
Official statistics say we are winning the War on Cancer. Cancer incidence rates, mortality rates, and five-year-survival rates have generally been moving in the right direction over the past few decades.
More skeptical people offer an alternate narrative. Cancer incidence and mortality rates are increasing for some cancers. They are decreasing for others, but the credit goes to social factors like smoking cessation and not to medical advances. Survival rates are increasing only because cancers are getting detected earlier. Suppose a certain cancer is untreatable and will kill you in ten years. If it’s always discovered after seven years, five-year-survival-rate will be 0%. If it’s always discovered after two years, five-year-survival-rate will be 100%. Better screening can shift the percent of cases discovered after seven years vs. two years, and so shift the five-year-survival rate, but the same number of people will be dying of cancer as ever.
This post tries to figure out which narrative is more accurate.
First, incidence of cancer:
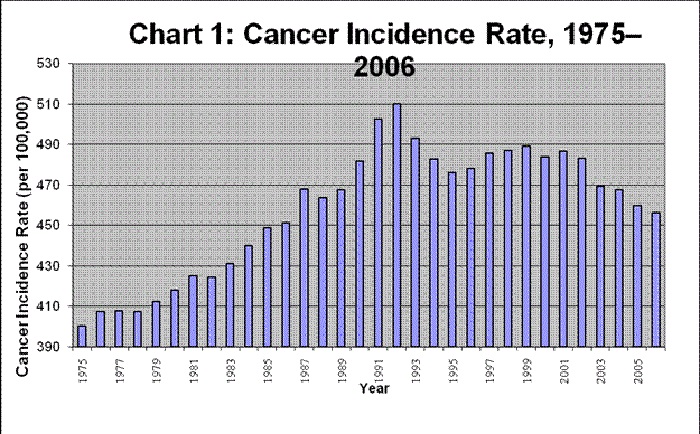
This chart doesn’t look good (in both senses of a chart not looking good – seriously, put some pride into your work). Although there’s a positive trend since 2001, it’s overwhelmed by a general worsening since 1975. But this isn’t the right way to look at things: average age has increased since 1975. Since older people are at higher risk of cancer, an older population will look like higher cancer rates. Also, something has to kill you, so if other issues like violent crime or heart disease get better, it will look like a higher cancer rate.
Here’s a better graph:
This is adjusted for age. I’ve switched from incidence rates to death rates, which is bad, but I can’t find good age-adjusted incidence data. Also, notice that this graph truncates its y-axis differently than the other. Still, it shows a similar pattern of adjusted death rates getting worse until 1990 and better thereafter. Why?
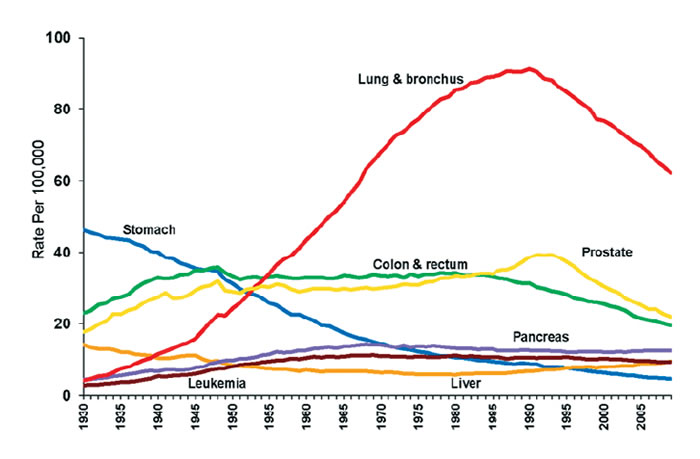
Smoking! That graph is just this one plus a 20-to-30-year delay:
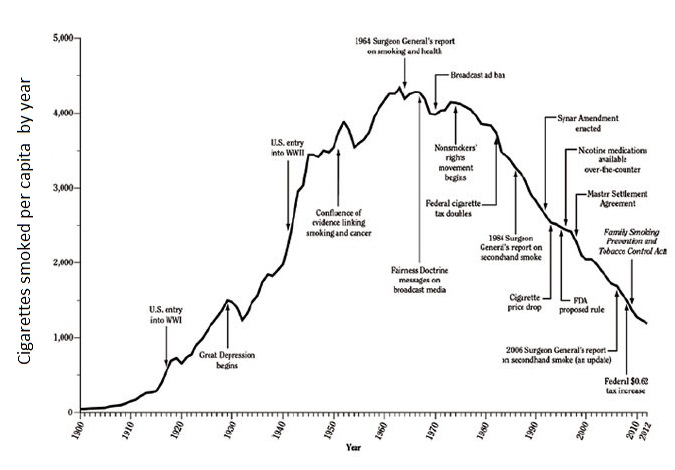
Through the first half of the twentieth century, improved tobacco-making technology, increased wealth, and better advertising caused order-of-magnitude increases in smoking. It takes on average a few decades for smoking to cause lung cancer, so there’s a peak in cancer (overwhelmingly driven by lung cancer) with a few-decade delay from the smoking graph. As smoking started to decline, so did lung cancer.
What about the other striking increase on the incidence graph, that of prostate cancer? In the late 1980s, guideline-making bodies suggested that doctors test harder for prostate cancers; doctors followed the recommendation, detected every little tiny irrelevant prostate tumor, and treated patients aggressively for cancers that never would have affected them before they died of something else. In the late 1990s, guideline-making bodies admitted this had been a bad idea, made the opposite recommendation, and people stopped diagnosing prostate cancer as often. If you look at incidence rates, that spike is much bigger. I’m not sure why this shows up on death rates, but perhaps the treatment itself contributed to mortality, or perhaps coroners were biased to attribute a death to prostate cancer if they knew the cancer was present.
Meanwhile, stomach cancer has declined dramatically; different sources attribute this to improved treatment for the cancer-causing stomach bacterium h. pylori, improved food processing methods, and increased vitamin C. Colon cancer is decreasing because colonoscopies remove more pre-cancerous polyps. Liver cancer increased because of a hepatitis C epidemic. A few other cancers are increasing or declining for similarly diverse reasons.
But overall cancer incidence and death rates increased up to 1990 and have declined thereafter. Pretty much everyone attributes the bulk of the decreasing death rate to improved prevention. If improved cancer treatment is contributing, it’s swamped by the social factors and we can’t see it in these data.
The most common method for measuring the effect of improved cancer treatment is the five-year survival rate – what percent of people survive five years after being diagnosed with cancer? Here are the relevant data (source):
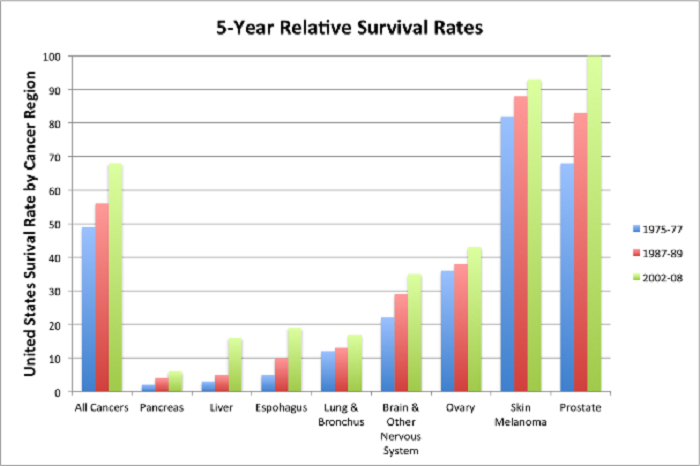
This is the best graph I can find, but it unfortunately leaves out breast cancer, colon cancer, and several other major cancers where we’ve made important advances. It’s from 2008, but the trends shown have continued since then. Note that change in the “All Cancers” category also reflects changing distribution of sites.
That looks like progress. But this is where the early diagnosis concerns come in. They’re best expressed by Welch, Schwartz, and Woloshin, who find that among different types of cancer, secular decreases in five-year-survival-rate are not correlated at all with improvement in the cancer death rate, but they are very correlated with change in the incidence rate. In other words, why are people living longer after being diagnosed with cancer? It can’t be because we’re treating the cancer successfully – if it were, they would be linked to decreases in the number of people dying of cancer. But it must be because we’re detecting more cases of small cancers too minor or slow-growing to kill people quickly (“lead-time bias” and “length bias”), which shows up as increases in the cancer detection rate.
This study does not prove that cancer treatment is not improving. It just shows that five-year-survival-rates do not in and of themselves provide evidence for improving cancer treatment. Any signal from improving cancer treatment is drowned out by the signal from improved detection.
How do we get around this? One possibility is to investigate change in stage-specific survival rates. That is, doctors classify cancers by stage, all the way from very early poorly-developed cancers with good prognosis to very advanced cancers with bad prognosis. A lead-time bias or length bias would show up as cancers being detected at an earlier stage. So if we found that more people were surviving even within each bin of “stage at which the cancer was detected”, this would be strong evidence that cancer treatment really is getting better.
Several groups have looked into this. The best data comes from the government’s national cancer statistics clearinghouse at SEER (source):
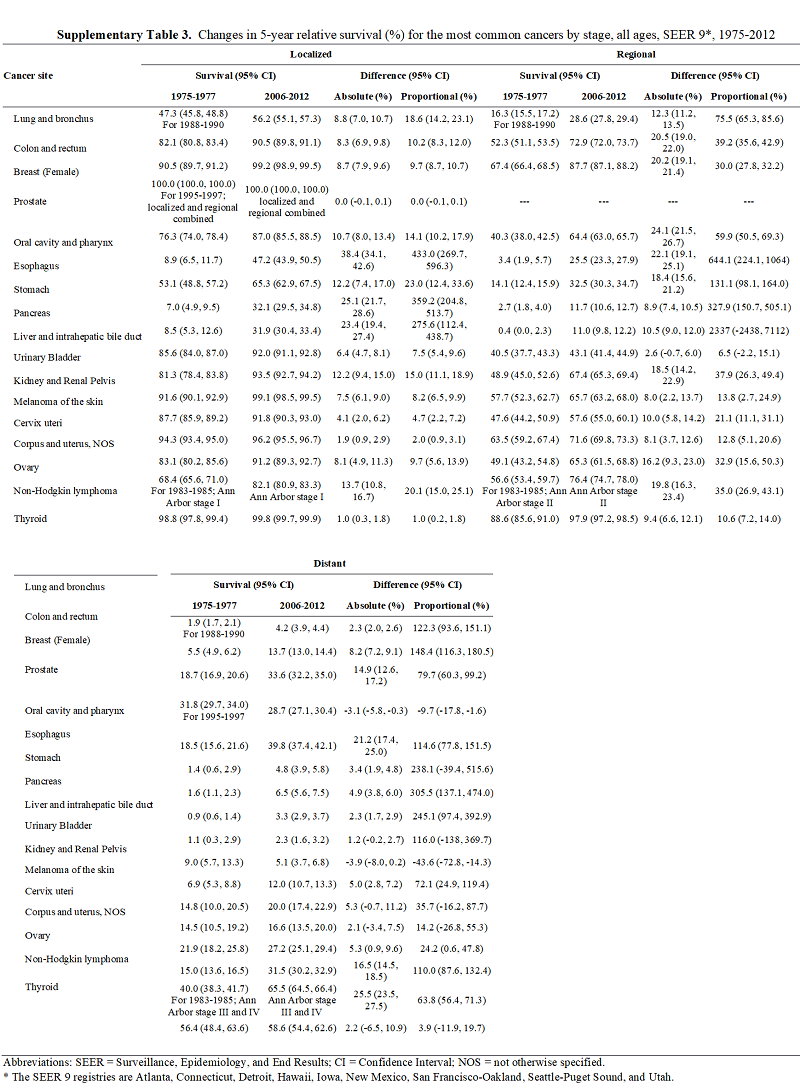
Even within each stage, five-year-survival-rate has increased significantly from 1975 to 2012.
Closer investigations of specific cancers are similar. Stage-adjusted cervical cancer risk and colon cancer risk both show most of the modern gains in survival rate persisting.
But maybe stages are too big a bin to serve as a useful proxy. Imagine a study that wanted to prove that having more cars made you happier. They do a survey and find that people with more cars are happier, but someone objects that maybe wealthy people have more cars and wealth makes you happier. Imagine that their response is to separate people into two bins: “poor people” who make below $50K and “rich people” who make more. They find that even within each bin, cars still make you happier. But this is just a problem of too few bins: a person making $10K is still very different from a person making $40K (and likely to have fewer cars). The attempt to remove confounding with bins fails. These cancer studies generally use only a few broad stages; might this be allowing effects from early diagnosis to creep back in?
Elkin, Hudis, Begg & Schrag look into this. They find that within each stage, tumors have gotten smaller since 1975, suggesting that the staging system isn’t capturing everything we care about regarding cancer. But they find that even when adjusted for size, some of the stage-specific modern gains in cancer survival still remain. In particular, decreasing size explains 61% of improved survival in localized-stage breast cancer, and 28% of improved survival in regional-stage breast cancer. Another study on breast cancer does a similar adjustment with other ways of classifying cancer and concludes that “improvements were shown irrespective of tumor size, lymph node status, and ER status” and “the impact of screening was by nature of limited magnitude. The modified treatment strategies implemented by the use of nationwide guidelines seemed to have a major impact on the substantial survival improvements.” Another group does a simulation and finds that it’s implausible that screening-related biases are the entire source of improved survival:
The results from our study suggest that lead-time bias introduced by mammography screening does not explain the survival improvement observed during the recent decades in the Nordic countries. The absolute as well as relative bias was generally small, and much smaller than the observed increase in relative survival between 1964-2003. However, in some settings the absolute bias reached 4.0-5.7 percentage points, on a survival around 68-77%, a difference that many would see as an interesting improvement in survival.
A lot of this work has been done in breast cancer, probably because it’s had a strong push for screening recently. We would expect screening to be even less important in other cancers, but there hasn’t been as much work on it. One exception is Tong et al, who find that changes in tumor stage and size explain only 20% of improved survival rates in colon cancer, but advancements in therapy explain about 71%. Separately, an authoritative-sounding collection of colon cancer experts express their opinion that “it is possible that within-stage migration had some effect on our findings, but it is implausible as the major source of the trends we observe.”
