’ve found them linked on a site named “transgendertrend.com” that seems to be anti-child-transition.)
“who are terrified of puberty and threatening (and in some cases, actually inflicting) self-harm – is that not a last resort scenario? How many suicide attempts should we require?”
Is there any other case where giving in is considered the responsible reaction to people who threaten suicide? I mean, I guess there’s Mohamed Bouazizi.
“If you’re willing to come out as trans and put your body through all of that, with all of the stigma and infertility and expense and difficulty finding romantic partners and the like — isn’t that more of a deterrent to making the wrong decision than anything that anyone else could come up with and impose?”
The medical profession could shut it down tomorrow by declaring it contrary to the Hippocratic oath.
Plenty of parents have come to accept their children’s homosexuality only in the recovery room after suicide attempts.
And are there any other medical treatments that we deny people (other than for reasons that better treatments exist)? For example, if a teenager wants to be sterilized, they’ll give you norplant and tell you to wait until you’re 18, which effectively accomplishes the patient’s wishes.
Is that how you think the medical profession works? That there’s some central supreme court of the Hippocratic oath, whose opinions are binding on all doctors everywhere, and which makes proclamations of what specific behaviors and treatments are and are not consistent with the oath?
My answers have largely been ninja’d by Alexander and quanta, but I’d add:
1) I never said I think being trans is a “choice”. Children who desist aren’t making a “choice”, they are experiencing changes (often the physical changes of puberty) that make them not trans. Giving them puberty blockers that lock them into trans if that’s not what they’d naturally be seems immoral. My take is that their are probably biological factors involved in being trans, but puberty is something of a crucible that (for many/most people) “locks-in” your gender and sexual identity. If puberty starts to increase your dysphoria, you’re probably trans. If it lessens it and you start to identify with your natal gender, you’re probably not trans. Given that the former will often require radical medical intervention, and the latter is relatively common, it seems like an approach of “support social transition, but take a watchful waiting approach to physical transition” is the most prudent.
2)
If there’s one thing teens and preteens are particularly bad at, it’s long term thinking and understanding consequences. There’s a reason “you’ll understand when you’re older” is simultaneously the most common, most ignored, and often best advice parents give.
3) I don’t think the comparison with homosexuality is apt. It is much easier for a person with a fluid sexual identity to transition between homosexuality and heterosexuality than it is for a person with fluid gender identity to transition from male to female and back, particularly if body dysmorphia is involved and they feel a need to physically transition. Being gay can come with certain risks, but it doesn’t come with a guaranteed crippling of a body system most people find fairly important in their lives.
I’d argue that anyone who would completely deny that children have agency is unfit to have authority over children, and that recognizing that one’s subordinates have agency of their own is an important step for any leader to take, whether they’re a CEO managing employees, a Army officer managing troops, a professor managing students, or indeed, a parent managing their children, and I might go as far as to say this recognition is the fundamental characteristic that distinguishes a leader from a ruler. Granted, another fundamental difference between a leader and a ruler is that while the ruler makes decrees without explanation, a leader strives to explain their decisions in a manner those affected can comprehend.
Yes, the parent who gives in to a child’s demands to eat nothing but ice cream is doing a very poor job, but I’d argue the parent who simply declares no ice cream and then tries to force feed their child “healthy” foods without regards to the child’s tastes or explanation as to why the ice cream diet is a bad idea isn’t doing much better. The goal should be to find foods that not only adequately meet the child’s nutritional needs and are within the parent’s means to provide to their child, but are also something the child will actually want to eat. Instead of saying “shut up and eat your broccoli”, or “shut up and eat your salad.” the reaction should be more along the lines of “you don’t like the mushy texture of cooked broccoli? here, try a sprig of crunchy, raw broccoli dipped in sour cream.” or “you don’t like lettuce? Here, try some romaine, or maybe some baby spinach.”.
More to the main topic, while I won’t deny there are statistical differences in behavior between men and women, I do think most of our conception of masculine and feminine is cultural, and whether intentionally or not, this seems to be reinforced quite severely on youths with most children’s toys and media being labelled as “for boys” or “for girls”, and while I might be biased, as a man who isn’t very manly by the standards of his homeland, it seems boys get the worst of it(or at least, I’ve seldom, if ever, heard tomboy used in a derogatory fashion, and even a lot of media “for girls” with the girly girl stereotype as the lead protagonist will have at least one tomboy character shown in a positive light, while the closest thing to a widely used short hand for a feminine guy, sissy, is almost exclusively used in a derogatory fashion, and most media “for boys” if they have a more feminine male character, he’s usually the punching bag for a more macho character, and even when more feminine males are portrayed positively, he’s usually gay or trans). Hard to say how common it is, but I’m sure there are plenty of children who think “I act like a girl, therefore I am a girl.” or vice-versa leading to lots of false positives when evaluating children for gender dysphoria. Sure, there would probably still be plenty of shows with mostly girl or mostly boy audiences, and there would probably still be a bias for more men to go into Computer Science and more women to go into the social sciences, but if we could remove ideas like “girls’ toy”, “boys’ show”, “x is for boys”, and “y is for girls” from our cultural vocabulary and promote the idea that anyone can like whatever they want, it might go a long way towards helping children further from the mean be comfortable with who they are rather than try to be something they aren’t to fit in. And if we reach a point where feminine boys and masculine girls are fully accepted without assumptions of being homo or trans or even a point where we’ve discard the masculine and feminine labels altogether, maybe we could achieve a clear picture of how best to help trans individuals.
Does anyone know of any comparison between Scandinavian countries and the US when it comes to gender non-conforming children? Especially Swedish culture is less into gender roles than the US, generally speaking, so it would be interesting what differences this leads when it comes to gender non-conforming and gender dysphoria.
It seems like there are multiple categories, such as:
– People whose outer sexual organs are either ambiguous or the opposite of their internal organs (e.g., certain athletes who dominate in some women sports). These individuals are relatively rare.
– Little boys who are extremely effeminate and little girls who are extreme tomboys. In America until very recently, the boys often grew up to be male homosexuals, the girls somewhat less often grew up to be lesbians. In some Muslim and Buddhist countries, they are encouraged to transition to the opposite sex, and America is now moving in the Iranian direction. A few percent of the population probably falls in this category.
– Adolescent girls who were normal girly girls before puberty but who suddenly undergo Rapid Onset Gender Dysphoria at the same time as many of their friends. This category appears to be increasing rapidly in this decade.
– Extremely nonfeminine men (e.g., military officer, jock, economist, computer scientist, explorer, etc.), often with high IQs and nerdy and/or difficult personalities, who decide at some point that they ought to be women. For example, I was on a classroom team in MBA school with a logically brilliant man with an extraordinarily arrogant personality who was convinced he would make his fortune from outer space, which he then did. He then made a second fortune inventing a medical cure for a disease that had struck one of the children he has fathered. He’s kind of a real life science fiction hero. Now the Washington Post calls this individual “America’s highest paid female CEO.” These individuals are quite rare, but are often high achieving (e.g., America’s most famous Olympic athlete), right of center in politics, and intensely aggressive about shaping the narrative they’ve chosen for themselves and silencing observers who offer alternative conceptions.
My impression is that the first two categories are of average IQ, the third may be above average, and the fourth category may have a sky-high average IQ. I recall Scott citing a study suggesting an average IQ of 128 for individuals of something like this tendency.
I would imagine that Scott’s readership includes a disproportionate number of the fourth category.
There’s a great deal of discussion on the physiological consequences of puberty blockers, mostly loss of bone density, but is there any data on the psychological consequences of blocked/delayed puberty compared to puberty on the normal pace? It seems likely that these are going to be substantial, and I don’t like seeing them left out of the discussion.
The authors do cite de Vries et al on what appears to be a generally positive experience during the period when puberty is suppressed, but that’s about it for data and it’s hardly the end of the story. Particularly if “should transgender children transition” is taken to mean that we should greatly expand the use of puberty blockers, that’s going to have an awful lot of people going through delayed puberty, and from the desistence numbers in part 1, at least half of them are going to be people who either will revert to their natal sex or would have done so if not for the puberty blockers. And even the ones who will inevitably fully transition, will likely suffer from the delay.
It seems to me that if we are very highly confident that some identifiable subset of transgender children will inevitably transition, we should be going straight to hormonal therapy for transition at the time of natural puberty, and if we are not so confident then we risk causing great harm by retarding the puberty of people who mostly would have been happier letting nature take its course. Puberty blockers seem like a minimum-benefit, maximum-cost solution.