The only contrary data point I can find is this study of laryngeal cancer, which finds worsening stage-specific survival rates for high-stage laryngeal cancer since 1977. However, the study authors note this was the only one of 24 cancer types examined to show decreasing survival rates. They speculate that maybe some kind of change in smoking behavior over this period has changed the nature of laryngeal carcinomas to favor a more aggressive type. They don’t really have any evidence for this, but given that this is the only one of 24 cancer types to show a decrease in survival rate, it’s probably something at least that unique, and doesn’t indicate a general failure in cancer treatment.
There could still be unobserved confounders. Stage alone wasn’t enough, but merely adding size to stage might still not be enough. Even the papers that look at a few more esoteric things like receptor status might not be enough. All we can say with certainty is that right now, adjusting for everything we know about and are able to monitor, cancer survival rates still seem to have increased. Tomorrow we might discover new confounders that take that away from us, but right now there is no particular reason to expect that we should.
So: age-adjusted cancer incidence rates and death rates have been going down since 1990, primarily due to better social policies like discouraging smoking. Five-year-survival rates have been gradually improving since at least 1970, on average by maybe about 10% though this depends on severity. Although some of this is confounded by improved screening, this is unlikely to explain more than about 20-50% of the effect. The remainder is probably a real improvement in treatment. Whether or not this level of gradual improvement is enough to represent “winning” the War on Cancer, it at least demonstrates a non-zero amount of progress.
I don’t want to frame this in terms of “here we DEMOLISH the pseudoscientific narrative that cancer progress is weak”. Many of the people I know who critique this research are from an older generation. They remember Nixon assuring them at the very beginning of the War on Cancer that we would have a cure within five years. If they’re really old, maybe they remember victories of that scale over polio and smallpox. If those were their hopes, it’s right for them to feel disappointed. But I come from a generation that doesn’t expect much, and I think the evidence suggests my low expectations have more or less been met.
















Thanks for the insight sclmlw. The fact that cancer research might have had a lot of positive externalities definitely shifts me a bit in the direction of more optimism about how much we are getting for our spending.
However, if we are trying to answer the question: “how much have we gotten for our trillion dollars that we spent as a result of launching the war on cancer?”, I don’t think it’s fair to give the the war full credit for all benefits incidental to basic research. First, I was assuming half of that trillion went to screening, and treatment (probably a very low estimate). Then out of the research half, I imagine that a grant-making body that is targeting research will tend to give a majority of funding to things that test actually procedures, not basic research. I would also imagine that even out of the basic research part, a lot of it would be about stuff that doesn’t really generalize to other diseases. So it seems likely that maybe only 10% of that trillion really has a shot of having positive externalities (I would actually be curious to know your estimate on this, since you are in the field). Since cancer funding very likely crowded out other medical funding over the past few decades, it’s possible that without the war we would have gotten more than this 10% of generalizable basic research out of that spending. And even if we would have gotten only 5% otherwise, that still leaves you with 950 billion of marginal dollars spent without positive externalities to justify just based on net lives saved.
I would also question your idea that curing a very rare disease saves an infinite number of lives on the margin. The first problem is that you have to apply some discount to future lives (mostly just because there is a good chance the human species, or at least the cure you invented, disappears on any given year), and the sum of this kind of geometric series is finite. The second problem is that this disease would likely have been cured anyway eventually, so you only get credit for how much sooner cancer research made it curable. The third problem is that using the money to just pay down national debt and using the interest savings to save lives on highways and the like (as I suggested in my rough cost analysis), also saves lives for an indefinite future, so it’s not clear that the externalities you mention are larger than the costs.
All that being said, I do appreciate your basic point that cancer research has been good for medicine. But I would be curious to hear your informed opinion of the likelihood of my general concerns about the war on cancer turning out to be true:
1. That for each quality adjusted life year better cancer treatments provide, they destroy more than one by submitting a bunch of people to very unpleasant procedures from which many turn out to get no benefit, and by submitting a bunch of people to a lot of unnecessary stress and procedures due to false positive in screening.
2. That for each new innovative type of procedure that does a lot of good, there is one that is going to turn out to have been way overprescribed or based on faulty medical trials (as many operations and medicines appear to currently be).
3. That even the good innovative procedures will turn out to have long term costs we don’t appreciate that wash out most of the perceived benefit (like increased CVD risk for everyone that undertakes them, even those who wouldn’t have died from the cancer in the world without the new treatment).
A few thoughts on how the story about our success in the war against cancer might not be quite as good as age-adjusted cancer mortality declines might suggest:
1. You mention that two of the biggest declines in mortality occurred in types of cancer where the improvement is potentially driven by environmental effects: lung cancer (obviously) and stomach cancer (maybe preservatives). What if the other major declines also turn out to be environmental? Maybe prostate cancer is just declining testosterone in men in the United States, and breast cancer has something to do with declining use of hormone replacement therapy or certain forms of birth control. On the uglier side of environmental effects could be those that cause increases in liver and pancreatic cancer, those just happen to be less prevalent in the general population by a stroke of luck. If the story really is almost all environmental, all the money we spent fighting the war, developing screening and treatment, would have been wasted.
2. There seem to be some studies suggesting that cancer treatments tend to increase risk of cardio vascular disease. What if it turns out that all of the increased treatment we do for potentially not-fatal cancers cause enough CVD deaths to offset the gains we get in declining cancer mortality (to make the math on this possible you would probably need to focus on non-lung and non-stomach cancers, since those are the cancers that appear to clearly benefit from treatment)?
3. Is it possible that for every quality-adjusted life year we add to some patient treated with cancer, we ruin the quality of 10 life years of other patients who were treated, and didn’t benefit much at all?
4. Let’s say we’ve spent a trillion dollars on cancer research, additional preventative screening and additional cancer treatment over the past three decades (in 2018 dollars, just an extremely rough estimate for the sake of argument). And lets say that once we really factor out all confounds, we find out that this war on cancer averted 100,000 deaths, at an average cost of 10 million per life. During that period, the Harvard Center for Risk Analysis found that the “median cost for lifesaving expenditures and regulations by the U.S. government in the health care, residential, transportation, and occupational areas ranges from about $1 million to $3 million spent per life saved in today’s dollars.” Let’s say we had used that trillion dollars to gradually pay down some national debt, save the federal government a few percent a year on it, and use the resulting say 20 billion per year on average to save 10,000 lives each year. So that would be a total number of lives saved several times greater (over the course of a few decades) than the war on cancer, and most of those lives saved would be much younger and healthier than the ones saved from cancer. So in terms of opportunity cost, it’s still possible that we didn’t do so well in the war, even if we did save many lives.
You make some very good points overall. I would like to comment on one thing…
> Maybe prostate cancer is just declining testosterone in men in the United States
The relationship between Prostate Cancer (PCa) and testosterone seems to be fairly complex. While eunuchs do not get prostate cancer because of a severely atrophied prostate, and hormone ablation therapy can temporarily defer the growth of a PCa, within the normal range there seems if anything to be an inverse relationship between testosterone and prostate cancer risk.
In addition there seems possibly to be a relationship with higher estrogen levels in men and prostate cancer. This may explain the link with obesity, which enhances conversion of testosterone to PCa.
Increasing obesity seems to be a factor that should be increasing the risk of PCa.
In a sense, it is all environmental. Cancer is cells mutating in a way that allows them to spread in a harmful manner. Many things cause this to happen, and environment certainly contributes. But there is basically never a clear cause. Smoking releases chemicals into the lungs that cause mutations, which could cause cancer. But some smokers never end up with harmful mutations; others had a genetic predisposition aggravated by the smoking, and some may have gotten it solely because of smoking, but it’s hard to tell. In the end, it mostly comes down to a matter of luck and, more so, time. The longer you live, the higher the risk of a harmful mutation. Environment plays a role, but cancer doesn’t really need a trigger – it’s just the way the body works – it a combination of normal processes compounding in a way that makes the result very abnormal. Sometimes the way the body works ends up being a serious problem. Autoimmune conditions would be one example – the immune system is doing what it is supposed to, but somewhere along the way it gets screwed up. You’re supposed to have wisdom teeth, but now that we don’t lose other teeth by that time, the result is a problem. You could classify this all as environment – living in a time where we have teeth, living to be unusually old, and possibly in the case of some cancers that affect women, not being constantly pregnant or breastfeeding.
I agree that most cancer treatments (and old age care) completely fail a larger cost-benefit analysis, which is why I think medicine will be socialized. It simply is not sustainable because it will never be profitable to spend that much on a significant number of people, and because it invests so much on people who are often already in poor health and whose quality of life will often not be good regardless. Of course, on a personal level, saving or lengthening people’s lives can be priceless. But the increasing life expectancy is a huge problem on many levels.
@mtl1882
I agree that in a sense that all cancer causes are environmental. I was just trying to suggest that what’s causing the decline in cancer mortality might be environmental (in the sense of non-medical causes from the general environment), rather than intentional better treatment of cancer resulting from research.
I am interested in your idea that old age care fails a larger cost-benefit analysis. I partially agree, but I have a few problems with it:
1. Here is a post about a paper suggesting that even though we spend a lot of money on people who are about to die, most of those people actually had a very good chance of surviving at the time the decision to spend money was made. So it’s possible that even with an optimal system, we would still have to spend as large a share as we do on old age care (since many of those people have another good ten years to live).
2. We are a pretty wealthy society. If you ask me whether we should invest the marginal trillion of our wealth in continuing to increase the number of bedrooms the average family has or in trying to get an extra year of life for old people, i would choose the latter.
3. Why is it not sustainable? In my guess about the future more and more jobs will be automated, the outputs of those industries will become very cheap, and we will end up devoting a majority of our man-hours and GDP to Education and Medicine. Currently, medicine is 1/6 of CDP, why can’t it eventually be 1/3?
As a cancer researcher, I’m curious as to what most people’s perception is on money spent on cancer research. For example, how would you answer the question: “If we don’t cure cancer in the next 30 years, would you consider the money spent on cancer research to have been wasted?”
Of course, this implies that the last 30 years of cancer research were – at least to the degree that all cancer has not been cured – wasted. From a clinical perspective, this seems ridiculous, since it’s clear that we’ve made improvements to the treatment of a number of cancer types that used to be basically untreatable. But from the perspective of basic understanding, cancer research has often felt like just better understanding how human biology works – from a systems level, all the way down to a genetic level. The problem is that, due to the nature of the disease, improving cancer treatment has often been contingent on better understanding how cells work. So cancer research and basic research are effectively the same thing, such that in some ways it feels like, “when we finally understand the underlying biology from end to end we’ll have all the tools we need to cure cancer.”
Which, as I write that, sounds like a pipe dream. But the basic research is good for a lot of things besides cancer. Along the way, we learn how to treat/cure all sorts of rare diseases that otherwise would never have received enough research dollars to gain any traction. It’s not necessarily that rare disease is itself so rare; it’s that any one rare disease is pretty rare. So if you don’t stumble on an answer while researching something else, you’ll never figure it out with the kind of money people would be willing to donate to the task of understanding one specific rare disease. Well, cancer is the ultimate ‘something else’ we spend huge amounts of money researching. In that sense, I have this filter in my mind that translates “cancer research” to “cancer (and everything else) research”, but my impression is that for the general public, “cancer research” sounds like “that money hole we keep throwing a bunch of money into; we never get anywhere on it, but these clowns keep promising that something real will come of it”.
And it’s not that we don’t make any progress in treating cancer. Every year we get better at treating lots of sub-types of cancers a way that’s important but not very visible (for the same reason new rare disease treatments often don’t make the news – the number of people who currently have the condition is relatively small, but the future generations that will continuously benefit are uncountable if projected forward without bound). But I think that when we talk about this cost-benefit analysis I almost never hear about the knock-on effects of cancer research in pretty much any other area of biology you’re interested in improving understanding for. (i.e. transplant biology, rare disease, asthma, psoriasis, infectious disease, neurological conditions, aging, etc.)
[H]ow would you answer the question: “If we don’t cure cancer in the next 30 years, would you consider the money spent on cancer research to have been wasted?”
If it were a poll, I would get angry at the poll designer for yet again asking something that only vaguely reflects the thinking of the participants.
First: any tough problem has large numbers of potential answers. If you expended resources on ruling out 70% of them, no one is likely to consider those resources wasted, even if you still haven’t found the real answer.
Second, as you say, it’s possible to rule out no potential answers at all, but serendipitously solve several other valuable problems.
Third, as you also say, we know cancer is really a family of related problems, and we’ve actually solved some of those.
However, there is more to it than that. If the potential answers to “how do I cure cancer?” are infinite, then we could pour resources into it indefinitely and perhaps find a method that cures 90% of the known cancers (probably a big win), rule out 50% of the known methods but triple the number of leads we should have been trying (ambiguous), rule out 10% of the possible leads while the problem gets worse (probably a loss), or a mix of all three. And that’s without considering the possibility of corruption or gross mishandling of research that invalidates millions of dollars of work.
If research solves several other problems by serendipity, that might be worthwhile, but it might not. A solution that helps infinitely many people when projected forward without bound doesn’t necessarily justify the expense, because many such solutions offer the same infinite value, and some values increase faster than others. If I spend $40 million researching cancer and report I found nothing, but I did find a cure for dandruff, that doesn’t sound good at all if it turns out that $40M came out of someone else’s budget, and they could have used it to develop a cure for heart disease. And if it turns out that I said I was going to use it for cancer but my justification was really tenuous and I really just wanted to cure dandruff, I’d expect to never secure grant money again.
So if I had to answer such a question, I would be compelled to say “maybe”.
Pathologist here. I’m glad you break down by anatomic cancer type, but I would go further. “Cancer” is not one disease (kinda like grouping all mental illness into one category) and looking at overall cancer survival rates, the variance over time is entirely do to changes of incidence of cancers by anatomic location (of the most common types), as you point out, of course; in the same vein, “breast cancer” and “lymphoma”, etc., are not each one disease, but a grouping of different molecular diseases, and similar consequences for summary statistics. Simpson’s paradox is a bitch. Obviously would be outside the scope of this great post, but doing so one would see more of a bi-modal distribution of success, (different than the average low-but-positive progress you site), molecular diseases where treatment has been a smashing success (bordering on cures), and others where essentially zero progress has been made.
@sclmlw
You raise interesting points. You suggest cancer cells are a type separate from human type. But are cancer cells not mutated normal human type? So what allows the mutation apart from what promotes it? Another interesting point is the inter cell space. Cells do a trick.They stay apart but also congregate e.g. kidney cells stick together. This is done with molecular precision. If this process breaks down e.g. in joint disease or hernia, cells congregate with insufficient gaps and degeneration follows. What sort of force is required to keep cells apart but together? Why is this gap in biological knowledge not discussed?
It’s not that these questions aren’t being asked, and it’s not that these are gaps in biological knowledge that aren’t discussed among oncologists. I think it’s more just that you have to be sufficiently familiar with the literature to understand it. I’m not going to go into the various and complex types of cell adhesion molecules here. Check out any basic molecular cell biology textbook for that (seriously do, because they’re fascinating!). Sufficient to say, in order to leave your current organ, pass to the draining lymph node, leave the fast-moving environment of circulating blood, and invade new tissue, you have to tap into some complicated processes.
It might seem mysterious that cancer cells can do all these complex things at once. I’d recommend reading more about the epithelial-mesenchymal transition to get a better understanding of this. There is also active research into tumor-associated cells, such as fibroblasts and macrophages, that are recruited to do some of the work of the cancer cell.
Cancer research has required us to get serious about fundamentally understanding everything individual cells do, as well as figure out how they communicate with each other locally and distally. We are making progress at figuring out much better ways of treating cancer. It’s just that there has been this half-century period where we needed to discover the mechanisms behind how cellular, molecular, and systems biology work before we could start making more significant gains. We’ll get there, though. We really are making progress along many fronts, and much of the research we do for cancer dovetails directly into research for pretty much every other kind of human disease.
“It’s not that these questions aren’t being asked, and it’s not that these are gaps in biological knowledge that aren’t discussed among oncologists. I think it’s more just that you have to be sufficiently familiar with the literature to understand it.” Granted my basis is not research papers. My source is mainly texts such as Molecular Biology of the Cell, Alberts et al. There the question of cell separation is given a descriptive (adhesins) rather than operational explanations. I do not find those explanations persuasive. Maybe you can point me in a good direction./
I would like to suggest another hypothesis: if 5 year survival rates are not falling cancer treatments are MUCH more effective today.
This comes via several lines of thought.
First rewind to 1970. You are a 60 year old male. You have a heart attack. You die. Your neighbor lives to 65 and develops lymphoma. He gets treated with doxorubicin. He lives 5 years. 5-year survival rate is 100%. Now run the same scenario in 2013. You have a nice STEMI, make it to the cath lab, and come out. You survive the heart attack, but with some pathological remodeling. Your neighbor and you develop lymphoma at age 65. You both get doxorubicin. You develop heart failure (a known side effect of doxorubicin), you die after 3 years.
It is not just a question of survival rates getting jacked by people being older, we also have a lot more unhealthy people getting cancer. Very few of the major mortality drivers are things where “curing” them results in complete regaining of health. Survive a heart attack, well you can tolerate a lot less cardiotoxic chemotherapy. People with comorbidities die faster; cancer patients have more comorbidities to start with today because the comorbidities don’t kill them, but still reduce health. Remember chemotherapy is highly toxic and we routinely dose until you literally cannot tolerate more of the drug. Liver, heart, kidneys … any previous disease there can close off whole classes of chemotherapy. Or take organ transplants. We routinely save people with organ transplants and immunosuppression. Unfortunately immunosuppression increases some cancers incidence and also decreases the efficacy of chemotherapy.
And it is not just chemo. Radiation toleration goes down dramatically if you manage to live long enough with COPD to develop lung cancer. Surgery is less likely to cure if your immune system is weakened and cannot finish off the remaining microscopic cancer blebs that all but inevitably get missed.
But it is not just surviving things that killed us 50 years ago; we are also less healthy in many ways today. Take diabetes. In 1970 <2% of the US population as diabetic. Today we are looking at over 7%. Diabetics who get breast cancer have a 1.32 odds ratio of dying compared to non-diabetics. As the percentage of patients with diabetes goes up we should expect to see non-trivial drops in five-year survival for breast cancer. Obesity likewise increases mortality odds ratios of mortality are 1.4 for breast cancer and obesity.
As baseline health has fallen without a drop in survival rates, something else is going on. We can play similar games with exercise, with psychiatric comorbidity, and other general determinants of health.
Then there are the changes in society. Society has grown less religious. This is bad for cancer survival. Having "no religion" is extremely well correlated with decreased cancer survival. Maybe it has nothing to do with belief and everything to do with community. Well that sucks too. The bowling leagues, the unions, the civic societies, the neighborhood bloc associations, and pretty much all major social communities are in decline in the US. Fewer people are part of such a community than ever before. And this is not just the psychic benefit. Family and community are how a lot of cancer patients manage their treatment. Good luck driving on chemo. Or managing your intractable vomiting without someone else. As America has become more atomized with more adults living alone with fewer friends we should expect compliance with arduous chemotherapy regimens to fall.
Are there government programs? Sure. They kill people. Going home and having a spouse help you bath and manage your side effects when you are physically incapable of doing works a lot better than entering a community skilled care facility where you get all manner of fun nosocomial infections. Having people from church cook for you is much better than having Meals on Wheels come direct from another patient sick with opportunistic infections.
We know what general things really help with survival in all cancers: starting off healthy, eating a healthy diet, having good social support, getting the heck out of group care facilities ASAP, and having reasons to live (like grandkids). Which of these have improved in the last few decades?
So in light of all of this, I submit we should be celebrating no progress. 65 year old stage 1 cancer has the same 5-year survival rate? Great, somehow we have improved treatment so the increased number of heart failure patients don't drag the rate down. Somehow the large effect of obesity has been counteracted. Somehow we have gotten better at delivering care even as social support systems have frayed.
We are fighting the Red Queen and not falling behind! Hooray!
Even if the only progress against cancer were earlier detection and decreased carcinogen exposure, I don’t see why those shouldn’t count.
They certainly count, but it means we’re no better at treating cancer.
Given the trillions (?) spent on doing just that, an outcome of zero should maybe lead to some reprioritization!
What’s the deal with sun exposure? I feel like the messaging I got as a non-biology person in the 1990s was that sunscreen and proper sunglasses were going to do for skin cancer what smoking cessation did for lung cancer. Has that happened? And how does that play with all the new guidance on sunlight being good for Vitamin D, mental health, and myopia-prevention?
On a personal level I have had medical professionals tell me in the past year to (a) never go outside without sunscreen and (b) make sure I spend at least 20 minutes/day outside without sunglasses, preferably at noon. So clearly the sun exposure piece is more nuanced than the smoking cessation piece.
That’s completely unsurprising given that our (mostly skin) cells have always been adapting to getting hit by sunlight, but not our lungs to inhaling lots of particulate matter.
Possibly more particulate matter than you think, considering use of fire for heating. Still people weren’t inhaling that as deeply as possible.
What’s the ratio or weighting between cancers that are caused by lifestyle, diet, pollution, radiation and other external factors vs. cancers that arise solely from genetics or heredity?
Somewhat tongue-in-cheek, but those of us with comparative biology background already know the genetic tweak necessary to almost totally eliminate cancer: cold blood.
While “sharks don’t get cancer” is a lie, poikilothermic (“cold blooded”) animals show much, much lower rates, and cancers are usually associated with toxins and viral infections – spontaneous neoplasms are vanishingly rare in ectotherms. The mechanism is simple and obvious – less metabolic activity means less cellular damage and less turnover. The genetic changes necessary to make humans ectothermic wouldn’t be trivial, but the benefits would be enormous: 90% reduction in food consumption, increased lifespan, tremendously increased resistance to serious injury (tissues remain alive for hours or days even if deprived of blood), the ability to “hibernate” (technically brumate) for months on end (with even greater food savings), tremendously increased resistance to drowning/asphyxia etc. due to low O2 requirements, and more efficient conversion of food into biomass. The only downsides would be reduction in aerobic capacity and some increasing heating bills in places which, frankly, suck to live anyway. And without the risk of cancer, regeneration is easy – basically everything outside of mammals and birds regenerates to some degree.
There’s no reason to think it would compromise intelligence, either – while humans are uniquely smart, varanid lizards, crocodiles, cephalopods, and more show intellects comparable or above most endotherms (all of those listed show tool use and rapid learning), suggesting that the few extra-smart lineages like apes and corvids are products of tangentially related ecological factors (e.g. the pressure to consume more fuel for a wasteful metabolism).
It may be 50 years in the future, but I gotta say, cold is the way to go! Plus, who *doesn’t* want to be venomous?!
paging Peter Watts
Paging Erik Sprague
A huge percentage of resting metabolism is taken up by the human brain. Perhaps other species have evolved to get a lot of processing power from a cold brain, but humans clearly developed most processing power after going the warm route. I’m not convinced we can reverse-engineer from warm to cold without really screwing up a lot of mechanisms that developed under a strict expectation of warm-blooded conditions.
Your idea sounds good in theory, but I think instead of reversing from warm to cold, you’re going to have to start over and re-build a human from a cold-blooded starting place. Maybe if you built it all from scratch (or from a much more divergent starting place) you could avoid the myriad problems of the reversal approach. Meanwhile, I think “curing cancer” just sounded a lot more feasible, compared with “creating cold-blooded humans from scratch”.
Well, as I note below, “turning people into reptiles” is more the goal for me, with “curing cancer” being an excuse. 😉
That said, I don’t think it would be as hard as you think. Ectotherms generally have the same basic mechanisms we do, and many actually operate are fairly similar temperatures (or higher, in active predatory species in the tropics and deserts, which can exceed 45C field-active body temperature), so while there’s a few systems which would need to be additionally modified, in many cases we’d simply be rather overbuilt (e.g. more lung area than needed) but otherwise comparable to some of the extant herps with narrow thermal niches. Indeed, most human physiological processes can be slowed down tremendously via cold and still work without much trouble, as seen in cooling during surgery, cooling organs for transport before transplanting, and reviving people with hypothermia. In the last case, the biggest issue is the heart, but there’s actually a simple modification which solves that problem, and which will become widely known once my damn co-authors get their **** together so we can submit the damn paper.
Some people could undergo additional modification to become thermal generalists, but that comes at the cost of lower peak performance even at optimal temperatures, so I suspect that modification would be only marginally popular. The most popular physiological profile will likely be that of an active tropical species, combined with external heating mechanisms.
You have suddenly reminded me of the thing I read, probably in The Secret of Our Success, that humans have far less internal resistance to food poisoning and a much shorter digestive tract than most comparable animals — we have offloaded the responsibility for these to our culture, in the form of cooking and other food prep.
I wonder if clothing and HVAC might eventually cause evolution to conclude that we don’t actually need to be so very warm-blooded after all. (I know clothing is more a matter of preserving internally-generated heat — but I’ve actually seen clothing with a battery, to enhance that. Probably more on the way as battery tech improves.)
Well, some of our short digestive tract has to do with being more carnivorous than most other apes, both now and in the past (there’s a fair bit of anthro theory about how hunting and scavenging gave our brains the protein and fats needed to grow), and our immune systems in general are pretty weak because of how protected we are from most germs in the first place.
I doubt HVAC will be enough to lower our metabolisms, too. Mammals in tropical climates and/or stable climates still have high metabolisms, even if they can’t up-regulate or down-regulate it as far, in part because of the main benefit that led to warm blood (we think): higher aerobic metabolism. For reasons that are completely unknown, maximum aerobic metabolic rate is always ~10x basal metabolism, so increasing basal metabolism not only keeps you warm, it lets you engage in aerobic locomotion at higher speeds.
As far as is known, there are only two, maybe three cases of substantial and permanent down-shifting of the overall metabolic rate (versus temporary like hibernation). Sloths and manatees have low metabolisms in order to exploit a specific niche which relies on large quantities of poor quality food in a relatively isothermal environment. There’s also a contentious hypothesis that crocodilians used to be warm blooded and reverted to ectothermy to invade the niche of an efficient aquatic ambush predator (early crocs were small, agile, terrestrial, erect-walking creatures that looked very similar to early dinosaurs,and only later became the creatures they are today after the phytosaurs died out, plus crocs have 4-chambered hearts and weird respiratory systems consistent with a higher-metabolism animal). I’m not sure I buy it, but it’s intriguing.
So we’ll probably have to use some sort of technological fix in the end.
I can’t believe you’re turning a cancer discussion into one about turning people into very smart archosaurs, yet somehow here we are.
Yeah, that comic is basically how I approach the problem. “Curing cancer” is a good excuse for turning people into reptiles, because the single most robust scientific finding ever is that reptiles are 456,000% cooler than any other taxon.
Chiming in late, but just had to say: this is one of the most phenomenally ironic pieces of writing I’ve ever read. It’s g*dd*amn Shakespearean. Kudos, mate.
Obvious application – space colonization.
A question about cancer which I am guessing will not get much or any response and that is what really interests me. Cancer/tumors seem to be rogue cells. It is reasonable to ask why and to ask further what is is the organizing principle for the social behaviour of cells in an animal body.What are the constraints and why do different cell types obey different ones? To my knowledge there is virtually no discussion in that vein. Some basic patterns are easily apparent if you choose to look. Is there some taboo around this? A cynic might say that the current state of research/knowledge progress may be considered by some to be not all bad.
I recommend Bob Weinberg’s The Biology of Cancer for a better survey of our understanding of this subject. The best way to describe our understanding of this (what would you call it? The heirarchical enforcement mechanism of inter-cellular interactions, maybe?) is perhaps to call it emergent order. Nobody is really “in charge” in the sense of some overall governmental structure. There are multiple, redundant systems that govern enforcement of each step of the process. And there are systems that govern those systems and so on.
So, for example, say you’re a cell and you want to divide. Ignoring the myriad complexities of getting the signal to divide from your cellular milieu, you decide to just tell yourself “I’m ready for cell division.” Normally, the natural signalling mechanism will lead to phosphorylation of a protein called RB. But when you do it yourself, your constitutive activation of the signalling pathway accidentally leads to extra RB phosphorylation. Thus, instead of causing you to divide, this activates another protein called p53, which triggers a self-destruct sequence, and you die. This can be thought of as a safety valve, where any cell that tries to rapidly divide will automatically kill itself. So you’re going to need to figure out how to signal to yourself that you need to do some extra cell division, but simultaneously you’ll need to make sure you also deactivate p53 or some part of the apoptosis signaling cascade.