That’s a strong hunch, subject to revision if e.g. the data says delayed puberty causes little harm. Do we have that data?
I have not looked into this myself beyond reading a couple blog posts, but I’ve read that one puberty blocker has been linked to cognitive problems and (more tentatively) to problems noticing cognitive problems. If true, that seems very significant.
I made a post in another subthread with a little evidence about the effect of puberty blockers on cognitive function.
I’m trying to figure out how to link it, because it’s rather long.Figured it out.+1 to the question, “Why not immediate hormonal transition instead of puberty blockers?”
Also, an analysis of non-trans use of puberty blockers might shed some light on how we assess their risks when they aren’t a political football.
Two points that I feel should be mentioned:
(1) The criteria for gender dysphoria in children have changed in the DSM-V and (IMO) do a better job of distinguishing gender dysphoric children from gender-non-conforming children who happily identify with their birth sex. Many trans activists, including myself, suspect that desistance rates will be lower with more precise criteria that don’t classify a boy who likes wearing pink dresses, playing Barbies, and having female friends as transgender despite his firm insistence that he is in fact a boy. That said, of course this is speculative.
(2) One of the major benefits of puberty blockers is passability. A trans person who never goes through the puberty of their birth sex is far more likely to pass as a member of their identified sex, even to people who know lots of other trans people. In my opinion, increased passability is by far the greatest quality-of-life increase from blockers. Looking like a member of your identified gender reduces physical dysphoria, passing reduces the amount of misgendering you get and thus reduces social dysphoria, and passing protects you from discrimination you would otherwise face as a transgender person.
Dysphoria, although recommended as a qualifier for medical transition in youth by the Endocrine Society Guidelines, is not in fact required by some clinics in the US.
Here’s Dr. Ilana Sherer at the recent Gender Spectrum conference explaining how she has Diane Ehrensaft a child psychologist and expert in the field “rubber stamp” medical interventions for non-dysphoric youth
“Non-binary” youth are also able to access medical interventions in the US, even in the absence of dysphoria.
The audio in the above link is Dr. Johanna Olson-Kennedy who heads the largest pediatric gender clinic in the US at CHLA. She’s contradicting your claim that most trans youth desire passability.
I don’t understand what your comment has to do with my point. Research, in general, uses the DSM-V definitions of terms, and research is the subject we’re talking about.
Your first example is troubling, but is also thirty seconds completely out of context in which the speaker explicitly says that it is obviously not a rubber stamp.
Your second link does not include any evidence that nondysphoric children are given medical interventions, other than a quote which is glossed as “[for gender dysphoria].” I listened to the linked video and it appears to start midway through a talk, so that I can’t tell what criterion the person is discussing. Some potential criteria would be very reasonable: for example, there is no reason to deny medical treatment to a transmasculine person who likes wearing dresses, because it is wrong to deny a person medical treatment for no other reason than that they are gender-non-conforming. The rest of the article consists of the shocking revelation that a doctor is trying to customize her treatment to the needs of her parents, as well as some fairly astonishing anti-autistic ableism. “Young people with autism are not exactly known for their self-sacrificing nature or their ability to reflect upon the feelings of others,” really?
@Ozy:
Indeed, in DSM-IV, [very] gender nonconforming children could be diagnosed with GID even if they didn’t say they feel like the other sex – but not in the older DSM-III, where wanting to be or saying he/she is the other sex was an obligatory criteria for diagnosis:
source: http://www.cpath.ca/wp-content/uploads/2009/08/ZUCKERDSM.pdf
And look at the table: the studies that only used DSM-III (or DSM-III-R) for childhood diagnosis have quite large numbers of desisters: 30% in natal girls, 58% and 75% in natal boys (even larger than the last study, Steensma et al.(2013), that used both DSM-III and DSM-IV).
What they don’t have (and the stuidies using DSM-IV have) are subthreshold children that later persist – so it seems DSM-III may have been better at diagnosis than DSM-IV.
Thank you very much for the correction!
The high rate of desistance among people assigned male at birth does make me wonder if there’s a social component, particularly since the rate of gender dysphoria diagnoses has gone up in people assigned female at birth. Of course, this could go either way– perhaps future research will find 60% of people assigned female at birth desist!
(A personal note: I myself am a person who became dysphoric at puberty and was not dysphoric in childhood, so this subject is very interesting to me. IMO the evidence clearly suggests that hormonal shifts such as puberty and perhaps pregnancy/breastfeeding/menopause affect how severe a person’s experience of dysphoria is.)
This question becomes simpler if we define “children” and “gender transition.” If we’re asking whether a six-year old should receive sex reassignment surgery, the answer is no. If we’re asking whether a teenager should be able to dress in a gender non-conforming manner, the answer is yes.
For this reason, both the World Professional Association for Transgender Health and the Endocrine Society have issued concordant clinical practice guidelines that make age- and procedure-specific recommendations. These guidelines can be summarized as follows:
1. Dysphoric kids shouldn’t receive any drugs or surgery before the onset of puberty.
2. During early puberty, kids can start receiving puberty blockers.
3. At age 16, kids can start receiving cross sex hormone therapy.
4. Irreversible surgery should not be performed until adulthood.
These evidence-based guidelines represent the most aggressive treatment commonly delivered to minors in the United States. The positive mental health impacts of puberty blockers for early adolescents followed by cross sex hormone therapy was demonstrated in de Vries 2014, which found zero desistence and well-being for treated children to be comparable to cisgender controls. This is an amazing finding for a population that, when treated later in life, has a ~20% suicide risk (see Dhejne 2011). It is the consensus view of practitioners that these benefits outweigh potential (currently speculative) bone health risks.
You are sadly misinformed if you think that in the US, clinics are following either of these guidelines.
Kids as young as 12-years-old are being given cross-sex hormones and natal females as young as 13-year-old are being given “chest surgery” (mastectomies). Both studies were financially supported by the NIH.
A study by WPATH’s Dan Karasic and Christine Milrod titled “Age Is Just a Number: WPATH-Affiliated Surgeons’ Experiences and Attitudes Toward Vaginoplasty in Transgender Females Under 18 Years of Age in the United States” found that of the 20 (anonymous) surgeons surveyed, 11 admitted to operating on boys under the age of 18.
From the NYT: “Several doctors said they had performed surgery on minors. Kat’s surgeon, Dr. Christine McGinn, estimated that she had done more than 30 operations on children under 18, about half of them vaginoplasties for biological boys becoming girls, and the other half double mastectomies for girls becoming boys.”
In addition, dysphoria is not a requirement for medical interventions as suggested by the Endocrine Society Guidelines.
Thanks for the Olson-Kennedy studies. I hadn’t seen either of them.
You’re correct these guidelines are not always followed in the U.S. and I didn’t mean to imply that they were. Particularly, in a research context, it makes sense to stretch these cut-offs. So I don’t find the Olson-Kennedy studies necessarily concerning, though I am surprised to see that they performed chest surgeries on such young girls. Fortunately, they seem to have found positive results.
I’m less comfortable with individual physicians radically deviating from clinical guidelines without good reason. However, I imagine the majority of such deviations are for people very near the age cutoff with special circumstances. For context, I believe McGinn has performed ~500 surgeries, so having 30 or so “special circumstances” is not that crazy.
Still, I definitely concede that there are instances of practitioners being too aggressive in treating minors. That’s a problem when it happens, but I think the answer is to refer back to these reasonable guidelines rather than to be upset that “children are transitioning.”
mo, why did you abandon our collaboration? I’m not upset – as you see, I found another partner-adversary and we finished this time – I’m just curious what went wrong first time (may be useful to know for the future).
I’m sorry 🙁
It was 100% my fault– I sent you an email.
A few issues are not clearly addressed here:
1. Data from all pediatric clinics shows that 90-100% of youth who are blocked in puberty continue to sex hormones. Suppressing natal puberty appears to lead to persistence.
2. Puberty blockade that starts in early Tanner stages and is followed by sex hormones results in sterility 100% of the time. Natal puberty is required for fertility. In addition, questions have been raised about how denying natal puberty impacts later sexual function. (GnRH agonists have also been used successfully to suppress sexual desire in repeat sexual offenders)
3. The above link includes audio of Johanna Kennedy-Olson the director of the largest pediatric gender clinic in the US talking at a recent Gender Spectrum conference. In the audio, she confirms that GnRH agonists often lead to increased emotional lability, a side effect for which the FDA required additional warnings in May 2017.