Meanwhile, each time you divide the ends of your chromosomes (telomeres) get shorter. There’s a mechanism that says, “once the telomere gets too short we can’t divide anymore.” This is like a hard-coded limit to the number of times you can divide. So you have to either activate a special protein that extends the telomere (telomerase) constitutively, or block the checkpoint that stops you from dividing if you don’t have telomeres. (more aggressive cancers often choose the second option to blow through this checkpoint, which causes lots of DNA mutations/chromosome instability)
The problem with all this is that it requires you to make a bunch of genetic modifications, which result in slight changes to the ‘look’ of the proteins involved. But there are cells that monitor for changes exactly like these ones. The way they do this is similar to sifting through cellular garbage. All cells turn over their proteins constantly, kind of like sending it all to a shredder and then spitting it outside of the cell. Before they take out the shredded trash, though, cells will load some of this shredded protein onto a molecule called MHC, which sticks to the cell’s surface for all the world to see. So the surface of every cell ends up with this MHC blanket that acts as a catalogue of everything that’s being made on the inside. Immune system cells called T-cells go around looking for anything that they’ve never seen before (like, say viral proteins that try to hide out inside cells and create more virus; or slightly altered versions of telomerase or p53 that don’t work like they normally should) and if they find anything new they kill the cell. There are trillions of cells out there; anybody can be replaced – and will be if it means protecting against cancer.
So some cancer cells (and viruses) figure they can just down-regulate MHC – that way their dirty secrets (that they’re producing new proteins, or variants on the ones that are supposed to work) don’t get out. But it turns out this doesn’t work either, because there’s another cell called the Natural Killer cell that goes around looking specifically for cells that don’t have any MHC on their surface. NK cells kill any cell without MHC.
Finally (but not really) if you’ve figured out all of the above but you don’t know how to instruct the body to grow new blood vessels into the heart of your tumor, you can’t grow much larger than a millimeter or two, because you can’t grow if you don’t have anything to eat.
So if you wanted to become a cancerous cell you have a lot of hurdles to overcome. The biggest problem you face is that:
1. Your mechanism for overcoming problems is by genetic instability producing altered versions of proteins and other elements that are there specifically to keep you in check;
2. Many of the mechanisms you need to tap into in order to generate these changes require you to multiply/divide;
3. The more you multiply/divide, the more pressure those natural anti-cancer mechanisms will put on you to either stop dividing altogether, or kill yourself.
TL;DR: Multiple mechanisms prevent tumorigenesis. They do this from multiple different angles. The organizing principle is not one of command and control so much as one of a naturally resilient architecture.
Interesting but beyond my knowledge level. I was looking for something more basic and analogous to other known social groups from microbes to humans. For example competition, resources, predation, cooperation. There is only a finite number of possible organizations.Would it be surprising if all organism societies exhibit some similarity. We can ask what seems to be the simplest and most common among studied groups. The answer is not likely the democratic and altruistic. Is that a possible reason for looking in that direction? I raise that question b/c it strikes me that this particular forum seems to accept altruism as more or less a given. Is this grounds for banning?
It defies basic logic that some “rogue cell” would be able to put together the most sophisticated molecular warfare systems seen anywhere in nature–capable of fighting off the worst that the most powerful chemical compounds we have and our immune system can throw at it simultaneously. It also defies basic logic that a cancer would prevail against the above, only to die with its host.
It makes far more sense that (at least aggressive or common) cancer is a pathogenic disease system that has a means of preservation outside the host and potential for infection of another after its first host dies OR that it is caused by a pathogen that does a good job of hanging out outside of the human body.
Tumor viruses were instrumental in the discovery of oncogenes. By the 1980’s, it was believed that viruses were the only possible etiology for cancers. Since then, we’ve discovered that few cancers are actually caused by viruses. Those that are are often much easier to treat/prevent (i.e. HPV).
I’m not an epidemiologist, but I recall reading somewhere that cancer rates in the developing world are much lower than in developed economies. That suggests there are things we’re doing that actively promote cancer.
Take smoking, for example. The primary drivers of cancer are:
1. Increased cell turnover/division
2. Increased genetic instability/mutation
So it makes sense that behaviors that encourage these two activities are associated with cancer in the tissues they affect. Tobacco smoke promotes DNA mutation. In addition, breathing in the products of combustion kills cells. So smoking causes lung cancer.
Meanwhile, if you chew tobacco instead of smoking that causes DNA damage, but is less cancerous because you’re not burning a bunch of stuff and then breathing it in (thereby causing cell death and encouraging division). However, if you chew and drink alcohol – like most people who chew – you’ll encourage cell death up and down your throat and encourage esophageal cancer.
OK, attribution to the presence of some one cause is the conventional way of analysis. But consider absence of some general characteristic which inhibits growth of cancers. As an example by analogy consider overgrazing on the village commons in the absence of a strong enough attitude against free riders by the many. Maybe many or most would overgraze then? Are tumors made up animal cells? I seem to have been too subtle in my original post about the possibilities of organizing principles that would be considered red in tooth and claw.Why that should be, if it it fact is, is what interests me. The good people of this forum surely have an opinion.
Again… we know smoking causes lung cancer, that’s right. That doesn’t change the fact that lung cancer is one of the most sophisticated, purpose-built killing machines on the planet. Random DNA damage caused by a poison isn’t really consistent with the above. There has to be more to it than that.
Just because we know a cause, or very strong risk factor, for a specific cancer doesn’t mean that (a) it’s the sole cause (tuberculosis was one of the great reapers of humanity for thousands of years, but it’s impotent in places without significant malnutrition) or (b) it has no way (in theory) of infecting other hosts at a later date. Simple reason suggests that an end-stage lung cancer patient who is constantly hacking is spreading potentially transmissible material throughout his or her environment.
That material may or may not turn into lung cancer in someone else. Maybe it will become another kind of cancer. Maybe some people are silent carriers. I am just throwing it out there because nature would not waste such a finely-tuned predator as cancer, and it’s highly unlikely something so advanced would arise as a random error.
Here’s a good way to understand this subject: consider that your blood (and interstitial space) is actually an incredibly valuable resource. You’re walking around with a pre-historic miniature ocean (1% salinity, similar to pre-historic oceans) that’s packed with nutrients in a nice warm, perfectly controlled environment. There’s constant perfusion with new nutrients, and virtually no competition for resources. Your blood, in other words, is microorganism heaven.
Except for your immune system and the physical barriers keeping out everything that would love to get inside and live there. So one of your questions is, “why does cancer work so well?” The short answer is that every cell in your body has the potential to defect and take on a role similar to that of any pathogen, except it can bypass all the physical barriers, and many of the immunological defenses that normally keep pathogens out. This is part of why there are so many controls against cancer built into the system.
In order to prevent cancer, somatic cells are organized to reduce their adaptability as much as possible. If you’re a single-celled organism and you encounter difficult conditions, it’s a good idea to introduce genetic instability in order to increase the mutation rate so you can figure out a new way to survive in your changing environment (cf. heat-shock proteins). In the human body, that’s not a strategy for inter-generational success, since coordinated systems are more important to maintaining the “personal ocean” effect than dramatic, unpredictable changes. Cancer essentially introduces a foreign agent with high genetic instability into an environment where that’s likely to be hugely successful short-term – until the organism dies. The cancer cells have to constantly fight against one specific immune system, but that doesn’t mean they’re well-suited for a different person’s immune system. Your body may have a difficult time distinguishing between kidney cells and kidney cancer cells, but your sister’s body has no problem telling the difference between her cells and yours. Remember that even for a close genetic match, an organ donation recipient will still have to take some serious immunosupressant drugs for the rest of their life or face immediate rejection.
Cancer develops in a semi-ideal environment where the only thing it has to contend with is a single immune system. It’s working with the enemy’s blueprints inside its own cells. Transplant it to a different type of battlefield and it will be wholly unprepared to expand and grow.
Also, remember that one of cancer’s greatest strengths inside your body is that it has lots of cells that often work together in unpredictable ways. Since the cells are all acquiring mutations constantly (in an aggressive cancer) one part of a tumor may be producing angiogenic factors (growing blood vessels) while another is deterring the immune system through cytokine manipulation.
Then, of course, there can be competition between tumors. This is, after all, a really nice beach vacation scenario for these different cancer cells, so they’ll naturally want to stake out their territory to funnel resources to themselves. So, for example, one tumor might release anti-angiogenic factors distally, to prevent growth of other tumors nearby. This leads, for example, to a phenomenon where a surgeon might remove a primary tumor and suddenly a bunch of secondary tumors spring up. The reason for those secondary tumors is that once the primary tumor – which was suppressing growth of nearby local tumor growth – is removed this releases those otherwise-invisible tumors to grow.
So imagine a couple of sneezed cancer cells floating through the air that you subsequently inhale. They don’t have the natural advantage of numbers, they’re working with a different immune system, a different genetic blueprint, and they have to figure out how to get “inside” past the barriers that other microorganisms have to deal with.
Meanwhile, those cancer cells aren’t optimized for long-term inter-generational propagation. They look successful, but unlike most successful organisms they kill their host before they can spread to a new organism. They rapidly outgrow their resources. And they don’t have millions of years of evolutionary experience at perpetuation of their novel strategies. Indeed, the only evolutionary information that is passed on from organisms that develop cancer is how to protect against it in the future. In short, they flame out and are as unsuccessful as we would expect from something with a bad long-term survival strategy.
If prevention is the most fruitful strategy right now: has anyone looked into the research on extended fasting for purging pre-cancerous cells via increased autophagy? I remember hearing Peter Attia talking about this, don’t know if it stacks up but sounded vaguely promising.
Did a bit of reading to answer my own question: autophagy is crucial for maintaining cell function and defense against pathogens. Deregulation of autophagy is linked to susceptibility to degenerative diseases, metabolic syndrome, aging, infectious diseases and cancer (once you already have cancer, it gets a bit more complicated: the cancer can use autophagy to survive/escape, so inhibition comes into play as a treatment option too).
Prolonged fasting dramatically increases autophagy. Studies show a 300% increase after 24 hours, then the growth rate levels off, but remains elevated. So it seems possible that doing regular prolonged fasts could be a useful preventative measure.
It’s also worth noting that in premodern times this would presumably have happened regularly; now we go our entire lives without ever leaving the fed state: it takes 24-48 hours of fasting to fully deplete glycogen reserves and switch over to ketosis (I’m not making an appeal to nature, but it suggests we’re at least perfectly capable of going long periods of time without food).
I’m probably nitpicky, but I’d say that changing social attitudes to smoking have radically changed both social policies and smoking rates.
My quest here is to murder the mental model of society as a machine where politicians decide on priorities that are then communicated to the masses who change their thinking accordingly and adapt to the decided upon priorities , thus improving society according to plan.
It’s possible I overreacted.
These stats from 2006-2012 are already way out of date for melanoma, and although it is a rare disease that doesn’t make much of a dent in overall cancer mortality like lung, breast, prostate and colon cancer, it is worth mentioning because the progress has been dramatic:
The phase III randomized trial showing the first effective treatment for stage IV melanoma had a control arm that had a 10% survival at 3 years in 2010. In 2018, the latest phase III trial with comparable patients had a 3 year survival of 58%.
Melanoma is an outlier in this list, but in some places we are making real progress.
> In the late 1980s, guideline-making bodies suggested that doctors test harder for prostate cancers; doctors followed the recommendation, detected every little tiny irrelevant prostate tumor, and treated patients aggressively for cancers that never would have affected them before they died of something else. In the late 1990s, guideline-making bodies admitted this had been a bad idea, made the opposite recommendation, and people stopped diagnosing prostate cancer as often.
More information on this
PSA testing became available in the 1980s. It is a blood test that is correlated with Prostate Cancer (PCa). It it a noisy indicator partly because it is also correlated with infection and with benign prostate enlargement (hyperplasia).
If PSA is high, you can have a biopsy and/or MRI scan to see if you have cancer.
In the early days, every cancer was treated aggressively. This resulted in a fall in death rates over time. But it also caused a lot of morbidity e.g. impotence and incontinence. The operation itself has a death rate of up to 0.5-1.0% so it can be a cause of mortality in itself. The biopsies can cause fatal infections, if done trans-rectally, and will impact sexual potency if done transperineally because of nerve damage.
Operative mortality may be one factor in the spike in deaths discussed in the posting. Also, previously many people with PCa did not know it and people would have died of it without specifically knowing where the cancer came from. Death results from metastasis into the bones, liver, brain etc. So better diagnosis can increase the apparent death rate from PCa.
Over time, it was realized that the aggressive treatment was not needed for all cancers e.g. localized cancers with low grade cancer rating (Gleason score of 4 mm diameter) that are dangerous.
Overall, I think PSA testing has resulted in a roughly 50% fall in PCa deaths, as suggested by the graph.
> (Gleason score of 4 mm diameter)
Typo should read
(Gleason score of 6 or less and less than or equal to 4 mm diameter)
RCTs of PSA testing have shown little to no benefit (and possibly harm) to PSA screening, so I doubt that it explains the drop in deaths, whereas therapies for prostate cancer have shown benefit in RCTs.
Improved 5-year survival rates for many abdominal cancers (such as ovarian cancer) are highly indicative of improved treatments being the cause, and not of improved detection. This is because of how cancer detection works. There are three main ways we often figure out someone has cancer:
1. We’re doing some expensive imaging (MRI, CT, etc.) for some other purpose and we happen to find cancer at the same time. This doesn’t happen a lot, since expensive imaging for some OTHER comorbidity is rare.
2. We have some kind of test (like PSA, pap smear, mammogram, colonoscopy) that we can use to look for signs of cancer.
3. The patient presents at the hospital complaining of symptoms that were caused by the cancer. Mostly, this involves the cancer cells growing somewhere they don’t belong. If you have lung cancer, that might mean you’re having difficulty breathing. If it’s ovarian cancer, you’re not going to notice a reduced function of the ovaries in a way that will likely cause you to head off to your doctor to get a CT scan. The reason is that the human abdomen is particularly well-suited to expansion. Organs shift out of the way to accomodate growth. This is good if you get pregnant and all that stuff has to move around to make way for an expanding uterus. If, instead, you have a growing ovarian cancer your organs shift out of the way and you don’t realize you have cancer.
The reason this is bad is because, as Scott mentioned, there are (roughly) four stages of cancer development, and if we catch your cancer at an earlier stage it’s easier to treat. For example, with stage 1, your cancer is local and usually we can just go in and cut it out and that’s the end of it. Stage 2 means it’s starting to spread into the surrounding tissue; we’ll try cutting it out, but we’ll also often give you some chemo to catch anything we might have missed. Stage 3 means it’s starting to spread out of the organ it started in, so there’s a larger risk that even with chemo we’ll still miss some cancer cells and they’ll come back worse. Stage 4 is … really bad; there’s a high risk that chemo won’t even begin to get everything, and no matter what we do something will be unaffected and will get out of control – fast.
So say you go to your doctor; “I’ve been having trouble breathing lately. Not sure why, but I’m always winded.” They do a CT scan and give you the bad news:
1. You have lung cancer. Not to worry, it’s stage 2, we’ll treat you and in our experience there’s a good prognosis for this type of cancer.
2. You have ovarian cancer. It’s spread throughout your abdomen and into your lungs now. There are too many lesions to go in and cut them all out. We’re going to hit you hard with chemo and hope for the best. Prognosis for this type of cancer is a matter of weeks or months. You have no chance to escape, make your time.
When I learned about improved 5-year survival rates for ovarian cancer was when I first started to suspect that improved treatment is a major contributor to improved cancer survival rates. Working directly in clinical oncology research has significantly shifted my views toward the “pro” side of the question, “Does cancer research improve outcomes?” Many sub-types of cancer that used to have very low survival rates have shifted substantially to much higher survival rates. The overall landscape is complex, since cancer is often characterized as a family of diseases, and it often looks like we’re getting nowhere. But trust me when I say that you’d rather have cancer today than in the 90’s, given the treatment options we have today versus back then.
Couldn’t there also be bias because non-cancer deaths are down? So the 5 year survival rate includes some people who died in (for example) automobile accidents completely unrelated to the cancer diagnosis. If traffic fatalities are down, that would show up as a increase in the 5 year survival rate even if the treatment is completely unchanged.
I thought they usually corrected for that.
It’s a bit of a misunderstanding of how we treat advanced cancers to think that improvements in 5-year survival rates must also necessarily be correlated with decreased death rates. Basically, if your cancer is sufficiently advanced we’re going to try an initial “curative” treatment, where we will cut out the main tumor (where possible) and then follow-up with chemotherpy or radiation treatment to try and get all the other lesions, and any cancer that’s too small to show up on a CT scan. If we’re successful, and your cancer completely disappears, there’s a good chance your 5-year survival rate will correlate well with you not dying of that cancer. That includes many of the easier cases that we’ve been building good treatment regimens for over the past few decades.
On the other hand, if your cancer doesn’t respond to that first round of chemo (more common with advanced stage cancers), there’s a good chance that you’ll have to undergo multiple other rounds of chemo, additional attempts at therapy, perhaps some clinical research trials. Some of these strategies will likely fail and we’ll quickly switch you to a different treatment approach. Some may succeed and give you anywhere from an additional 6 months to 3 years (or more!) of progression-free survival. Eventually, honestly, most advanced patients eventually progress and the cancer wins in the end. But to say this doesn’t matter if the patient eventially dies of cancer ignores the many additional years of life those patients get – often without any symptoms of their dormant cancer. In the fight to improve cancer therapy, absolute cures are not the only metric we care about. To a 47 year old mother of 3 who gets an additional 10 years to watch her children graduate college and get married, it really matters that improved treatments gave her more time, even if she died of cancer in the end.
How often does this happen if there actually are such other lesions? I thought that (detectably) metastatic cancers were almost always incurable at present for most types of cancer.
This really depends on the type of cancer, how aggressive it is, the extent of metastasis, and where the mets are located. Lot’s of cancer treatment efficacy questions really boil down to “it depends”.
As to the statistics, “Of patients with metastases who receive initial adjuvant chemotherapy, what is the 10-year survival rate?” I don’t have those numbers. But again, there’s reason to believe that it would be different for, say, NSCLC versus glioblastoma; such that lumping them all together in the same statistic doesn’t necessarily tell you as much as you want to know. It isn’t true that metastases are always a death sentence, though.
We can cure a reasonably high percentage of metastatic colon cancer, for example.
Wars tend to be educational. One thing the “War on Cancer” has educated us in is that cancer is not one disease.
In old books, people die of “fever.” Then we started trying to cure fever, and realized that staph infections are different than strep infection, and both are different from viruses, and inflamed lungs are very different from inflamed meninges. But at one point, they were all classified as “fever”.
Similarly for cancer: some are viral, and virus treatments greatly reduces their incidence (HPV-related cancers). Some respond to particular therapies (for example, childhood leukemia was a death sentence 50 years ago, is ~90% survivable now.) But there’s not a general solution, because it’s not one disease–it’s many.
*Not a medical professional, but the one college friend I still talk to regularly is an oncologist.
When I read history, I always notice all the “fevers.” They did attempt to discern the causes, but unfortunately didn’t end up along the lines of virus/bacteria. At some point Alexander Graham Bell wrote he had “a fever from too much photo-phone.” That was a precursor to the telephone. Fevers were usually blamed on some sort of stress, which is just sad. The people were probably stressed because they were suffering from malaria or something and were generally disoriented, and then they were told it was their fault.
The more I learn about rising human lifespans the less credit I give medical science. It seems like every time you zoom in on an improvement in some health metric it ends up being about improvements in lifestyle and environment rather than some technological innovation.
“every time you zoom in on an improvement in some health metric it ends up being about improvements in lifestyle and environment”
That’s because “deaths due to starvation” is treated by lifestyle and environment changes, along with “death by smallpox” “death by infection” and “death by transportation accident”.
Farming, vaccines, antibiotics, anti-derailment devices, anger management, air quality, and fire exits are now “lifestyle and environment”, not “medical innovation”.
Antibiotics and vaccination likely deserve a great deal of credit. Antiseptics, too. I suspect advances in childbirth-related medical technology would be important too. It’s hard for an individual disease treatment to move the needle much. Heart disease and cancer are the most common causes of death, but neither is really a single disease.
Add clean water to the list.
I’m a little surprised that increased early detection is played down in this post as a measure of progress. Digging into how well we can do battle with a tumor of a certain strength once we know it’s there is certainly a useful thing to know, but I think the real message here is that we should be singing praises for those who have pushed forward the field of cancer detection. Based on your post it cetainly seems to have had the greatest effect on overall mortality, which IMO is the most important metric.
The point isn’t that cancer detection improves prognosis, it’s that it improves an artificial measure of prognosis based on how long between the detection of the cancer and the time it kills you.
(it does also improve prognosis, that’s just not what this post was about)
Ah, that makes sense now. Thanks for clearing it up.
A common intuition here is that most early detection testing isn’t worth doing because the tests would need to be ludicrously accurate to do more good than harm and actual real-world tests frequently fail to meet that mark.
For instance, suppose you have a population in which some rare form of cancer affects about one in a thousand people and you have a test for that cancer which is 99% accurate by which I mean only one time in a hundred does it produce a false positive. (we’re ignoring the false negative rate for now – let’s say it’s zero.)
In that circumstance, out of a thousand people tested you’d find one person who actually has the cancer but you’d also get ten false positives, meaning if someone tests positive there’s still a ~90% chance they don’t have that cancer.
You could try rerunning the test but even that might not improve the odds as factors specific to that person which caused the initial false positive could cause a followup false positive.
Thus as early-detection options proliferate, this fact is likely to make us ever more prone to treat people for cancer who don’t have cancer. Then when those people who we have subjected to needless costs and medical procedures continue to not have cancer and thus fail to die from it, we inaccurately congratulate ourselves on having nipped it in the bud. A higher misdiagnosis rate caused by the introduction of a new test automatically makes the numbers look better – the measured survival rate for that cancer is higher – even though 90% of the actual patients are worse off for the existence of that new test.
In short: Base rates matter.
It also matters whether treatment helps and whether treatment is necessary and appropriate – even when the test is accurate and somebody DOES have cancer it’s not clear early detection is a win.
Relevant youtube link: Adam Ruins Everything – mammograms
Yeah, actually, cancer biology is my field (PhD student in a Tumor Bio program). I was chatting with a fellow trainee at our department retreat last week and we were talking about what we might expect for cancer and “curing cancer”, say, 50 years from now. We were both inclined to think that prevention and early detection has some relatively low hanging fruit. Specifically, it seems like we’ll develop the capacity to have a much better idea who’s at risk for what cancer. Pancreatic cancer is basically a death sentence, because it’s almost never caught early enough. If you catch pancreatic cancer early I’m pretty sure you can take the pancreas out and have a pretty good prognosis. But it’s really not feasible to just screen everyone for pancreatic cancer, because of the false positives, and by the time most people have detectable symptoms it’s pretty much too late. But if you had a very good idea that okay, this small subset of people have really elevated odds of developing pancreatic cancer, you can screen just the high-risk group and come out with good results. Obviously some of that exists currently, pretty sure mammogram recommendations define different risk groups, but it’s pretty coarse for the most part. Sequencing is getting cheaper and cheaper, and data analysis is starting to make some gains on getting useful information out of the type of datasets we can currently generate – that’s where the gains in this area will come from, if they do in fact materialize.
Researchers are working to add algorithms for detecting pancreatic cancer into medical imaging systems so that hopefully pancreatic cancer will be able to be detected incidentally when someone gets a scan for eg. back pain.
Hey, if you can come up with a great system for spotting pancreatic cancer in scans, that would do the trick. But you’d need the specificity to be very very high to get valuable results out of applying it incidentally in a population where pancreatic cancer is very rare (like in random people getting scanned for back pain).
I see this occasionally (cardiac nurse). We’ll send someone down for a cat scan of X. Incidentally, it will pick up oddities elsewhere, a nodule on the lungs for example, with the suggestion to have it looked into later.
The idea behind lead time bias is that, when you say that median survival with this new improved screening method goes from 1 year to 2 years, it sounds like you are giving those people on average a whole extra year of life. But in reality what is often really going on is that instead of telling the patient, on 8/2/18, “you have a year to live,” you are just travelling back in time to 8/2/17 and telling them “you have 2 years to live.”
The reason this is counterintuitive to most people, and I think the main reason people get so frustrated with the lack of progress despite fancy treatments and surgeries and scans, is because most people dont really understand or internalize the dictum of cancer doctors: biology is king. To oversimplify a bit, there are cancers you are gonna cure, and cancers you arent, and what you do in terms of surgery, chemo, rads, whatever is far less important than tumor biology.
For well behaved cancers, you have a wide window in which to detect and treat, so late detection isnt so bad. For poorly behaved cancers, you have a narrow or nonexistent window, and so early detection doesnt matter. Most of the progress is, of course, made on the margins
How much of the increased survival within stages is due to better staging because of increased detection technology? If a cancer would have been formerly labeled as stage 2, but better technology let’s you see metastases all over allowing the correct label of stage 4, this would lower the mortality of both bins(presuming the metastases you can see only in 1975 are worse).
Quick note about me: I work in life sciences, and have worked in precision cancer medicine in the past.
One thing to keep in mind is that cancer is a family of diseases. Progress in one area may or may not translate into others. Scott has made this clear; when I first read the headline my reaction was “we’ve significantly reduced mortality rates in colon cancer (and maybe a few others) but not in the big ones I hope Scott points this out” and I was pleased :-).
We have also made a lot of progress in treating childhood cancer, good discussion at from cancer.gov. (That page uses 5-year survival rates, and raw mortality rates would be better, but I expect the bias discussed above doesn’t apply as strongly to youth since we don’t screen them, and also treatment has improved a lot for 0-4 year olds and we don’t test before birth so 5-year survival should be an unbiased metric. Raw death rates here, there’s been a 25% decrease since 1990. That’s going to be a mixture of barely any progress in some cancer types, combined with a lot of progress in others, just like adults).
Regarding lung cancer, cancer immunotherapy has been all the rage recently, and it’s most applicable to lung cancer. Checkpoint inhibitors have been massively successful in treating previously-untreatable cancers. This has meant increasing the 5-year-survival from 0-5% to 20-30%, in terms of raw cancer deaths anti-smoking efforts are much more effective (EAs take note). Still, for somebody who gets lung cancer, 30% chance of survival is much better than 5%. And if that success can be repeated the survival rate could get much higher.
I expect that trend to continue. “Breakthrough” treatments are at best going to increase survival rates by 10% in a limited set of cancers. Note also that this is fucking huge, and it only started happening in the last decade. This is way more progress than in the 90s or 00s. So progress is accelerating (unless it was a fluke). Still, it’s going to take a few dozen breakthroughs of this nature to bring survival rates up to something a lot less scary (say >90% for >90% of cancers).
@ Jacob Silterra or anyone else
A few questions:
(1) I’m curious, what significant improvements (if any) have been made in the last several years regarding early detection of lung cancer?
(2) I recall a study whose outcome suggested that low-dose CT scans were useful for a subset of the population that smoke heavily. However, this doesn’t seem like a great way to detect lung cancer early given that the radiation is still an issue, and access to (and the cost of) such scans can be a problem. Also, lung cancer arises in people who have never smoked, so this doesn’t seem to pertain to them.
(3) I read about breath analysis in press releases, but so far as I know, no such technology is available for patients yet. Is that true?
(1) People are working on it obviously but nothing has made it to the clinic (that I’m aware of). I didn’t mention this earlier btw, but lung cancer is typically detected at stage 4. People have almost no symptoms until they’re close to death. It’s a big problem. Early detection would help tremendously.
(2) Yeah I’d be suspicious of this approach, also the logistics are tricky. Currently there are 20 million CT scans done in the US per year, compared to ~40 million smokers. We would need to triple capacity, for a screening test which might not work and could be counterproductive.
(3) I’ve never heard of breath analysis before, this review has some nice info. Looks promising but there’s nothing in the clinic. Apparently dogs can be trained to detect cancer, I wonder if the fact that cancer-sniffing dogs don’t exist yet is a market failure.