GIDS/Tavistock sees 42% of youth qualify for medical interventions and of those youth who block puberty, 95% continue to sex hormones
100% of Dutch youth: de Vries, “Puberty Suppression in Adolescents With Gender Identity Disorder: A Prospective Follow-Up Study”
“[Norman] Spack has, he says, put “about 200 children” on to hormone blockers at the onset of puberty. Of these, 100% have gone on to take cross-sex hormones because “no one changes their mind”.”
>Suppressing natal puberty appears to lead to persistence.
Or parents and doctors are very good at determining who is truly trans and not giving blockers to those who will later go on to desist, as the reading speculates.
One would hope. The problem with the affirmative model being used in the US vs a ‘watchful waiting’ approach in the UK, is US clinics report that 100% of youth seen for services qualify for medical interventions. In the UK, only 42% of youth seen receive medical interventions.
Doesn’t that seem extraordinarily unlikely when no one can tell beforehand who will persist and who will not? There don’t appear to be any objective criteria that could achieve such accuracy. Is this the one area where doctors are super geniuses and magically by physical proximity can determine something that no one can on paper?
Very good stuff, only improvement I think would be to include more on the physical outcomes (positive and negative) of puberty blockers. Not just mental health and osteoporosis – are trans persons who have additional gender surgeries after puberty blockers substantially more or less happy with their physical outcome, compared to those who did not begin physical transition until after puberty? What happens if a child desists after or during puberty blockers? What is the outcome?
Puberty blocking seems like the really controversial issue here, and the most important one to get right. Social transition, or at a minimum support for gender nonconformity, ought to be less controversial and is certainly more easily reversible.
I know it’s morally tricky to talk about a “preferred” outcome, but to me it seems that children should be given an opportunity to desist, if they are going to. Gender reassignment is far from perfect, and at best results, after a great deal of physical and mental stress, in a person who can pass socially and not have body dysmorphia, but is infertile and may have other serious sexual dysfunction. If a child might be mentally happy in their “natural” body, that seems like it should be a medically preferred option, with pre-puberty physical transition something of a last resort.
This article is interesting since I haven’t actually done a lot of research into the subject, but it’s affected my life a lot. I’m transgender and started socially transitioning in 7th grade, though I only started feeling gender dysphoria at the onset of puberty. More relevant to this subject though is my 6-year-old cousin, who has declared himself a guy and is insisting on fully transitioning. Following the traditional social metrics of “guys versus girls” activities, he’s always been more interested in guy things, but nobody in our extended family puts much stock into these perceived gender roles and so we hadn’t been paying attention until his full-on declaration.
It seems to me that if a child is dedicated enough to insist on a social transition, it’s kind of unavoidable – my cousin’s friends would already be calling him a guy even if my aunt hadn’t intervened, etc. It’s more the question of puberty blockers and other things. To me as a trans person, I can’t understand it because I only found reason to force a transition, both socially and physically, after and during puberty – before then I didn’t really understand the concept of gender.
I guess I’m not really saying anything strong here except I don’t understand how trans groups can through themselves wholeheartedly into supporting transitioning children (especially through physical means) when sometimes dysphoria isn’t even that relevant to a child, and gender roles can be generally obsolete anyways. Then again, I didn’t have Gender Dysphoria as a child, so who knows.
As a disclaimer, I’m not a trans guy – I consider myself nonbinary, they/them pronouns, the whole shebang. If I hadn’t known nonbinary was an option from the internet though, I think I would’ve tried to transition to being a guy as a child and then “desisted” by the time I reached the age I am now, since my dysphoria isn’t that strong now and has mostly been mitigated through therapy.
These stories concern me. I wonder if kids who grow up in “progressive” families may have a somewhat confused idea of what gender is, and think that it’s something they can just pick and choose, i.e. they think “I’m a guy” is the same of “I’ll be an astronaut”.
The problem is that if a kid says “I’ll be an astronaut” the parents will just say “Sure, darling”, while if a girl says “I’m a guy”, the progressive parents will take her to one of these pediatric gender clinics where they’ll screw up her endocrine and reproductive systems for good before she’ll even understands what sexuality and reproduction and gender identity are about.
When I was 9 or so I was very insistent that I would never like girls. Imagine if there had been a bunch of asexual activists around back then pushing for puberty blockers for kids like me. I would have been cut off from so much of life.
Same here.
I also used to dislike the idea of growing into an adult man. Not that I wanted to be a woman, I just wanted to remain a sort of child-like asexual person, even though I didn’t have the language to express that at the time. Adult men looked scary and brutish to me, and once I knew about sex, the idea felt repugnant. Bad role models, I suppose. When the first hair started to appear on my face it was awkward, I’m not sure if you could call it dysphoria, but sort of.
Then puberty really kicked in, girls started to look beautiful, the idea of sex started to feel interesting, and being masculine started to feel good.
I dread what could have happened to me if I ended up in the hands of these gender activists, and I wonder how many boys and girls, “confused” like I was, become irreversibly damaged due to these gender reassignment practices.
The footnotes beyond the first don’t appear to be referenced in the text?
The footnotes 2-6 are referenced in the table.
Do puberty blockers disrupt fertility?
Completion of natal puberty is required for fertility. When followed by sex hormones, use of blockers result in sterility 100% of the time. They may also greatly limit sexual function.
Whoa, that seems like a pretty massive negative side effect of puberty blockers ! How come this wasn’t mentioned in the article ?
Indeed. Sterility is the main negative effect of medical transition, it’s strange that the article never mentions it.
Being sterile and/or asexual does not make you a “broken” or less valuable human being; it doesn’t necessarily have to make you a less happy human being either. I know that this was not mentioned in researchermom’s post, but bugmaster’s reply sounds the way I’d imagine most of society would react to this fact. I think this is a case of typical mind fallacy: something like 99% of humans would be significantly unhappier if you took away their libido; that does not mean it shouldn’t be an option for the other 1%.
In fact, if you have a transitioner who feels disgust and shame at the body parts they were born with, they’re less likely to have a “normal” sex life in the first place.
I agree these facts should be known and discussed with anyone considering hormones (although from what I can tell, the trans community is quite aware of this already), but SSRIs are also known to have side-effects in this area (in exchange for a small chance of improving your depression in the meantime) and we still prescribe them.
Personally, I think taking puberty blockers and getting these “side effects” would have been one of the best things that could have happened to me and it might have lessened a lot of the mental health issues I’ve been struggling with since.
To be fair, this is the first time I’ve heard anyone warn that testosterone might result in sexual dysfunction…
Thank you! Reading a comment like this 10-18 years ago would have been super helpful.
Does anyone have information about what proportion of people care a lot about being fertile?
Obviously, some people care tremendously about the ability to have biological children. Some people would rather be sterile, and (if female) have a lot of trouble getting sterilized.
I’ve seen enormous amounts of self-reporting from cis-hetero women who, on learning that they are infertile, feel broken in a fundamental way. I think this is real and substantial, and it will probably affect at least some trans women. And as always, non-anecdotal data very much welcome.
But if we’re going to use words like “broken”, it should be in the same sense that we would refer to e.g. deaf people as “broken” – there’s a normal biological function correlated with positive life outcomes that isn’t functioning and we don’t know how to repair, but this is in no way a moral judgment or an assignment of lesser worth as a human being.
And of course we don’t use “broken” for deaf people, but the substitutes keep riding the euphemism treadmill to the same connotation if we aren’t careful. So maybe we shouldn’t use “broken” for trans people, but definitely we should watch out for negative moral connotations with whatever words we use to talk about unfortunate biological circumstances.
Also, can someone get to work on uterine replicators?
Isn’t there a significant chance that “feeling broken” about infertility is socially driven? After all, many sexual minorities went through a phase of “feeling broken” for not being heterosexual when they first discovered their desires.
Never mind the ~4 billion years of evolution driven by the pressure to maximize the number of copies of your genes in existence, it’s all a social construct. /s
@AG – Homosexual here; I consider infertility to be the worst form of brokenness that a person can have (not necessarily the most painful) aside from causing infertility in others. I haven’t contemplated suicide particularly since I still have relatives whose lives would be ruined if i did, and I’m not clinically depressed about this fact, but as a homosexual it’s genuinely hard to justify my own existence as such.