Jacob and others–I don’t know if you guys are still actively participating in this thread, but I suspect that the lack of significant symptoms of lung cancer before it is too late is “a feature not a bug”. It probably is a feature of natural selection for the survival of our species, shaped in an era where very large numbers of humans routinely got lung cancer from some environmental cause (frequent wildfires? An upper respiratory pathogen that did a lot of DNA damage? Some zoonotic from game animals when most of us were H-Gs?).
In other words–people who survived for a long time with lung cancer with no appreciable disability were more able to provide for and protect their children until an age that they could fend for themselves than those who quickly became crippled and useless after developing it. Look at the hated “obesity genes” that plague the First World and developed Third World today with diabetes, heart disease, etc.–historically, humans were more likely to die of complications of starvation than of obesity at a ratio of about 99:1, so of course calorie-“conserving” genes would win out over our species. We are adapted to surviving without enough to eat, not with.
I’m a medical oncologist and cancer researcher.
Screening CT scans have been proven to be effective in preventing deaths from lung cancer in long term, heavy smokers in a randomized trial. It is recommended in people aged 55-80 with a history of smoking at least a pack a day for 30 years. Cost and capacity to screen everyone who is eligible is an issue, but the level of radiation involved is several orders of magnitude below being significant. Nothing yet for lower risk folks such as nonsmokers, but we are working on trying to develop tests with better specificity.
https://www.nejm.org/doi/full/10.1056/nejmoa1102873
Can’t speak to the breath thing, but I’m highly skeptical.
Thanks for the replies, Jacob and JR616 (and for the link).
I’m surprised by the rate of progress on this problem. Given that late diagnosis is so common, and that it leads to such a poor outcome, you’d think that there would be something better available for detecting lung cancer at an earlier stage.
I understand that lung cancer doesn’t attract the most sympathy from would-be donors. That’s a big reason I dislike smokers, as I imagine they stymie research in this area and, arguably, contribute to the deaths of those non-smokers suffering from this disease.
My father has lung cancer and, anecdotally, they added the ability to do a blood test to check his plasma for cancer cells and monitor mutations. The lab got this capability about 4 weeks ago.
I am not an expert, it might be too expensive or too low power to make sweeping changes to early detection. Cursory google searches yield hopeful articles.
https://www.medicalnewstoday.com/articles/320679.php
It was miserable getting my dad’s diagnosis after it spread throughout his body. If this blood test saves people from that experience then this it is a miracle.
@ Flavoryeagle
Sorry to hear about your dad, that’s awful. I’m guessing you’ve looked into options, but in case you haven’t heard of them, a couple things worth mentioning (particularly if your dad suffers from non-small-cell lung cancer (NSCLC)):
Perhaps have your dad obtain a genetic-marker test to detect EGFR, ROS1, or ALK mutations. If the EGFR mutation exists, then there is targeted medicine available called erlotinib (marketed under the name Tarceva). For ROS1/ALK there is a medicine called crizotinib that you may need to specially request for access.
Out of date, but there is (was?) a medicine called Nivolumab made by Bristol-Meyers Squibb, and other PD-1 or anti-PD-1 therapies, being touted as promising for NSCLC. Although I see at least one commenter suggests these have not been as effective as hoped; nevertheless, perhaps ask your dad’s doctor about access (hopefully, these are out of clinical trials now) and possible benefits.
My sympathies.
What’s up with the c1940 use of the phrase “war on cancer”?
It disappears if you put the phrase in quotes. There was war, and some texts about it also contained “on” and “cancer” somewhere else.
That’s not how google ngrams works. It’s already searching for the phrase. If you put it in quotes, it searches for people who used quotes themselves, talking about Nixon. If you don’t use quotes and then the google books links at the bottom of the page to search google books have quotes added, like this. Some of those hits have the wrong date, but most of them are real.
One of the major things I observed at MetaMed was that the cancer death rates from rare cancers have improved much more than those from common cancers. Also, the outcomes from common cancers seem to have improved a great deal at the best clinics. One natural interpretation is that progress in beat in class cancer treatment has been rapid but for social reasons, only a few people get to be the top recognized experts in a given cancer and social pressure has prevented people who aren’t the top experts in a cancer from adopting innovations. Since only a few doctors can be the top experts in a given cancer, almost no patients benefit from the improvements in treatment of common cancers.
The rare cancers which have been treated may just be by nature more easily treatable than common cancers, however. If a cancer is common, it’s likely that it’s fairly easy for it to be caused and perhaps it has many different possible causes, which may imply fairly difficult for to be prevented or treated.
The big exception (as usual) is smoking-caused lung cancer.
Is it also plausible that common cancers are more competent? Perhaps rare cancers are the ones that people are better at fighting off and/or preventing.
Might alcohol consumption also be a significant factor in the rapid decrease of stomach cancer?
I doubt it, since there hasn’t been much decrease in alcohol consumption. The first thing to check is to control for sex, since female consumption is way up since Prohibition.
Might the quality of alcohol have been worse when it was unregulated and illegal?
Sure, but that was only a decade. And if that made a big effect, why don’t we see a trend upwards some time after that decade?
My bet would be swapping chewing tobacco for smoking.
Smoking contributes to stomach cancer, which makes sense with Korea being #1, but doesn’t make sense with the secular trend in America. So that’s an interesting hypothesis. Again, control for sex. But it’s such a huge change. It’s about 1/6 as common as it was in 1930. If it were as simple as chewing tobacco, ie, a single cause by something not that common, that would leave a pretty clear signal in the 1930 data (though not necessarily the data today, when chew is rare). I wouldn’t be terribly surprised if someone told me that no one had ever looked and it turned out that this is the answer, but until someone claims that I’m assuming that they did look and it’s not that easy to explain. Again, Korea. They don’t chew much, do they? (If they do, then it should be easy to see the effect in the data today.) Pickles make a lot more sense. They’re spread through society without individuals identifying as picklers or abstinent, but there are big changes in quantity through time and space.
Sweden has this awful chewing tobacco that is quite popular there (13 % of the population use it regularly). In fact, chewing tobacco is so popular in Sweden, that they included an exception to EU laws on oral tobacco during the accession. Sweden is basically quite similar in genetics, lifestyle and income to other Nordic countries. Does Sweden have unusually higher incidence of chewing tobacco?
Is it really more popular than in other nordic countries? I guess if Sweden has an exception that Denmark doesn’t, that’s pretty suggestive.
Anyhow, Sweden has lower stomach cancer rates than Denmark and Finland, which are lower than the rest of Europe.
It is only legal in Sweden. It is illegal in every other EU country (and Swedish businesses cannot sell it to other EU countries).
Snus and the government monopoly on alcohol sales were the exceptions Sweden got when they entered the EU. Sure, there will be some people in Copenhaghen who drive across the bridge and buy it, but it being illegal there makes its use much smaller. Snus is also illegal in Finland.
Sweden has the smallest smoking rate in Europe, because they consume snus (the cold and the high prices also help).
Then we can assume that chewing tobacco probably does not affect stomach cancer rates. I think that Sweden and Denmark are as close as you can come to populations similar in every way, except for the oral tobacco. If they don’t differ, then oral tobacco probably does not affect much.
There’s some literature that I read but am too lazy to look up that links a significant decrease in stomach cancer (and some decrease in colon cancer) to availability of refrigeration.
I.e., if you don’t have refrigeration available, then people consume much more preserved foods – pickled, cured, smoked, fermented, etc, etc; and most such traditional preservation methods are somewhat carcinogenic. Once refrigeration gets widely used, all those traditional preserved dishes get consumed in much smaller amounts and after a certain delay the cancer incidences drops as well; and this decrease has happened in many cultures at different decades depending on when “mass refrigeration” happened there.
Wait, just how carcinogenic are pickled and cured foods?
Somewhat? It’s a *slight* effect, much smaller than smoking, and cumulative – it manifests a lot when it’s a staple food that everyone would be eating every day throughout the winter, and not nearly as much when it’s a snack every now and then. Also, carcinogenous compounds get created simply by frying bacon and the like.
It also highly depends on the processing method; much more of curing used to involve nitrites and thus was much more carcinogenous than nowadays when this has been regulated more and less nitrites are used; the same applies for things like smoked fish that can be done in different ways, and the more carcinogenic traditions can be made illegal for sale – but this means that “how carcinogenous is dish X” depends on where you live and what practices are used to make that dish; often the faster/cheaper (and sometimes simply more tasty) process is much more carcinogenic than another way of making (almost) the same thing.
Sometimes it can be a substantial effect:
https://www.ncbi.nlm.nih.gov/pubmed/11992412
(If I’m reading this correctly, it seems close to the “staple food” case)
I recall seeing something once (man oh man does that sound reliable!) where the largest factor in the increase in smoking rates were the world wars and the US government giving free smokes (plus conditions ripe for wanting to smoke) to entire generations of US males. Of course this doesn’t explain increase in female smoking that happened and I am predisposed to believe it and I have no reference.
Anyone know of suck a study, or am I making it up?
The graph in the post marks US entry in to both wars. American cigarette consumption took off like a rocket at the beginning of both wars, which is really weird, since the country entered late. Consumption doubled during WWI, but leveled off on actual entry. Consumption kept increasing during WWII even after American entry, but not any faster than before.
Consumption doubled during both wars, but it also doubled during the roaring 20s. That could be the returning soldiers spreading it to the rest of the population. Consumption is steady after WWII. That surprises me. I’d expect demobilization to have a large effect of either sign.
Thanks, I was on my phone reading and couldn’t make it out.
I would like to see more about the military and smoking.
When I started smoking as a teenager I bought cigarettes in the PX in Germany for one dollar a carton. My father started smoking in the service during WW II. It was one pleasure the military encouraged since troops could not legally have sex or drink in a combat situation.
I recently saw a movie about D day and they had Ike virtually chain smoking.
Moreover, the active military is now a much smaller share of the population.
I have been told by friends of mine who smoke or used to smoke that there is nothing like a nicotine hit to level your heard and calm your jitters when you are in situations of high stress or fear of doom.
One good friend of mine, for whom kicking her nicotine addition was like tearing off her own arm, credits taking up smoking and then heavy smoking to saving her life and her sanity from a period in her life that was legit full of external imposed extreme stress and existential dread.
Given that, it makes sense why war time would cause an increase in smoking, especially by soldiers.
Don’t know of the study, but I was interested to learn that cigarettes were a part of military rations until 1975.
I can personally attest that in 2005 there were designated smoking areas on submarines. I didn’t see anything that would cause me to believe that has changed, I just can’t personally attest after that date.
In my experience submarines did away with smoking underway around 2010, though this may not have been a Navy-wide policy. Most of the smokers on board switched to chewing tobacco, and then to Snus and the like when the Pacific Garbage Patch-motivated plastic waste minimization policies meant they couldn’t dispose of spit bottles easily. There was a brief period where people switched to vaporizers and used them wherever, but the command just declared them to be equivalent to cigarettes once a trend was identified.
I find this interesting particularly because the idea of one soldier telling another one “y’know, smoking causes cancer” strikes me as so obviously funny that I swear there’s been a Bill Mauldin cartoon about it at some point.
That is: anything cancerous is fine for soldiers, given what else is likely to kill them earlier.
Which then leads to me wondering how much of lung cancer from smoking came from young men who decided they were likely to die in a war anyway… and then they stopped dying in wars.
Combat deaths in the US military really plummeted after Vietnam, didn’t they? Earlier than that for the Navy and Air Force…
It sounds like a very Bill Mauldin thing, but he didn’t do military cartoons after 1945, IIRC, and the link wasn’t firm until 1950 according to Scott’s graph.
That is: anything cancerous is fine for soldiers, given what else is likely to kill them earlier.
I don’t see it. First, most young men who went overseas had a good chance of coming home alive. An infantryman in WWII had really bad odds, but it’s easy to overestimate the number of infantry and underestimate the number of aircraft mechanics and supply clerks. Second, by the time the smoking-cancer connection had become common knowledge (probably late 50s/early 60s), even infantry had a pretty decent chance of making it home. I don’t have good statistics offhand on infantry casualty percentages in Vietnam, but only about 2% of those who served in uniform in Vietnam were killed.
@bean: And didn’t US Army and Marine Corps combat deaths drop orders of magnitude again after Vietnam?
> Official statistics say we are winning the War on Cancer. […] More skeptical people offer an alternate narrative.
When I read those first two paragraphs, I thought you were publishing one of the articles resulting from your adversarial collaboration contest. But nope.
Stupid question, why can’t we just look at the change in average age of death of people who have a particular cancer?
If for, say, lung cancer, we’re detecting it earlier but not treating it better, five-year survival will increase but average age at death from lung cancer will not. If treatment improves, the average age people are at the time they die of lung cancer would increase.
I’m not sure that works. Lung cancer only kills you if nothing else does so first. If lung cancer treatment remains the same, then the average age of lung cancer deaths should go up as other causes of mortality go down, allowing more people to live long enough to die of lung cancer. Not to mention that this is heavily confounded by changes in smoking patterns. If younger people are less likely to smoke, then the incidence of lung cancer among the young will go down, driving up average age.
Ah, that makes sense.
Thanks.
This probably won’t be a large effect with lung cancer specifically, since it tends to kill people quickly (though your point about age-related smoking still matters). It likely is a big confounding effect with prostate cancer since that affects mostly older people and takes a long time to do so.
I’m not sure that how quickly it kills you matters very much here. Let’s say that being a heavy smoker gives you a 5% chance of lung cancer every year after you turn 49, and it kills you exactly 1 year later. Let’s say that everyone dies of non-lung-cancer causes at 63. So a heavy smoker has a 50% chance of dying of lung cancer and a 50% chance of dying of something else. But medical advances suddenly raise the death threshold by 5 years. This raises the proportion of heavy smokers who die of lung cancer from 50% to 62.5%, and shifts the average age of death from lung cancer up some amount that I can’t be bothered to calculate.
(I am well aware that this is not a particularly good model, but it illustrates my point. Toy model, do not use for actual decision-making.)
Death rate of each cancer among people of each age group over time? I think that avoids the confounder of “only if something else doesn’t kill you first”.
5-year survival rates by age first diagnosed over time? Is that even a graph that the data is available for? What about “Age first diagnosed, of >5 year, 5-10 year, and 10+year survivors”? More aggressive diagnosis would show an increase in diagnosis and survival times with no change in death rate unless there was some benefit.