To be clear it, has nothing to do with religion and I’ve become less gay-firendly the more secular and gay-friendly the world has become.
Not the most physically or mentally painful thing in the world, but an organism that is incapable of reproducing has ‘failed’ the game of life in a way that, say, ‘not earing a high enough salary’ or ‘not having a big enough house’ simply cannot compare.
It’s simply not sustainable to establish as a principle that everything that a social organism might consider a “virtue” [i use that term loosely] [Fertility, Wit, leadership ability, strength, care-giving] needs to be deconstructed so that people who lack that virtue feel more like they belong. If you took this to its logical conclusion you wouldn’t have a society that would be worth belonging to to begin with. The only reasonable approach to this if one virtue is lacking, try to emphasize the others. If you can’t have a biological family of your own, try to support the biological family of your relatives or people you think are upstanding.
> When followed by sex hormones, use of blockers result in sterility 100% of the time.
Isn’t this a little like saying ‘When followed by being shot in the head, eating cereal is 100% fatal’?
I thought the reading said that puberty continues normally after going off the blockers. Do the blockers themselves cause permanent infertility, or not?
If GnRH agonists are used during early puberty and then suspended with natal puberty completing, female fertility is minimally compromised. Much higher rates of POCS are common, however, which can impact fertility.
However, when 90-100% of all youth who are put on blockers for gender identity continue on to sex hormones, that means 90-100% of youth who are blocked will end up infertile. You cannot go back and restart natal puberty after initiation of cross-sex hormones.
Puberty blockers themselves don’t cause definitive sterility – the Dutch researchers say that if they are stopped, natural puberty resumes. They were used to delay precocious puberty before being used for transition.
Of course, if they are followed by cross-sex hormones that cause opposite sex puberty, the combined effect will include sterility – I think this is quite obvious, but maybe we should have said it explicitly in the article.
About lack of orgasm as an alleged side effect it’s the first time I hear.
This is really good. Thank you both for making it happen.
My understanding is that the current WPATH guidelines https://www.wpath.org/publications/soc recommend that socially gender affirming what a child feels is the right way to go (among other things, bullying a child into behaving in a socially normative fashion when all they’re doing is figuring out their identity- which could go either way- is clearly harmful), and that puberty blockers should only be prescribed carefully in the context of rigorous and longitudinal assessment in a paediatric gender clinic with a multidisciplinary team of paediatricians, paediatric endocrinologists, psychologists, child psychiatrist, etc. Certainly in Australia and New Zealand that is what is required for an adolescent to be prescribed puberty blockers, and I think that’s wise. Among other things, there’s nothing harmful about psychotherapy- it is beneficial. And of course, presence of intersex conditions can also be identified.
To share my own experience:
As a trans guy, I can say that my parents letting me play with whatever I wanted to and not making me dress in girly clothes was a protective factor. Going to a homophobic single sex girl’s school was the opposite of a protective factor. I transitioned later in life, and as an adult, time and extensive counselling was helpful for me to sort out what I wanted to do. While I wasn’t that distressed by puberty many other people I know were. I do have some quite distressing memories of being bullied as a young child by other children for insisting I was a boy or wanting to play with boys.
Had I grown up in this day and age, and with accepting parents I would imagine that I would have presented as a boy and being the indecisive person I am, would have taken a while to make any decision, would have gone to counselling/gender clinic, and I’m not sure that I would have made a decision around medical intervention early. But I might have, because my gender identity was very strong from a young age.
At the same time, there is evidence that earlier transition tends to result in better healthcare/mental health outcomes, partially because of not going through puberty.
I’m friends with a number of people who may have identified as the opposite gender to how they identified as adults (and are now cis-identified)- I don’t think they would have been harmed by socially gender non-conforming as children? Some parents have been known to be physically and emotionally abusive in order to ‘correct’ gender expression. The length of time they could have potentially been exposed to puberty blockers would have on the grand scheme of things *if at all* (big ‘if’) fairly short.
As a doctor, I can say that my profession *as a whole* is very transphobic and even homophobic- possibly because I work in Australia. My specialists have all been amazing but they are sub-specialised in gender work, and have a great deal of experience- as well as being very savvy about the complexities around if someone is lying to them or has been coached to hide things. However the broader context of medicine and society really does need to be taken into account when considering the treatment of children in the system. Ultimately they are best served by subspeciality multidisciplinary clinics, and we all need to remember that being a trans person- adult or child- means you are prone to exposure to hateful and discriminatory behaviour at times. Some of this is reflected in the literature, as some researchers are transphobic. It’s not the case that even transitioning socially is an easy neutral binary decision- by which I mean that a lot of factors can cause people to ‘desist’ (what a word!), and at least in adults a lot of so-called ‘detransitioning’ is due to being ostracised from society, rather than a lack of gender dysphoria. That said, gender identity in children does fluctuate and it takes time for them to sort out who they are, thus the advocation of a careful approach by WPATH.
Long term, it may be that those who are prescribed puberty blockers are concurrently prescribed osteoporosis medications to prevent loss of/inadequate bone mineralisation- certainly it’s a risk that can potentially be mitigated medically.
There’s been a lot of scare stories in the media where they say 6 year old boys are being given oestrogen and I have no idea where this rubbish comes from because that’s clearly untrue.
Once again, hugely impressive. I’m not going to vote because I haven’t devoted adequate time to reviewing the details of the submissions to have an adequately informed view but my bottom-line response is the grade school teacher’s “you’re all winners in my book.” Minor reactions to this one:
1. It’s funny to me that the entry would address the “should” question posed without even alluding to questions of morality, which would presumably be significant for many on the “con” side of the debate. I get that this is just so far out of the realm of consideration for many here that many in this community would consider it perverse even to discuss, and I also get that it would be difficult to get one’s hands around this side of the issue, but maybe at least a placeholder for the core of the majority view would have been warranted.
2. On the empirical question, one part of this that I had a hard time teasing out was imagine a scenario where the adverse mental health issues associated with dysphoria are not caused by the dysphoria, but rather dysphoria is one among many symptoms of a larger condition that produces an array of symptoms (e.g., depression, anxiety, suicidality, gender issues, etc.). Just showing that people with these gender issues also tend to be depressed, etc., obviously doesn’t show that the depression stems from the gender issues any more than the other way around. But without eliminating that possibility it seems even harder to assess the effects of “transitioning,” etc. What if “transitoning” disproportionately occurs in families that care about their children a lot (which is why they are willing to engage in the exercise), and then any positive associations stem from having disproportionately caring families rather than from the intervention? Similarly, is “transitioning” more common in communities that are more accepting of nontraditional gender roles, and any correlation with positive outcomes come from that rather than the intervention? Some of these are touched on in various ways but it was hard for me to tease these possibilities apart. (Talking about Samoa, e.g., doesn’t make it obvious how this sort of thing applies to intra-geographical differences within, say, the United States.)
I was actually wondering the same thing as point 2. The other question I’ve always had was if there were any studies done on dysphoric individuals who were given hormones corresponding with their biological gender, and what the results were.
The answer is yes: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5010234/
Unfortunately there is a lack of numbers in many studies resulting in underpowering for positive outcomes, but it looks like we will have an explosion in medical research in the not too far future.
This looks like a study about being given hormones corresponding to their preferred gender; by saying “biological gender” in their original comment I would have understood them to mean scenarios more like “giving estrogen to a trans man”—perhaps under a conversion-therapy conjecture that the dysphoria comes from being insufficiently feminine and that it might induce them to “desist”?
1. Given that most of us are utilitarians (I assume?) from our perspective the entire article was about morality. I assume you more mean ‘surprising that they didn’t consider the religious/virtue ethics position’, but I’d say that those are fully subjective opinions that are not susceptible to change by empirical analysis, and therefore there’s not much point in researching them in this format.
2. If there were a meta-disorder that caused a wide range of mental disorders in the same person, including gender dysphoria as well as anxiety and depression, then you would expect transitioning to do nothing to treat this underlying meta-disorder. However, this reading seems to say that both social transitioning and puberty blockers both massively decrease all the other mental disorders including depression and anxiety, which indicates that the dysphoria is upstream of those other problems.
Let’s say a child would persist if enabled, and wants to transition; but it is very statistically likely that they would desist if you nudged them in that direction. What should a preference utilitarian do, given that their present desires clearly point toward transition, but they might have more psychological problems down the road if they persist? How do you take the preferences of children into account, anyway? We usually think of them as not too important, such that parents can often overrule them in order to protect their interests; but what counts as an “interest” in cases like these?
Utilitarianism still demands you come up with a utility function. There are big unanswered philosophical questions here, even if you’re a committed utilitarian, and it would have been cool to see those grappled with a bit.
Similarly I was curious if there’s any literature available on efforts that try to address co-existing psychiatric disorders before addressing gender dysphoria. For example, I would imagine that in addition to allowing for social transitioning, that providing CBT for anxiety issues or anti-depressants would relieve other symptoms and possibly increase the desistance rate.
On another note, I’m surprised no information was included on binding. While binding isn’t surgical, it definitely is an intervention that can come with socialization if puberty blockers/hormone therapy hasn’t been used, and there are definite side effects to such an intervention.
In Dr. Lisa Littman’s recent study of parental reports of teens with rapid onset gender dysphoria, she found that “For parents who knew the content of their child’s evaluation, 71.6% reported that the clinician did not explore issues of mental health, previous trauma, or any alternative causes of gender dysphoria before proceeding and 70.0% report that the clinician did not request any medical records before proceeding.”
CBT has been used successfully in the past to manage body dysmorphia but it is not reportedly used for youth with gender dysphoria under current affirmative models.
I agree with you about binding
The APA gets at the heart of the issue: “gender nonconformity is not in itself a mental disorder. The critical element of gender dysphoria is the presence of clinically significant distress associated with the condition.”
Gender is a set of social expectations and role(s). The classic “gender is a social construct.” Most of us (~98%) find that whatever was put on our birth certificate matches the social expectations we would prefer to adopt. And if there are some things we don’t like, we just don’t adopt those, or push for social change. We keep the label. Some find conforming and labeling really unacceptable to them and reject the role. Some even to the point of distress. There is a spectrum of gender conformity, and the amount of distress generally increases along the spectrum, as you might expect when you’re out of sync with what everyone else seems to believe. Thus the prescription for social acceptance and understanding makes a lot of sense- it affirms one’s value beyond the roles one does not want to accept, reducing anxiety.
But this spectrum is fluid! Gender identity/conformity is fluid. So, if one might identify with some of the positive associations with the gender female for a while but eventually realize that simply being a “girlish boy” and identifying as male is fine, what kind of interventions should that person be taking? Perhaps greater gender education or available resources (at guidance offices) would benefit borderline students. They might learn that anatomical transitioning is expensive and complicated and should only be done when they are absolutely certain. Then, the most vocal transgender children should be taken more seriously by their parents. On the other hand, it might give pause to children who realize that there is a spectrum and you don’t have to identify with the opposite gender just because you don’t feel completely at home with your current label, and that it’s okay to incompletely adopt your gender roles/associations (a la localdeity), which should reduce distress by itself. As gender associations become less rigid, too, implied social acceptability will improve and distress should drop. Another note: parents have control of the household sub-culture.
There’s plenty to be done before transitioning your child after the first time they express some gender identity confusion. And it doesn’t have to “treat” them like they have something wrong with them. Lots of room to be affirmative.
Yeah, it seems to me that teaching children about the fluid spectrum nature of gender would have a huge positive impact.
Or not talk about it in terms of gender in the first place. So your daughter likes physics. “Ah, I see, you’re getting in touch with your male side. That’s perfectly all right, society is accepting of all kinds these days.” Good lord, please no. How about: “Physics is a great subject; can I get you some books on it?” If your son wears a dress around the house, my instinct would be to not express any opinion about it. (I suspect it’s good to not talk about appearance in general, except maybe when the kid is an adult and wants to make a serious effort to attract one of the sexes.)
There are some behaviors that might get the kid in sufficient trouble that the parent should do something about it. When I was to start swimming lessons and needed a swimsuit, I wanted a one-piece swimsuit that went up to my shoulders like my sister had; my mom said the adults wouldn’t allow it and she wouldn’t get one for me. I think that was the right call. (A kid going into an opposite-sex bathroom is probably another example of something for which society would impose significant consequences on the kid, and therefore the parent should warn against doing it.) She also didn’t make a fuss about my having long hair, and I think that was also the right call. Protect the kid from getting in trouble with the adults, but otherwise don’t make them think about gender roles any more than is absolutely necessary.
“This may be a sign that your child is Scottish. Do not under any circumstances allow your child to wield any kind of greatsword during this time.”
I must object to your scotshaming, sir.
If your child shows signs of being scottish, they should be encouraged to transition to the claymore as early as possible. They’ll need a training sized one, of course, but it takes a lifetime of practice to properly swing a sword that’s longer than you are tall.
I’m sure that an entire culture which accepted more fluid and weak gender roles would be beneficial to gender nonconforming children, and might well cut down on the demand for transitioning.
However, I’m very skeptical of teaching dysphoric kids who are growing up in a gender restrictive culture about gender fluidity as an alternative to transitioning. They will still have to interact with the restrictive culture eventually, and I doubt that being told by their parents that this is all silly will do much to lessen the trauma and anxiety from this interaction.
What are the effects of puberty blockers on mental health for *non*-trans children? Is anything known about that? One would expect them to also be positive, since puberty is usually psychologically uncomfortable in itself. Although showing outward signs of not hitting puberty on time is probably socially deleterious.
Not my experience. Puberty was great! I was taller, stronger, could run faster, learned how to masturbate… Growing hair on my face was a minor inconvenience, and the sudden overwhelming sexual urges were a mixed bag, but there was a lot of unambiguously good stuff.
Seconding that anecdata. I barely noticed puberty; it was like “huh, I have hairy balls now, neato, time to grow a wizard beard like I always wanted.” The early growth spurts were way worse for me; those actually hurt.
However, I had bigger things to worry about at the time. Maybe for someone who lives a normal near-zero-adversity childhood, having your hormones kick in really is a traumatic experience.
In May 2017, the FDA required additional warnings for Lupron that include:
“Psychiatric Events
Psychiatric events have been reported in patients taking GnRH agonists, including LUPRON
DEPOT-PED. Postmarking reports with this class of drugs include symptoms of emotional
lability, such as crying, irritability, impatience, anger and aggression. Monitor for development or worsening of psychiatric symptoms during treatment with LUPRON DEPOT-PED [see Adverse Reactions (6.3)].”
and:
“Psychiatric Disorders: Emotional lability, such as crying, irritability, impatience, anger, and aggression has been observed with GnRH agonists, including LUPRON DEPOT-PED [see Warnings and Precautions (5.2)]; Depression, including rare reports of suicidal ideation and attempt, has been reported for GnRH agonists, including LUPRON DEPOT-PED, in children treated for central precocious puberty
I’d be interested in knowing what the effects of loss of bone density are. I think it really changes the decision-making calculus if the outcome is, like, “slightly increased risk of osteoperosis when you’re seventy” or if it’s, like, “chronic pain.”
I also would be interested in this. My instinct is that social transition is relatively minor step, so children who expressed a reasonably fixed desire to socially transition should probably be allowed to do so. It may be that the process itself helps to crystallise their feelings, and if they desist, they can transition back relatively easily. On the other hand, my instinct is that preventing puberty is a fairly drastic intervention that a pre-pubescent child can’t understand, so I would be inclined to caution. But the only negative effect identified here seems relatively minor: a choice between low bone density and suicidal depression seems easy. So I’m inclined to update towards puberty-blockers being less risky than I had supposed.
Unfortunately, this otherwise mostly on-point post failed to note concern for other major long-term side effects from puberty blockers used to treat girls with precocious puberty as exposed recently by Kaiser Health
There is also an n-1 published study that found a significant decrease in IQ: “Brain Maturation, Cognition and Voice Pattern in a Gender Dysphoria Case under Pubertal Suppression”
In addition, from what’s known, 90-100% of youth placed on blockers for dysphoria in the UK, Holland, and the US, continue to sex hormones. As a result, sterility and negative impact on future adult sexual function should be considered.
Regarding the word choice of “desist”– I’m just curious why they don’t use the term “remission” (or “resolve”) instead? Because here we’re concerned primarily with the emotional distress that the people are under, right? We might say that a symptom or a disease “persists” or “is persistent”, but we don’t say that it “desists”, we say it “resolves”, “is cured”, or “goes into remission” (if we think it might return at some future point). So if a person’s mental distress about his/her bodily gender dissipates after puberty, then the condition has resolved, or perhaps gone into remission, rather than the person is “desisting” from mental distress.