To avoid this effect, look at the percentage of people who get a given type of cancer at a given age, rather than the average age at which people get that cancer. But even then, earlier detection should move the time the cancer is detected earlier by just a few years, and it’s hard to separate from the noise coming from behavior changes etc.
Polio and smallpox vaccines are much cheaper than cancer treatments. They are also more likely to affect kids, and kids are a much more sympathetic recipient of free state treatments than the general cancer patient (who probably contributed to their disease, or can be accused of that). So even if we had cancer treatments as effective as the polio vaccines, but at the current prices of cancer treatments, we would not eradicate cancer, at least not worldwide.
Most of the low-hanging fruit is gone. Every disease we eradicate will be much more costly than the previous one.
>Every disease we eradicate will be much more costly than the previous one.
The last enemy that shall be defeated is death.
And if that happens there is the new horror of having to live forever.
The last enemy to be destroyed is submaximal global utility; defeating death just buys us more time.
What if global utility reached its maximum sometime prior to homo achieving self consciousness? What if global utility will always be submaximal as long as there is a human?
Then who would define utility?
That assumes death has no utility. I’m a devout murderist, personally.
Defeating death does not mean you have to live forever. It means you can live as long as you want to.
deathheat deathInteresting backward looking data. Any take on recent new developments (immunotherapy etc.)? Seems that at least for certain blood cancer types scientists are really starting to crack the code and pump out miracle drugs, and solid tumor cancers are expected (hoped?) to be next in line. Impact wouldn’t show in stats yet, but the direction of travel seems encouraging.
There’s been an avalanche of work (and money, the crystallized form of work) pouring into immuno-oncology based on the broad responses seen with PD1/PD-L1-targeted therapies, but the most recent news in IO is the back-to-back failures of both Merck and BMS’ IDO inhibitor trials. This was supposed to be the next big thing in checkpoint inhibitor therapy, but at the moment it looks like an utter bust. Plenty of other irons in the fire, but the picture isn’t near so rosy as it was even a few months back.
Oncology has historically moved in waves like this, with some thrilling new paradigm shimmering over the horizon, promising an ammo belt full of silver bullets – cytotoxic chemo! TKIs! anti-angiogenesis! – which instead offers some modest progress on a subset of cancers before making way for the next big thing. IO is an exciting field to be in, no lie, but the immune system is qualitatively more complex than cancer itself and successfully harnessing it to zap a tumor without triggering some catastrophic inflammatory response might be the work of a generation.
More immediately, I’d expect liver cancer numbers to start collapsing now that hep C’s been basically cured.
(filter seems to have eaten my comment, so posting again without links)
There’s been an avalanche of work (and money, the crystallized form of work) pouring into immuno-oncology based on the broad responses seen with PD1/PD-L1-targeted therapies, but the most recent news in IO is the back-to-back failures of both Merck and BMS’ IDO inhibitor trials. This was supposed to be the next big thing in checkpoint inhibitor therapy, but at the moment it looks like an utter bust. Plenty of other irons in the fire, but the picture isn’t near so rosy as it was even a few months back.
Oncology has historically moved in waves like this, with some thrilling new paradigm shimmering over the horizon, promising an ammo belt full of silver bullets – cytotoxic chemo! TKIs! anti-angiogenesis! – which instead offers some modest progress on a subset of cancers before making way for the next big thing. IO is an exciting field to be in, no lie, but the immune system is qualitatively more complex than cancer itself and successfully harnessing it to zap a tumor without triggering some catastrophic inflammatory response might be the work of a generation.
More immediately, I’d expect liver cancer numbers to start collapsing now that hep C’s been basically cured (sofosbuvir).
I can’t agree with this comment too much! I trained in immunology in the 2000’s and there was a lot of optimism about how it could be used to treat cancer. I was a true-believer – until the evidence came out and it became clear we weren’t getting far with immune system modulation. The problem really is that we don’t understand the immune system well enough, and anything we do to modulate it is likely to produce numerous unintended effects.
That doesn’t mean it’s all bad, since better understanding of T-cell receptor signaling has led to real gains, and in non-oncology fields (psoriasis, RA) immunology research has lead to some solid gains (e.g. IL-17 inhibitors). With cancer it’s always good to take advancements with a grain of salt, because reality has a nasty habit of catching your theory and pounding it against the mat.
Perhaps this https://www.fightaging.org/archives/2018/07/oisin-biotechnologies-produces-impressive-mouse-life-span-data-from-an-ongoing-study-of-senescent-cell-clearance/ is the next big thing? Unfortunately I have not had time to dig out papers on their “programable suicide gene” but IF it works as advertised and IF cancer cells can’t easily evolve around this mechanism this might work on basically every cancer because every cancer has some unique protein it expresses [citation needed]. Unfortunately these are also two very big ifs…
Call me old fashioned, but when I see someone suggest selectively killing all my cells that express p53 I think “No thanks, I don’t want to develop cancer”. p53 is the big daddy of tumor suppressor genes. I get that they’re going on the rationale that the expression of p53 is a marker of senescence. But it does not instinctively sit well with me, I’ll say that much.
It might work, but I’d bet against this specific thing being the next big thing simply because everyone is trying to sell their thing as the next big thing and almost certainly most won’t be. I wouldn’t get your hopes up too high about this specific approach. But there might be merit to it, we’ll see.
Agreed. File this with “things that are easy to do in a mouse model but will never be practical in humans”. I have slowly come to realize that non-biologists just don’t have the training to see the myriad complications suggested by obvious-sounding interventions that are ultimately not feasible.
That is my fear too.
1. I am a biologist 2. Biologists also can’t see the myriad complications suggested by obvious-sounding interventions that are ultimately not feasible. Especially if they haven’t even read the relevant papers. 🙂
I think the error is the tendency to think, once you understand a piece of a complex puzzle, that you therefore sufficiently understand the salient aspects of the whole of it.
It’s like learning about the interaction of tissue factor and factor VII in blood clotting, and you think, “now I know how blood clots”. And I think it takes time until you’ve had enough experiences where the complexity of the system shatters your previous supposed understanding.
You keep thinking, “now I know what’s going on here” when you learn the signaling pathway for NFkB; and then you learn that NFkB has multiple signaling pathways that it interacts with, but that’s not a problem because you can memorize the multiple pathways and understand which one is activated in the system you’re interested in. Then you learn that NFkB isn’t a single protein, but a complex of multiple proteins. Then you think, “okay, but now I understand it” and then you learn that there are multiple different possible combinations of subunits that can form the NFkB complex. Then you learn that each of those subunits has multiple splice variants. Then some group of researchers discovers siRNA, and you learn that suppressor mRNA modulate gene expression for the balance of splice variants of the different subunits that comprise NFkB and you look across the landscape of all the different molecules in the whole signalling pathway that all have a similar level of complexity and you say, “I’m going to try and understand this one piece a little better; but I can never pretend to understand the whole of it.”
I just don’t know how you teach that, or communicate the scale of it, other than through direct experience.
You want your cells to have the p53 gene, not to express it. It gets expressed if and only if something in that cell goes terribly wrong. If this cell then has and expresses p53 it may become senescent, otherwise it would become cancer (oversimplified). So selecting against p53 expressing cells does not promote cancer. Selecting against p53 having cells would (it would also kill you).
Yes, and this makes it a good target against senescent cells. For cancer treatment you would of course need a different target, since cancer cells typically do not express tumor suppressor genes.
That is a fully general counterargument, since it will also work against every single approach that actually does work. And if you had asked me 5 years ago what kind of system might actually solve cancer (and begin to solve ageing) in the future I would have described something very similar. In fact I have done so (as an ill fated attempt to convince my professor to let me do that as my Phd thesis in his lab) https://www.dropbox.com/s/o1lmh3vklf7uyop/Selecting%20among%20metazoan%20cell%20populations.pdf?dl=0.
Yeah, like I said, I do in fact understand the rationale. But if you come to me and say “I have a great idea for anti-aging tech, just throw in a genetic kill switch for all cells expressing these one or two genes only expressed in senescent cells” I’d be inclined to say “Interesting approach and maybe it has potential but I can think of several ways such a blunt approach could go wrong; I’d expect it would take an immense amount of fine-tuning even if it does end up looking plausible”. And if you say “One of those genes is p53,” I’d probably say “Oh, yeah, I guess that’s kind if clever in its way but my inclinations that it would be exceptionally tricky at best if anything are increased (though maybe in fairness they ought to stay the same)”. Senescence is a big complicated thing from what I know of it and you might get all kinds of interesting and unpleasant results from attempting to nuke all senescent cells as determined by expression of just two genes.
As for my fully general counter-argument, yes, that’s what it is. It’s something I think anyone who seems inclined to get excited enough by one mouse model survival plot to wonder if it’s “the next big thing” might as well hear. It’s preliminary data (experiment not yet complete) in an early proof of concept in a mouse model (maybe I missed it in the slideshow but I couldn’t even find an n for the experiment). Those are if not a dime a dozen, well … I wouldn’t hold my breath. Not that they shouldn’t keep pursuing it, but it’s really far from enough information to be able to judge whether it has a particularly good shot at being a game changer. Anyway if I were to get excited about anything in longevity research I’d focus on the naked mole rat people. Once they rule out some stuff there might be really interesting mechanisms indicated to go after. But mostly it’s personal bias on my part because naked mole rats are cool and I’d just rather read about them.
Glancing at the slide deck they link to at the bottom of that article, I’d be skeptical. Oisin does look to have a legitimately impressive gene therapy platform (chemically-inducible suicide genes, expressed in specific tissues by using different promoters), but they run afoul of the same limit that kneecap basically all gene therapies, CRISPR included: we have some incredible genetic tools but no good way to get them into the tissues of living adults safely, efficiently and specifically.
By way of illustration, we’ve had the ability to clone any transgene, driven by any promoter, into any cell since, conservatively, the 1980s. That should have way more sci-fi potential than targeted deletions a la CRISPR – you’re actually knocking in a completely novel, foreign gene – but the reason I don’t currently have green fluorescent hair, or a butterfly photoreceptor that lets me see in the near UV, is that the only way to inject these genetic payloads into living tissue are a few fairly crappy viral vectors. Crappy because these have very low efficiency (the vast majority of your target cells will not receive the modification), very limited ability to target specific tissues or cell types, and they tend to induce immune responses that prohibit repeat dosing.
This is why the idea of shooting suicide genes into tumors has been kicking around for decades, but no one’s made any headway on it AFAIK. The few potential gene therapy successes thus far have mostly been in areas where transfecting a handful of cells with a one-time dose is sufficient for the desired effect; for example, cloning some antiviral antibody into a handful of muscle cells in the bicep can be sufficient to generate protective levels of that antibody in circulation. Oisin sidesteps this whole problem by modifying their mice at the germline so that every cell in the mouse contains the transgene, but that’s not feasible in humans for reasons I’ll leave as an exercise for the reader.
TLDR: in gene therapy, we have the genetic equivalent of thermonuclear warheads, but our delivery systems are equivalent to rickety old V2s.
Oh, I remembered another case where gene therapy can work in humans: when you can remove the target tissue, do your genetic manipulations in the lab, then pop the modified tissue back into the patient. The signal example of this right now is chimeric antigen receptor T cell (CAR-T) therapy where you suck some circulating immune cells out of the blood of a cancer patient, engineer them to express an anti-cancer receptor and transfuse them back in. Something like this is feasible for “tissues” that circulate in the blood as single cells, but doesn’t readily generalize to, say, a pancreas.
I’d say the most exciting current type of treatment is in precision medicine. Last year’s news at ASCO about larotrectinib was incredible. As someone who worked on those trials, I can say it felt like the future of cancer treatment. The only problem, of course, is that finding a drug that treats <1% of all cancers (but treats them really well!) is slow progress indeed. The hope for this approach is that we accumulate dozens of these types of drugs, each targeting a small percent of cancer patients, but each targeting a mutation that drives that specific tumor. This will likely take at least 20 years – even considering that many pharmaceutical companies are rushing to get treatments to market that are based on treating patients with a specific genetic marker, similar to larotrectinib.
Say this is moderately successful. Twenty years from now, after running some tests, your doctor tells you that spot they detected on your CT scan was cancer. They already sent out the biopsy for NGS testing, and it turns out you have three mutations for which we have effective drugs that target them. They skip the chemo and start you on a cocktail of all three drugs, hoping to catch the whole cancer in the same way you might lay down multiple herbicides in a field. Combined, the side effects of these drugs are easier to deal with than chemo, so it doesn't lay you up for weeks on end. You take them for a couple of months, your cancer goes away, and maybe MAYBE we start using words like "cure".
But there's no cover of Time magazine for this long-term gradual approach. Slowly, fewer and fewer people have to go through chemotherapy. More people get cancer and not only don't they die, it doesn't represent some major life-changing experience for them.
And maybe some day our children grow up in a world where they don't understand why cancer was so scary to us.
Or maybe larotrectinib is a fluke that's replicated in one or two other targets, but we mostly don't see any major advances using genetic approaches. Such is the nature of cancer research.
My father was diagnosed with stage IV lung cancer last September and had leptomeningeal carcinomatosis at presentation. I went through and read as many medical journal articles to understand what to expect and each started:
“Leptomeningeal carcinomatosis (LMC) is a dismal terminal stage disease of solid cancer that is devastating to the patient.”
Up until recently, treatment was either extremely invasive chemo administered through a lumbar puncture, installing an ommaya reservoir directly into his skull or palliative care that had a median survival rate of 4-6 weeks. Not only was he likely to die soon, his quality of life would be seriously affected by the treatment.
Instead, he has an EGFR Exon 19 deletion and we started on afatinib immediately. He is maintaining a high quality of life and the symptom that brought him to the hospital, resting oxygen below 80%, has returned to 97%.
I know that a mutation will arise and maybe osimertinib will be given if it is T790M. If not we will return to a tough reality. But I strongly agree.
” there’s no cover of Time magazine for this long-term gradual approach. Slowly, fewer and fewer people have to go through chemotherapy.”
This extra time has let him plan for succession in his law firm, craft a will and transition plan for his illiquid assets and see me get married last May.