They are mostly desisting from overt external cross-gender behaviours, or from expressed cross-gender identification, probably not desisting from cross-gender experiences and desires.
It does not ever really go away, you just get used to never getting what you really want and have to learn to accept it.
Hate to contradict you, but according to the sources and the article itself, that’s not what many desisters report (though I assume that some may feel as you say).
Several are quoted in this post self-reporting a cessation of desire to be the other sex, and/or a cessation of feeling that they are the other sex.
@emmajoey: according to Steensma et al. (2011), a Dutch qualitative follow-up in which persisters desisters tell their experiences, in those childhood (puberty) desisters it seems to be really the case of ceasing to feel like the other gender.
There are for example 2 girls who lived almost like boys in elementary and middle school (didn’t change name and pronouns, but looked like boys and were treated like boys) who during puberty wanted to revert to their natal sex:
Also during puberty, the boys discovered “a good side of being a boy”:
Lucky for boys number 3 and number 10. Some of us discovered around puberty all the things that we really wanted to do with our body as a girl, but couldn’t because we didn’t have the necessary parts, and the things we thought we were supposed to be thinking about as a boy just didn’t seem to connect with any actual emotions.
But by that time you are pretty much stuck with it, and 20+ years later it still doesn’t work properly.
Sounds like you did not desist?
As always, comparing health outcomes in post treatment populations vs health outcomes in the general population is misleading and incorrect. Consider: individuals who have undergone chemo therapy have decreased health outcomes compared to the general public. Does this mean that chemo therapy is a bad treatment for cancer? No, no it does not. In order to have a valid comparison, one must compare post-treatment and non-treatment populations, not post-treatment vs healthy populations. Which, in the case of transgender individuals means comparing GID diagnosed individuals who socially transition/who receive puberty blockers/-insert proposed intervention here- vs GID diagnosed individuals who do not socially transition/who undergo normal puberty/-insert nonintervention here-.
It may well be that puberty blockers lead to a positive mental health impact and negative physical health impact. But none of the studies cited here appear to have the ability to demonstrate such, let alone which impact is more weighty.
To be fair, there’s no reason to believe that being transgender would cause one to have less bone density.
On top of that, some puberty blockers had bone density decreases as a known side effect before people were really interested in studying transitioning. Leuprolide acetate for example.
It would be amazing if blocking normal physical development didn’t have a bunch of negative side effects.
Sun exposure is correlated with bone density, isn’t it? Is there any reason to believe that Gender Dysphoria might correlate with reduced sun exposure? Ex, minimizing visibility of antidesired secondary sex traits, or general withdrawal due to negative responses from community/peers?
Really interesting read, but I’m not sure it answers the question the title poses. Whilst we now have a great overview of the relevant facts, whether or not children should transition seems to be a potentially tricky ethical dilemma. I would be interested in hearing from the authors to know if they originally attempted to come to a conclusion on this, but couldn’t agree, or whether they only ever set out to clarify the facts.
My gut feeling on this issue has always been that we should happily encourage children to socially transition and experiment with gender, but the use of puberty blockers with permanent effects concerns me, and I’m not confident that doctors and parents are able to distinguish between those who will clearly benefit and those who might end up ‘desisting’. But then I haven’t thought about this in depth, nor am I aware of what damage transitioning and regretting it does, especially compared to the obvious damage that not transitioning early can do.
I mean, it seems like the reading precisely addresses these concerns. My reading was that very very few teens who go on puberty blockers later end up desisting, indicating that doctors and parents are very good at determining who should use them. And the only roundly confirmed health consequence appears to be bone density stuff.
This doesn’t follow. Desistence may be well caused by natural puberty. And since desistence is a preferable outcome than transition, puberty blockers may be harmful.
And sterility. And anything that is a health consequence of transition, if that transition could have been prevented by desistence.
hahaha! my reading was that this indicates that puberty blockers prevent many people from desisting who otherwise would
The real problem is letting kids have a say. Parents routinely make decisions for their kids – where to go to school, which parent to stay with after a divorce, up to and including whether to undertake life-threatening surgery. Ya know why? Because children lack agency. Kids have a lot of stupid ideas that parents shouldn’t allow, for their own good. Imagine 7 year old Aban:
“I want to eat ice cream for dinner every night!”
“No, Aban, that’s a bad idea. We’re making this decision for you, for your own good.”
“I want to get a gun!”
“No, Aban, that’s a bad idea. We’re making this decision for you, for your own good.”
“I want to move to rural Alabama!”
“No, Aban, that’s a bad idea. We’re making this decision for you, for your own good.”
“I want to be a girl!”
“OK Aban, let’s call the doctor and get you on drugs that will seriously alter your body hormones and possibly permanently affect your ability to have children.”
In making those decisions, parents routinely get information from the child. “My arm hurts really bad” “What happened?” “I fell several feet and landed at a bad angle” “Is there a sharp pain when you try to move it?” “Yes” “Ok, it might be broken, we’ll take you to the doctor.”
If the kid is expressing a certain kind of significant physical pain, or psychic pain, it’s quite appropriate for the parents to take this seriously. (Taking it seriously doesn’t mean always taking the first obvious action that comes to mind at the first sign of trouble.) What it’s best for them to do, in a certain range of situations, is the subject of the post.
> What it’s best for them to do, in a certain range of situations, is the subject of the post.
Exactly. Most of the decisions parents make for their children they don’t make for the sake of making decisions. They make them because parents are assumed to want the best for their child (i.e. something along the lines of: growing up happily, and then going on as grown adults that can lead a fulfilled life). You say it yourself in your own post: They’re making those decisions for a child’s own good.
To make the right decision, parents need to know what decision brings them closest to the ideal decision for the child’s well being. Putting the decisions on the parent isn’t supposed to be a shortcut to just get the decision out of the way, but for the parent to make a more informed decision with better long-term outcome than their child could at that moment.
Which is what information like this is for.
This seems like a weird way of understanding parenthood.
Parents very often – like all the time daily – as children what they want to do or what they like or care about, and help them in fostering those interests and pursuing those goals. Whether that means asking what movie they want to watch or what sport they want to play or what friends they want to visit.
Yes, sometimes kids want things that are impractical or dangerous, and parents have to use their better judgement to make those decisions instead. This does not generalize to meaning that children never have any agency of any kind and that their wishes should always be ignored.
Furthermore, with regards to parents using their better judgement, this reading is precisely about helping adults develop their knowledge and beliefs about when and in what ways children should or shouldn’t be allowed to transition.
You listed three examples in which the answer to the question “which course is best for the child” is obvious next to one in which the answer so non-obvious that there’s a SSC Adversarial Collaboration Contest on it.
The only bar to the ACC was finishing the exercise.
The article seems to allude and hint to the idea that I have in mind, but not do much with it, so I’ll go and explain it…
I was raised with the idea that gender roles were mostly outdated and silly, and certainly that enforcing them was a bad thing. As a biological male, I have many male-typical interests, but a few that are probably considered female-typical (e.g. I like soft clothing, I seem to have a soft spot for romance stories), and a few that are probably just “weird”. I tended to let my hair grow long (mostly because I disliked haircuts), and when, occasionally, some kids said I looked like a girl, I laughed contemptuously at them for being stupid (for thinking that hair length = gender, or whatever). I was proud of not letting other people’s opinions control what I did. Incidentally, I scored 34 out of 50 on the online autism scale from an SSC survey—just barely inside the “autistic” range.
Anyway, I’m wondering if general acceptance of the idea “you can be a certain biological gender without feeling any obligation to exhibit any of the particular traits—behavior, appearance, interests—that others associate with your gender” would relieve the difficulties for some of these children. (The Samoan example is quite interesting—it seems like there is full acceptance of a certain kind of biological males who mostly act female. I wonder if there is still some pressure to fit a particular mold of fa’afafine.) There is already a word for some kind of male-behavior-exhibiting biological female in the U.S.; I searched the text of the page for “tomboy” but didn’t find it. I’ve heard there is less acceptance for the mirror equivalent.
Do the authors think that promoting the above idea is likely to help some of these children?
Don’t really have anything to add, but I think this is a really important point.
Does anyone know what the point of ‘gender’ is? It just looks like a bunch of stereotypes. Let people have their own pronouns, nobody cares. But sport, health services, etc. depend on sex, not gender.
Most trans people hormonally transition. Trans people who hormonally transition aren’t straightforwardly one sex or the other. For example, hormonally transitioning trans women (trans people going from male to female) are at elevated risk of breast cancer compared to cis men, because they have far more breast tissue. For certain labs (such as creatinine, hemoglobin, and alkaline phosphatase), hormonally transitioning trans men’s normal range is the same as cis men’s. Conversely, of course, trans women are at no risk of uterus cancer and trans men are at no risk of prostate cancer.
A doctor who acts like a hormonally transitioning trans person is like a cisgender person of the same birth sex may hurt their patient, the same way that treating a cisgender man as a cisgender woman would hurt their patient. Ideally, trans people should get their medical care from a person with expertise in transgender health and an understanding of our complicated bodies.
Similarly, it is genuinely unfair to cis women to have hormonally transitioning trans men on the same sports teams as they are– and, yes, that has happened. Trans women are a more difficult case and the appropriate policy may have to be sport-specific.
What definition of “trans people” are you using here, and do you have any numbers for this? Last time I looked, I couldn’t find anything I trusted for the US, and one seemingly-reputable data source for the Netherlands indicated that people who self-identified as transgender were roughly an order of magnitude more common than people who were receiving hormonal therapy. But, at least in the English version, I’m not absolutely certain “receiving hormonal therapy” included post-transition maintenance.
If by “trans people” you mean people who are more than just socially trans and that of these hormones alone are more common than hormones+surgery, that seems fairly certain. But I’m persistently curious as to what fraction of people who identify as trans, either have or likely will transition at least hormonally. And you’re one of the experts here, where I’m not curious enought to spend a great deal of time digging into the research.
Unfortunately, I’m not aware of any statistics. I’m simply basing it on my own experience. But I have several reasons to expect that the hormonal treatment rate is very high: for example, many trans people recommend a brief
one-to-two-month course of hormones as a way to diagnose the subtler manifestations of gender dysphoria.
I am excluding what you might call “lowkey nonbinary” people, who use ‘they’ pronouns in approving social circles but switch to the pronouns of their assigned gender among family and in the workplace. I’m not certain, but I suspect that lowkey nonbinary people might outnumber those of us with more significant dysphoria, particularly if you count all the people who would be lowkey nonbinary if they had a more trans-positive social group than they actually do. But I think that their experiences are different enough from other trans people that it makes sense to exclude them in analyses like this.
I find “gender” unfathomable in this context. I can get that there exists a social construct called gender, consisting of culturally-dependent cues used to signal biological sex. Women wear lipstick, men wear suits, etc. There is also typical sexual orientation, and typical male or female traits like aggression vs. nurturing or what-have-you. But “gender” in this context doesn’t seem to refer to any of these things as such. It’s not intended to refer to underlying sex. If anything, these people want to have the cues while acknowledging that they’re false … or something? But having false cues renders the cues meaningless. I don’t see the point of it. It seems terribly incoherent.
I think this is sort of an example of Goodhart’s Law: sexual dimorphism and division of labor was probably one of the evolutionary features that made homo sapiens more successful than e.g. neanderthal, with the result that (or as a result of?) many developed a preference for individuals exhibiting strongly sexually dimorphic features and behaviours. This results in an incentive to try to emphasize and/or fake those signals getting embedded in culture.
Yep. It reminds me of that quote by Phillip K. Dick, “reality is that which, when you stop believing in it, doesn’t go away.”
I suspect that a lot (probably a minority, but a large one) of culturally constructed gender-associated traits are probably cultural manifestations of an underlying bio-psychological sex difference. For example, it is known that males’ sexuality is associated much more strongly with visible physical cues than females’. It’s also known that women in our culture tend to ornament themselves with, e.g., lipstick and fancy clothes. It seems plausible and even likely, from an evopsych perspective, that just as males tend to develop a sexual attention to visible female features, females tend to develop a preference for displaying and flattering their appearance. This would naturally be mediated by what a culture considers appropriate and attractive so, in our culture, it manifests as a desire to wear pretty dresses and lipstick. If we consider trans women to have female brains in male bodies (a flawed model, but good enough for this context), it’s natural that they would want these same things.
You don’t really need that complicated chain of reasoning, though. There’s enough cultural gender indoctrination that people have a pretty good idea of what things are women’s things vs. men’s things.
If you just assume that people “feel” a certain gender inside, and like it when their social gender (i.e., all the cultural stuff) matches their internal gender (which seems empirically to be the case; how would you feel about being forced to cross-dress, for example?), then that’s enough to explain trans people’s desire for the arbitrary, culturally-determined, gender-affiliated trappings.
That’s a lot of it yes. The feeling is less about enjoying lipstick for its own sake, it’s more about copying and competing with other females.
Self-imposed isolation away from too many feminine triggers helps to keep the feelings at bay.
Call it ‘mirror neurons’ if you like, but my subconscious mirrors females not males.
Not sure if you wanted a deep dive into philosophy on this one, but if you actually want a good answer to the question “what is gender and why”, you’ll probably need to go there. I started this comment trying to give a full treatment of the issue, but that became way too much, and I’ll probably dump all that thought on an open thread later. Let’s just say, there are a lot of views as to whether/why gender is important.
But to explicitly present a view you might not have considered, and one which very much takes gender to be more than a (potentially useful) stereotype, consider the Catholics. From Pope Francis’ Amoris Laetitia:
So, he’s not a fan of trans-ness. But more pertinently for your question: note the definition of gender as the “socio-cultural role of sex”, something he elsewhere summarizes as “difference and reciprocity in nature between man and woman…[which are] the anthropological basis of the family.” Francis thinks gender is important because he believes in robust gender roles, where women should act one way and men another, especially in how they behave toward one another (thus “reciprocity”).
So, there’s one motivation for conceiving of gender as more than a social construct: because you need it to undergird your gender roles. (I think this may even be the only justification for making it something other than a social construct; but I’ll save that argument for another day.)
As the Samoan example indicates, I think that living in a society where this was a generally accepted and expected proposition would help many of these children.
However, given that we live in a culture where there is low belief and even lower alief in this proposition, I’m not sure how much teaching this to individual children would help.
Especially for children who are more social or are more socially conscious/anxious, they will be quick to find the ways that gender shapes how others treat them and what expectations others have of them, and simply being told by their parents that these behaviors are silly may be of little comfort in the face of the difficulties they may have by trying to live outside the actual social conventions of their peers.
That said, I do think parents should try to teach their kids this proposition, on general principles of encouraging freedom of expression and acceptance. But I don’t think parents should rely on this teaching alone to help dysphoric children manage their distress.
AFAIK, certain preferences are strongly correlated with biological sex. These are just vague “preferences” and not specific “behaviours”, but still, statistically speaking we could expect men to be more interested in things and women to be more interested in people, as the homily goes. This means that most people will likely still cluster into recognizable genders based on sex, in the absence of strong social pressure to do the opposite.
This fact (if true) does not invalidate the idea of “you can be a tomboy or have long hair or whatever if you want to”, but it does cast doubt on the stronger statement “gender is pointless and everyone should be roughly homogeneous”.
There are statistical differences in the behaviours and preferences of men and women just as there are statistical differences in height.
However we don’t say that because 5’9” is more typical of men than women that anyone who is 5’9” is therefore male or that a man who is 5’4” is less manly.
I think a lot of people do perceive unusually short men as less “manly” and unusually tall women as less “feminine.”
A woman who is over 6 foot is often considered un-womanly, insulted, implied to be transgender… It wasn’t so long ago that tall adolescents were given growth blocking drugs to prevent this.
Short men get some flack as well, but the perception is more that they are weak or unattractive, rather than un-masculine.
My personal preference has always been for a more capacious acceptable range of behaviours for both men and women such that more people feel comfortable both “being themselves” and identifying with what it says on their birth certificate. But having some kind of “third sex” like the South Asian hijra might also be a helpful solution–could possibly reduce gender dysphoria if there were more accepted categories people could slot themselves into, maybe even if those categories were somewhat looked down upon relative to “manly men” and “feminine women.”
My personal feeling, were a child of mine to suffer gender dysphoria, is that it would depend entirely on the severity and persistence of those feelings, in addition to my sense of that individual child’s personality and feelings (“dad gut” as one of the links describes it) whether I encouraged or discouraged transition.