He will not be cured, he will die from this disease within 5 years of diagnosis almost guaranteed. Yet he has already lived much longer than he would have if he were diagnosed before 2004 (first line TKIs were approved then) and, if we are lucky enough, osimertinib will extend his survival well beyond what we could expect if he were diagnosed before 2017. Eventually some very smart team will find another treatment that stacks with TKIs in EGFR+ patients and your future will be true for this subset of cancer.
I find your discussion of these biases very cogent and up to date. And these analyses are probably the best way of estimating how good we are at rolling out and scaling improved methods. But what about RCTs? I mean I expect this literature to have its own set of problems with nonreplications, publication bias, etc. But at least you don’t get the lead-time bias. And I guess dead people are dead people, so maybe less room for mischief than in psychiatry.
There have been RCTs of each individual cancer therapy that shows it works as well as or better than the older cancer therapy, but this is less of a knock-down proof than you’d think. After all, most things in health care are confirmed to work by RCT, but it’s surprisingly hard to find a positive effect for health care in general (see eg Robin Hanson’s writings on RAND). So it’s good to have confirmation.
It would also be hard to calculate society-wide magnitude of progress from RCTs.
Knockdown argument, haha, as if..
Of course every approved treatment worked in some trial, but you might see diminishing returns in terms of effect sizes or number of successful trials. Or not, and of course there is tremendous potential for bias. It just seems interesting to compare and contrast. If anyone has some lit that did this, I’d be keen to hear.
In a perfect world, we’d learn whether we should redouble efforts to train doctors in new methods or in discovering new approaches. I guess comparisons across health care systems get you some of that.
How would one go about determining the probability of more or less curing cancer by 2050?
My mother and maternal uncle were prolymphocytic T-cell leukemia patients, so the issue of advancing cancer treatment hits close to home.
.. A general cure for cancer impllies a major breakthrough somewhere, and frankly, I would find it much more likely that we stumble on a general preventative for cancer than a cure (A drug or other intervention that make cancers less likely to start) But this is not the kind of thing you can put good numbers on. A specific type of cancer, sure, the people doing research on it probably have a sense of the odds. Cancer in general? Not so much.
Even a vaccine or drug that makes a specific type of cancer orders of magnitude less likely to form would be a huge deal, if researchers working on several different cancers each come up with one.
That’s the HPV vaccine, no?
That would be an example. One would hope for a high probability of more being invented.
First, rigorously define “more or less curing cancer by 2050”.
Then, make a estimate of the base rate of similarly difficult things by finding everything that is similarly difficult that has been intended, ans looking at what fraction of those things happened.
Then adjust for evidence, which in this case looks the same as adjusting your reference class: What fraction of things as difficult as more or less curing cancer that also got this much media attention/inflation-adjusted funding/other support happened?
Basically, the same way you would go about estimating the probability of any other event. The fact that it’s life or death to you is utterly irrelevant to the math.
Laryngeal cancer getting nastier and harder to treat–hmm, it seems to me like HPV has taken over tobacco as the main driver of oropharyngeal malignancies, and maybe it messes with cellular DNA more severely than tobacco does. HPV is very likely the source of increasing colorectal cancers in young adults as well.
Maybe they need to start having sex that conforms more to natural law to escape cancer.
There are six comments on this post about cancer, and two of them are you trying to pick fights about culture war topics. Consider yourself warned.
I read the red text in Uriel-voice, and I’m okay with that
Which natural law is lesbianism?
It’s kinda uncool to engage with someone after they’ve gotten a warning.
I honestly read the initial comment as ironic. Do they have a background to lead us to assume they weren’t making a quip?
It’s absolutely a quip; a quip that LMC can’t respond to without threat of banning. That’s why it’s uncool. It’s like kicking someone while they’re down.
@lazydragonboy
At best, it’s “haha only serious”. I am fairly sure that LMC does disapprove of non-heterosexual sex.
@Nornagest
Eh, it might not be particularly honourable but honour isn’t real. I don’t think I harmed LMC any more than they harmed any gay readers, or dealt significant damage to the comment section’s cultural norms. Also, I think you misread lazydragonboy’s comment — they thought LMC’s comment was ironic.
Actually HPV-associated head and neck cancer has better survival rates than smoking-associated head and neck cancer. This is an extremely well-replicated finding, eg https://jamanetwork.com/journals/jamaotolaryngology/article-abstract/2662647
I think that the reason for a signal of decreased survival in laryngeal cancer (a type of head and neck cancer), is most likely due to the same trends that led to increased overall cancer rates up to 1990: increased rates of smoking. Alcohol may play a role too. If this is true then it should improve shortly (or may have already been improving over the past decade or so).
None of this is to deny the major role that HPV plays in the development of deadly head and neck cancers, or the critical need to vaccinate young people of both sexes and to develop better screening/treatment strategies for HPV-associated head and neck cancer.
Then, if that is so–this development about laryngeal cancer *really* makes no sense!
Laryngeal cancer is anatomically distinct from oropharyngeal cancer, so there is a confusion in terms here.
Medical oncologist here. HPV related oropharyngeal cancer patients do way better compared to the alcohol/tobacco related ones, possibly related in part to the fact that the people who get them are healthier. HPV associated with anal cancer but not so much colorectal, as far as I know.
This sort of thing makes me suspect that belief in the Singularity is an emotional response to mundane technological progress slowing down. We can’t invent medical nanomachines that hunt and kill cancer cells? Well, the Singularity AI could!
Nice Bulverism, but early 2000s singularitarianism was closely intertwined with the belief that technological progress was increasing superexponentially so a singularity would have to happen soon. Ray Kurzweil and his graphs were the worst offenders, but this was something like half the movement and I think still is pretty influential even though I rarely meet those people anymore.
Yeah, I know about Ray Kurzweil and his graphs back to the Paleolithic.
The timeline of this stuff was a bit of a blur to me. It’s funny that “technological progress is increasing superexponentially” was a belief that spread around the same time as the Supersonic Transport was retired with no replacement, which was two years after the widespread disenchantment with science fiction and futurism that I DO remember from 2001. Adults were talking about how it was improbable that there would be manned interplanetary travel before they died, when it was “supposed” to happen by then. Avery Brooks from Star Trek did a TV commercial for I forget what that captured the “Where’s my flying car?” zeitgeist in those exactly words.
Fantasy became the mass media escapism of choice at SF’s expense.
And the Kurzweil era of singularitarianism was happening at this exact time!
Avery Brooks from Star Trek did a TV commercial for I forget what that captured the “Where’s my flying car?” zeitgeist in those exactly words.
IBM Lotus Software. (Some of the comments there are amusing.)
If we’re playing Bulverism like that, I’ll be more specific: it’s an emotional response to mundane technological progress slowing down everywhere except with computers. Thus, people appeal to future even-more-advanced computers to fix all the shortcomings elsewhere.
But mundane technical progress is not at all restricted to computers. I suppose you could try to argue that the postal service, telephones, books, TVs, radios and playback of recorded media have all “turned into” computers, but that seems a bit disingenuous, given that watching TV or a movie is still watching TV or a movie, but far improved now in every respect over the 1980s. But well outside of that you can look at, say, lighting technology, now providing brighter lights at a fraction of the power consumption and maintenance effort, and even allowing us to change the hue at will, remotely. And certainly device lifetime on batteries for a given weight has increased dramatically in the last couple of decades, even if that is more to do with the things using them needing less power than the (smaller) improvements to battery technology.
Maybe part of the problem is just that the changes are different from the ones we expected. Almost nobody anticipated ubiquitous networking, which I would take over flying cars any day even at the cost of now wincing every time I see someone use a videophone booth (2001) or physical media in older SF stories.
Telecom, entertainment electronics, and computers. Lighting… meh. We’ve got LEDs now, I liked incandescents better. Transportation is worse. Medical is fractionally better for massively increased price.
Residential buildings have gotten lower quality for higher price (the advances in technology have allowed the substitution of cheaper materials for higher priced materials; in most cases the cheaper materials are only almost as good and overall price increases have more than wiped out the savings).
Household appliances have not gotten any better; they’ve either gotten worse by government fiat (washing machines, toilets, dishwashers, lawnmowers), not changed (stoves, vacuums), or gotten more efficient but not more useful (refrigerators). Where’s Rosie the Robot or her non-humanoid equivalents?
Clothing has gotten cheaper but wears out faster; the exception here is certain outdoor clothing which actually has gotten better.
Weapons may have gotten better but governments won’t let people have the good ones. (hey, where’s my lightsaber, blaster, or vibro-blade?)
Well, if you like flashlights four or five times the size that put out less light and don’t last a quarter as long, you’re welcome to your old incandescent ones. And if you like bulbs that last a few months rather than a half dozen or more years, and use far more power, you’re welcome to the household incandescents, too. Objectively, however, the currently available LED lights, available in a wide range of colour temperatures, are far better.
And how on earth has transportation gotten worse? Every bus stop where I live now has a display showing the arrival times of the next buses and their current actual (not scheduled) distance from the stop, the buses load faster, are slightly cheaper and transfers are much easier because of the cards, and we have free WiFi Internet access during the trip. Cars are safer, use less fuel, have navigation systems better than what military aircraft had forty years ago, and are well on the way to driving themselves.
And household appliances have certainly gotten better. Something as basic as a rice cooker or pressure cooker works noticeably better and more easily now that they use microcontrollers, and we now have appliances such as automated bread makers that didn’t even exist forty years ago.
Fifteen year old apartments are certainly nicer than my 35-year-old one, but I’ve not looked into this area much beyond that. Do you have any evidence building an apartment or house today with older technology would be cheaper than doing it with new technology of the same quality, though? I find it difficult to believe that modern technology and building techniques are going to make it more expensive to build something.
LEDs simply have a poorer spectrum than incandescents. All the rest is traded off against that.
Buses still arrive late and three at a time (or full and bypassing your stop). Knowing that they’re doing this isn’t an improvement in transportation. And they take longer to load because of the handicapped requirements (it takes time for the bus to “kneel” and lift back up).
Cars have more bells and whistles, but they don’t get you there any sooner.
If you want a faster car, they certainly exist. For instance, there’s the Bugatti Veyron, top speed 253 mph. But if you bought one, you’d discover that you can’t actually make use of that speed on a crowded highway. “Getting there faster” is a traffic problem, not a car design problem.
Household appliances have similar issues – no matter how hot your stove is, the steak that you’re cooking on it hasn’t changed, and that’s what determines things like “how long your stove takes to cook a steak.” There are some cool counterexamples like molecular gastronomy, but for the most part, the food we eat hasn’t changed, and changing that would be a biology problem, not a stove design problem.
Basically, some problems are outside the scope of a single gadget to resolve. It’s like arguing that kitchen technology has worsened because your new non-stick skillet can’t cook a meal for 20 people in the same time you used to cook for 4.
And it’s a problem for which negative progress has been made in recent times. Trains and planes and cars, all slower. I didn’t ever say it was a car design problem.
There are plenty of potential improvements in cooking without speeding up the actual cook time. Right now if I want food, I have to remove the raw ingredients from the refrigerator, chop, season, stir, etc. Like I said, I want Jetsons-equivalent functionaility. I pick a recipe, N minutes later I get a plate of food, where N is about the time it would take me to make it. We’ve made exactly zero progress towards that. Then I have to clean up…. again, lots of room for improvement, none accomplished.
The answer is that a computer that can do roughly the same number of calculations as a human brain still costs approximately $600,000. Add in machine vision, good tactile control, and with the whole kit powered by batteries, and the cost would way more than hiring a human maid.
The “cancer will be cured in five years” thing is why I, being older and remembering all these kinds of promises that in
fivetenokay twenty for sure! years time we’d have all these advances and be living on the Moon with our flying cars, am so laid back about things like Argh AI Threat and Argh Climate Change and Argh Latest Flap.It may happen, but it’ll happen much more gradually and in a different way than expected. Re: the point about disenchantment, I think it’s because we’re living now in the Far-Flung World of the 21st Century and while we do have incredible advances in things we never imagined, it’s because it hasn’t turned out as we imagined and expected (Mars colonies, tourism on the Moon, aliens and robots) that we are so disillusioned. And that ties in with the other thing: maybe Fairy Godmother AI will come, but not in the way or the form we expect it, and there won’t be medical nanobots and the like because that’s probably not doable.
Nuclear fusion, really good solar cells, really good batteries, cancer cures, aging cures, obesity cures, artificial intelligence, etc… there’s a lot of things we’ve been expecting for years and just haven’t happened. File it under “Where’s my flying car?”
There’s been progress in some of these (solar and batteries, for instance), but there was just so far to go that it seems disappointing. In some things we’ve retrogressed — not only are there no flying cars, but transportation has gotten slower both in the air and on the ground.
It’s good that cancer (once the smoking signal is removed) seems to be in the category of “things making disappointingly slow progress” rather than “retrogressing”, but it’s still disappointing.
“Transportation has gotten slower both in the air and on the ground”
I definitely agree that transportation has gotten slower in the US, and it’s very plausible to me that it’s gotten slower in the air globally, but does “slower on the ground” hold throughout the developed world or only in certain countries?
Transportation is unusually susceptible to government policy changes, not just technological changes, and policies are far from uniform, especially for ground transit.
I figure this was The Nybbler referencing the US’s non-adoption of high-speed rail.
That ambiguous “we” is a powerful cheat.
Peter Thiel makes a pretty good argument that progress has stalled in a lot of meatspace arenas even as it has gone nearly parabolic in the new field of computers.
Air travel has got much cheaper though, maybe not in the US but in Europe low-cost airlines are at least an order of magnitude cheaper than the traditional airlines of decades ago.
Trains got faster and cheaper, again maybe not in the US, but this seems to be a single country problem (it’s because Americans love cars too much?)
“This sort of thing makes me suspect that belief in the Singularity is an emotional response to mundane technological progress slowing down.”
Using a human brain at 20 petaflops (per Ray Kurzweil), the total number of human brain equivalents (HBEs) represented by all the world’s microprocessors was and will be:
2010: 50,000 HBEs
2020: 30 million HBEs
2030: 12 billion HBEs
2040: 10 trillion HBEs
http://markbahner.typepad.com/random_thoughts/2016/02/recalculating-worldwide-computing-power.html
That’s why you haven’t seen any evidence of a coming Singularity. Wait for…maybe 7-15 years…and you will. Or 25 years at the outside.