If, for example, I had a son who felt, persistently, deeply that he should have a woman’s body, then I might encourage transition (social to begin with); but if I had a son who simply liked tea parties and ponies and wearing dresses and who wondered if that didn’t make him a woman, since only women like those things, I’d rather just tell him “not only women like those things; it is possible to be a boy and like tea parties and ponies and dresses.”
I’d rather just tell him “not only women like those things; it is possible to be a boy and like tea parties and ponies and dresses.”
Indeed. I’m a very, very cis male, with very typical masculine interests, (guns! monster trucks! grilling steaks!) and I’ve designed a number of “male dresses” (though, uh, being me, with my terrible completion rate, I’ve never actually made any of them) based off a sort of BDU design (so, really, females will probably flock if I ever actually make these things, because hey, pockets on a dress!)
I’m not sure it would actually be practical, but I’m thinking of it as a sort of jumpsuit version of a utilikilt. 😀
I mean, I guess if I was worried about it I could call it a “masculine one-piece unbifurcated garment”, instead of a “dress”. 😛
—
TLDR; If you wanna wear dresses, knock yourself out.
@localdeity:
There is in the article an example of a boy, C.J., whose parents tried the approach suggested by you – they let him be as gender-nonconforming as he liked, but didn’t socially transition him officially:
His story told by his mother:
https://raisingmyrainbow.com/2015/10/08/trust-your-mom-gut/
And by himself:
https://raisingmyrainbow.com/2017/08/24/inside-the-head-of-a-gender-creative-boy/
It seems it worked for him. Although, of course, the boy was sometimes bullied by some classmates who said he is gay. Maybe such approach works better for girls – tomboys are more accepted than efeminate boys.
A hundred years ago, this “problem” didn’t exist. Where gender roles stronger or weaker back then?
@Alexander Turok, we have records of transgender people even in ancient history. The problem of hormonal transition didn’t exist 100 years ago because medical science has advanced since then. https://en.m.wikipedia.org/wiki/Transgender_history
While certainly not fitting Western 1950s conceptions, a lot of those examples seem kind of like stretching current classifications over pretty distinct past behaviors or broadening the current rough idea in order to encompass behavior we don’t even see today.
It’s not even clear it makes sense to say all those times and places in the past had similar categorizations to ideas like hetero- or homo- sexual or cis- or trans- gender. The modern west doesn’t really approve of pederasty or eunuchs, but a lot of different past cultures had these classes/behaviors. Or in relatively recent times, the Sambia of New Guinea have manhood rituals that involve pre-pubescent boys ingesting semen.
Anyways, my point is sexual behavior and categories can vary a lot, but the modern western progressive conception of sexuality and gender doesn’t really seem well suited to applying to a multitude of distinct rather distant past cultures even if it’s somewhat broader than the modern conservative conception of sexuality and gender.
Nonetheless, it disproves Alexander Turok’s assertion that the problem didn’t exist. The “problem” perhaps was less historically visible because elder civilizations had these solutions in place.
So even if these solutions don’t match the current models of gender and sex, it at least implies that there will always be a GNC “problem,” and that it must be acknowledged and addressed in some way.
A little bit, but I mostly disagree that there’s much of a unifying thread to GNC throughout history given that the norms of sexuality move. By Western conceptions, almost every male of the Sambia would be homosexual when very young, then homosexual in a different way when a little older (arguably someone’s being abusive by Western standards), then heterosexual. I doubt this is because the Sambia have elevated genetic tendencies towards this specific pattern. I don’t think there is some “problem” they are solving. If you adopted a bunch of Sambians as babies and they grew up somewhere else, I think you’d find the distribution of their sexual behavior looked roughly like the culture they grew up in. Vice versa if the Sambians adopted some non-Sambians.
Similarly for the less strange examples that are more of an outlier of their culture like eunuchs or crossdressing priests that presented as opposite of their birth sex.
I think a more accurate reading of the evidence is that human sexuality is more plastic than conservatives or progressives would like to admit. Very little biological “problem” is being solved by any given idea of sexuality or gender. A lot of it is self-referential.
I think we have almost no understanding of what the dominant factors are and little more than a collection of outlier examples and a bunch of poorly understood dynamics.
@quanta413:
I don’t think it’s that hard to see the “problem” this rite is “solving”. “Problem”: teen boys want sex and don’t have access (or success) to girls. “Solution”: they use those younger boys instead. In many places and circumstances when men/boys were isolated from women, either physically or culturally, some used younger men/boys as substitute for women. The younger the better, preferably teens (less facial hair, less difference from women) => pederasty. It happened in prisons (it still happens), in monasteries (including Buddhist Tibetan monks), in English boarding schools, on ships etc. It happened in ancient Greek culture, where women were quite restricted to gynaeceums but boys practiced sports naked, it happened in some muslim societies (like Turkey or Afghanistan) where teen boy dancers were very sought for. Of course, those men weren’t true homosexuals – and frequently neither were the boys (sometimes poor or slaves) who as adults ceased to do it (or did it in the active role). In such societies – like in prisons today – it wasn’t considered shameful or abnormal to have sex with men, if you were the active part.
But other examples from that Wikipedia link seem really similar to the transgenders discussed here: the Hijra in India, the berdache (two-spirit) among Native Americans and the fa’afafine in Samoa (the last discussed in the article). They not only have sex with men, but really assume the dress of women and more or less of their social role, and do it willingly (afaik).
I don’t find your explanation about the Sambia convincing; it’s a just-so story. Most cultures teen boys didn’t or don’t have much sex. Modern westerners were outliers although maybe not anymore. Most cultures whose teen boys aren’t having much sex also don’t have their ten year old boys fellate older boys. It’s closer to pedophilia than pederasty by most standards. If the “problem” you mentioned was all that had to be solved, they’d masturbate. Hardly a new practice.
Mapping fa’afafine to “transgender” or vice-versa seems like a mistake judging by wikipedia. It covers men who present as masculine or feminine and who sexually are homosexual to bisexual. At best you can map many western things to one Samoan thing.
The article on two-spirit is less specific and maps even less distinctly to modern progressive western ideas. Hijra are a separate caste/religion/sexuality/gender.
Notably, two of these three groups articles make no mention of body modification which while not required to be transgender in the modern sense, is common. And body modification is not some weird impossibility without modern technology. Castration is a really, really old practice.
I think calling these groups gender non conforming makes sense, but not grouping them under transgender which has more specific denotations and connotations not matched by these groups.
Judging by the paper linked in our article, mapping fa’afafine to former feminine boys (gender dysphoric children, informally known as transgender children) seems correct – see the quotes in this comment:
https://slatestarcodex.com/2018/09/08/acc-entry-should-transgender-children-transition/#comment-669144
Among Western feminine boys, some persist and some desist, becoming homosexual men, a few (rarely) even heterosexual men. Among fa’afafine, it seems nobody desists returning to the male role, but they vary in their degree of feminity/masculinity as adults, like the Western ones. So it seems there is the same underlying biological phenomenon expressed in different forms in different cultures.
What about the dutch study which found that natal males allowed to partially socially transition as kids almost always persisted, while those who were not allowed often desisted?
https://www.sciencedirect.com/science/article/pii/S0890856713001871
Also some of the statistics for discussed in this post strike me as irrelevant because they fail to distinguish between late-onset and early-onset gender dysphoria.
I actually don’t like that phrase, but I don’t know how to say it better. (I’m not a native English speaker, so my “adversary” wrote most of the article.) Maybe:
“There is no solid/conclusive/definitive evidence yet that social transitioning increases the rate that gender dysphoria persists or desists.”
Steensma et al.(2013), mentioned by you, offers some evidence – all socially transitioned children became persisters – but it could be argued that maybe those who socially transitioned were those with the strongest GID.
You mean the statistics about suicide and mental health of adult transgenders? Those statistics, especially the one with 41% suicide attempts, are referred a lot in the debates about transition, we couldn’t ignore them. I don’t know a large study about transgender suicide and mental health that separates between early-onset and late-onset – do you?
Initially I wanted to touch the problem of the differences between early-onset and late-onset MTF in the article, but we already had to much material to cover (the article has 11 pages).
The 41% trans suicide attempt rate: A tale of flawed data and lazy journalists:
@Scott: do you want to add in the boilerplate paragraph about this being an entry to the contest? (The other entries have it, and not everyone will know what “ACC ENTRY” in the post title refers to.)
Oh, right, forgot! Thanks!